

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Chronic subdural hematomas (CSHs) are generally regarded to be consequences of head trauma.717) The most commonly accepted pathophysiological explanation of CSH is that mild head trauma leads to tearing of bridging veins with subsequent bleeding, thus creating the hematoma.4) However, a history of trauma is absent in in about 30% to 50% of the cases, especially after the age of 65 years.15919) Besides trauma, alcohol abuse, seizures, cerebrospinal fluid (CSF) shunts, coagulopathies including therapeutic anticoagulant, have traditionally been considered as risk factors.717) Because of the continuing rise of life expectancy and the increasing use of anticoagulants, the incidence of CSH is expected to rise.21013) Current trends in an aging population predict that CSH will be the most common cranial surgical condition by the year 2030.3) Since the CSH is common in the aged and alcoholics, we presumed that they forgot the trauma. A customer subscribed to Disaster agencies insurance can receive payout twice to five times, when he said the cause was trauma. If the customers subscribed to a Sickness rider insurance, payout would be only a fifth to half of the former at the same situation. What shall we do, when a customer requires to change the International Classification of Diseases, 10th revision code to get the insurance payout? Although causality and apportionment of trauma is an important issue in CSH, