

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Transradial approach has been preferred for coronary angiography (CAG) and percutaneous coronary intervention (PCI) due to several advantages, including decreased associated vascular complication, patients' convenience, and early ambulation compared with transfemoral approach.1)2)3)4) With these advantages, current guidelines support that radial access is recommended for CAG and PCI in acute myocardial infarction (AMI) patients with and without ST-elevation if performed by an experienced radial operator.5)6) Regarding the access site selection of radial artery (RA), most operators commonly use the right radial approach because the left radial approach increase operator discomfort during vascular access and procedure, especially in obese patients.3)6) However, the left radial approach has potential benefits for the patient and operator as well. Firstly, the left radial approach is associated with lower fluoroscopy time compared with the right radial approach.8)9) It may also lead to less exposure radiation for the patient and operators. Secondly, subclavian tortuosity was more frequent in the right radial approach compared with the left radial approach.10)11) Therefore, the catheter via right radial approach has to bend sharply into the ascending aorta through the right brachiocephalic trunk, which may lead to disrupting atherosclerotic plaques with subsequent embolization.12) Longer duration of CAG via the right radial approach by the subclavian tortuosity can also contribute an additional embolic source. Thirdly, the inexperienced operator should consider the left radial approach because a learning curve is shorter than the right radial approach.8) However, actually more operators still prefer the right radial approach due to greater physical comfort despite various benefits of the left radial approach.
The left distal radial approach, called snuffbox approach, can be an alternative option to choose the left radial approach without an uncomfortable position for the operator as the left hand of patients is naturally placed on the left or right groin area according to patient's body type, similar to transfemoral approach.13) However, the feasibility of CAG and PCI via snuffbox approach is still concerned due to the lack of data regarding the coronary procedure. One of the concerns is whether the diameter of the snuffbox RA is suitable for the conventional transradial sheath. In addition, there are few data regarding the feasibility of snuffbox RA puncture and coronary procedure via snuffbox approach. Therefore, the aim of the study was to compare the diameter of snuffbox and conventional RA and investigate the efficacy and safety of left snuffbox approach for CAG and PCI.
METHODS
Study population
We retrospective analyzed 150 patients who planned to perform CAG or PCI via left snuffbox approach for suspected myocardial ischemia from November 1, 2017 to March 31, 2018 at the Chonnam National University Hospital, Gwangju, Korea. During study period, single operator performed the left snuffbox approach in patients who only had normal pulse in the left snuffbox area. The study protocol was approved by the Institutional Review Board of Chonnam National University Hospital (approval number: 2018-078).
Position and preparation for left snuffbox approach
The patient places the left upper arm over a cushion and bends the elbow slightly so that the left hand is naturally located in the left groin site (Figure 1A) and the operator positions on the right side of the patient to prepare left snuffbox approach (Figure 1B). After local anesthesia on left anatomical snuffbox with 1 mL lidocaine hydrochloride using a 26 gauge needle, the puncture is performed using a 20 gauge needle with the through-and-through puncture technique. After successful puncture, 0.025-inch straight wire is inserted, followed by an insertion of the radial sheath (Radifocus® Introducer II; Terumo Corporation, Tokyo, Japan) (Figure 1C). After left snuffbox RA cannulation, a combination of 0.2 mg of nitroglycerin, 2.5 mg of verapamil, and 3,000 units of unfractionated heparin diluted in 10 mL of saline solution is administered to prevent arterial spasm in all patients except for those scheduled for ergonovine provocation test. After the procedure, hemostasis was obtained by compressive bandage with gauze for 2 to 3 hours (Figure 1D).

Comparison the diameter of left snuffbox and conventional RA
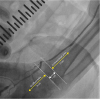
Among 150 patients enrolled in our study, left RA angiography was not able to try from 49 patients due to technical issues including very unstable punctured needle position. Therefore, RA angiography from hand to forearm was achieved only from 101 patients before injection nitroglycerin and verapamil (Figure 2). With our experience regarding left RA puncture, a hypothetical line was created between the styloid process of radius and top of the distal radioulnar joint on radius side and from there to proximal 1 cm was defined as the puncture free zone, which was not available for RA puncture. Based on the puncture free zone, an area which was within proximal and distal 3 cm, were defined as conventional and snuffbox area, respectively. In the 2 areas, the maximal RA diameter measurement was calculated by quantitative computed angiography (QCA). In addition, all of the left RA angiographic images were reanalyzed by 2 independent observers to investigate inter-observer agreement of snuffbox and conventional RA diameter measurement.
Data collection
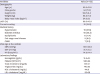
Demographics including age, gender, height, weight, body mass index, current smoking, medical history including hypertension, diabetes mellitus, dyslipidemia, end-stage renal disease, and coronary artery bypass surgery, and left ventricular ejection fraction on 2D echocardiography were collected. The patient's vital signs, including systolic blood pressure, diastolic blood pressure and heart rate were collected at the catheterization laboratory before performing CAG. Laboratory findings, including complete blood counts and lipid profiles, were measured during hospitalization. Data of coronary angiographic and procedural characteristics regarding the performance from left snuffbox approach were also recorded.
Statistical analysis
Categorical variables were reported as numbers with a percentage. Continuous variables were expressed as mean with standard deviation and analyzed using the paired t-test. Correlations were assessed using the Pearson's correlation coefficient, and the intraclass correlation coefficient was used to evaluate the consistency of inter-observer agreement of the maximal RA diameter measurement. Statistical data were considered significant when the p value <0.05. Statistical analysis was performed using SPSS 22.0 for Windows (SPSS-PC, Chicago, IL, USA).
RESULTS
The left snuffbox approach was tried in 150 patients during our study period. Although the successful puncture of left snuffbox RA was done in 140 patients (93.3% of the success rate of snuffbox puncture), an insertion of 0.025-inch straight wire (45 cm; Terumo Corporation) was failed in 8 cases due to tortuosity of snuffbox RA with vasospasm. Therefore, 132 were succeeded for the left snuffbox approach, defined as the success of cannulation via snuffbox RA by the radial sheath, and the success rate was 88.0% (Table 1).
Table 1
A success rate of the left snuffbox approach for patients undergoing coronary angiography or percutaneous coronary intervention between November 2017 and March 2018

| Coronary angiography via left snuffbox approach | Value (n=150) |
|---|---|
| Success rate of snuffbox puncture | 140 (93.3) |
| Success rate of cannulation via snuffbox approach | 132 (88.0) |
To compare the diameter of snuffbox and conventional RA, 101 left RA angiographies were analyzed using QCA. The maximal diameter of snuffbox RA was significantly smaller than conventional RA (2.57 mm vs. 2.72 mm, p<0.001) (Figure 3A). In the correlation analysis, there was a significant correlation between the maximal diameters in the left snuffbox and conventional RA (r=0.856, p<0.001) (Figure 3B). Regarding inter-observer agreement, the intraclass correlation coefficient values for the measurements of snuffbox and conventional RA were 0.955 and 0.958, respectively, demonstrating excellent inter-observer measurement consistency (Supplementary Table 1).
Figure 3
The maximal diameter in the snuffbox and conventional radial artery (A) and the correlation of the maximal diameter between the snuffbox and conventional radial artery (B).
RA = radial artery.

The baseline characteristics for 132 patients undergoing successful CAG via left snuffbox approach are summarized in Table 2. The average age of patients was 65.9 years and 71.2% were male. The body mass index was 24.6 kg/m2 and left ventricular ejection fraction was 60.9%. Regarding medical history, 9 (6.8%) patients had the end-stage renal disease with hemodialysis through arteriovenous (AV) fistula on right arm and 7 (5.3%) patients had a history of coronary-artery bypass surgery.
Table 2
Demographics and clinical characteristics for 132 patients undergoing successful coronary angiography via left snuffbox approach
The coronary angiographic characteristics of patients with successful left snuffbox approach are presented in Table 3. A total of 2 (1.5%) patients underwent emergency CAG for ST-segment elevation myocardial infarction (STEMI), 56 (42.4%) patients presented with non-ST-segment elevation acute coronary syndrome (NSTE-ACS, including unstable angina), and 74 (56.1%) patients underwent angiography due to the investigation for coronary artery disease. In all 132 (100%) patients, 6 French (Fr) sheath were used and the success rate of CAG via left snuffbox approach was 100% (n=132). For evaluation of variant angina, ergonovine provocation test was performed in 4 (3.0%) patients and an assessment of left internal mammary artery (LIMA) was done in 7 (5.3%) patients. Regarding diagnostic catheter for CAG, 5 Fr Judkins type catheter (Vista Brite Tip®; Cordis, Miami, FL, USA) was used for the left or right CAG in most patients. In addition, 5 Fr Tiger-II catheter (Terumo Corporation) was used for a single-catheter technique in 18 cases.
Table 3
Characteristics of coronary angiography in patients undergoing successful coronary angiography via left snuffbox approach

The characteristics of successful PCI via left snuffbox approach are summarized in Table 4. PCI via snuffbox approach was successful in 41 (97.6%) of 42 patients and 1 patient failed to PCI via snuffbox approach due to severe angulated calcified lesion in the left circumflex artery. A total of 25 (61.0%) patients underwent PCI for AMI including 2 cases of STEMI. The most frequently treated vessel was the left anterior descending artery (n=19, 42.2%) and 1 case for left main (LM) disease was included. Most patients were treated by stent implantation (n=39, 95.1%). Functional assessment by fractional flow reserve (FFR) wire was performed in 7 (17.1%) patients and intravascular imaging-guided PCI was done in 8 (19.5%) patients, including 6 of optical coherence tomography (OCT) and 2 of intravascular ultrasound (IVUS) guidance. Multi-vessel PCI was performed in 4 (9.8%) patients. Regarding vascular complication, forearm swelling with bruising, not requiring surgery or transfusion, occurred in 2 (4.9%) cases. In terms of the guiding catheter for PCI, extra backup type catheter (RunWayTM; Boston Scientific, Natick, MA, USA) was used for PCI for the left coronary system in 21 of 31 cases. For treatment of the right coronary artery lesion in 13 cases, Amplatz right type catheter (Mach1TM; Boston Scientific) was used in 11 cases.
Table 4
Procedural characteristics in 41 patients undergoing successful PCI via left snuffbox approach

Data expressed as number (%).
AMI = acute myocardial infarction; AR = Amplatz right; EBU = extra backup; FFR = fractional flow reserve; IVUS = intravascular ultrasound; JL = Judkins left; LM = left main; LAD = left anterior descending artery; LCx = left circumflex artery; OCT = optical coherence tomography; PCI = percutaneous coronary intervention; RCA = right coronary artery.
DISCUSSION
In this study of patients undergoing CAG or PCI via left snuffbox approach, we found that the success rate of cannulation via snuffbox approach was 88.0%, even though the success rate of snuffbox puncture was 93.3%. Nevertheless, CAG via snuffbox approach by the 6 Fr sheath was successfully performed in all 132 patients, although the diameter of snuffbox RA was significantly smaller than conventional RA. In addition, PCI via snuffbox approach was successfully performed in 41 of 42 patients. There was no major vascular complication requiring surgery or transfusion.
Kiemeneij13) who firstly introduced the feasibility of the left snuffbox approach for CAG or PCI reported that the success rate of the snuffbox approach was 89% (n=62) in total 70 patients. He failed arterial cannulation in 8 cases, 4 cases of them were in difficulty of wiring. We also experienced that wire advancement failure into the proximal RA in 8 patients among 140 patients with successful snuffbox puncture. In these cases, left RA angiography confirmed that the tortuosity of snuffbox RA with vasospasm. Therefore, we tried wiring using 0.018-inch stainless steel wire with a soft, flexible proximal part and a rigid distal part (Nitinol wire, Micropuncture® Introducer Set; Cook Medical, Bloomington, IN, USA), instead of 0.025-inch straight wire (Figure 4). Soydan and Akın14) reported that the left snuffbox access with the 0.018-inch stainless steel wire was successfully advanced in all 54 study patients. Thus, the use of 0.018-inch wire would be a solution if there is the difficulty of wiring after successful snuffbox puncture.
Figure 4
The left radial artery angiography demonstrating the tortuosity of snuffbox radial artery with spasm (A) and successful wiring into the proximal radial artery using 0.018-inch stainless steel wire (B).

Regarding the RA diameter, QCA measurement demonstrated that the snuffbox RA had significantly smaller diameter than the conventional RA diameter. However, CAG was performed via 6 Fr sheath in all 132 patients who had successful cannulation. The 6 Fr sheath was also used in 105 of 106 patients from the recent 2 studies, although the 6 Fr sheath was used in about half of the patients in the early experience of snuffbox approach from Kiemeneij.13)14)15) The use of the 6 Fr sheath enables to perform PCI via snuffbox approach as same as the conventional transradial approach, such as the physiologic assessment with FFR, intravascular image-guided PCI, and multi-vessel PCI using the various guiding catheters in the patients as shown in Table 4. With our experience, we reported the feasibility of the IVUS-guided PCI for LM disease via snuffbox approach.16)
Our study observed that CAG was performed in all 132 patients who underwent successful left snuffbox approach. Furthermore, among 42 patients who needed to perform PCI, only 1 patient changed into the right femoral approach due to a severe angulated calcified lesion in the left circumflex artery. In the meta-analysis regarding comparing the right and left radial approach for coronary procedures in total 3,210 patients, the left radial approach is superior to right radial approach regarding access site failure leading to crossover to femoral access.17) Park et al.18) also observed that the left radial approach had a lower incidence of access site change than the right radial approach. Furthermore, several studies have shown a higher incidence of right subclavian tortuosity, reported as one of the main predictors for transradial failure, especially in the elderly patients.9)10)19) Therefore, the left snuffbox approach may be an alternative approach for the elderly patients.
In our study population, 9 patients with the end-stage renal disease with hemodialysis through AV fistula were enrolled and a coronary procedure was successfully performed in those patients (CAG in 9 and PCI with CAG in 2 cases). In daily practice, the use of radial access in those patients has been concerned as a preservation of RA for AV fistula creation.20) Snuffbox approach is also beneficial for patients who have to perform CAG or PCI by the femoral approach, such as patients with the end-stage renal disease or chronic kidney disease who need to protect RA for AV fistula.
Regarding vascular complication, there was no complication in 80 patients who underwent only CAG, even though they took periprocedural antiplatelet, including aspirin and P2Y12 receptor inhibitors, over 95% (Supplementary Table 2). Only 2 patients had post-interventional forearm swelling with bruising, not requiring transfusion, in all 41 patients who had medication of aspirin and P2Y12 receptor inhibitors, including 4 patients with taking an oral anticoagulant (Supplementary Table 3). In the previous studies regarding snuffbox approach, no major vascular bleeding was observed.13)14)15) Therefore, snuffbox approach could be considered for alternative access site in patients with high bleeding risk.
There were several limitations in the present study. Firstly, this study was a single-center study with the limitations of a small number. Secondly, all snuffbox approach was performed by a single experienced radial operator. Therefore, some selection bias might have influenced the results and our results cannot be generalized. Thirdly, regarding QCA of RA, we did not consider arterial spasm even though puncture-induced arterial spasm was occurred in many cases. Alternatively, maximal RA diameter was analyzed in both arteries to prevent from bias by spasm. Fourthly, vascular complications were only evaluated during hospitalization. Fifthly, we did not evaluate pain grade at access site during the procedure. Sixthly, this study did not have the control group to test the hypothesis. Seventhly, pulse examination or ultrasonogram was not performed to evaluate RA occlusion after snuffbox approach. Nevertheless, our study might be meaningful to understand the possibility of the new access technique, snuffbox approach, for the physician.
In conclusion, left snuffbox approach is suitable for the alternative approach for CAG and PCI compared with the conventional radial approach. Further large, prospective, multicenter, randomized study regarding comparison with the conventional radial approach should be needed for evaluation of the feasibility of left snuffbox approach in details.
 XML Download
XML Download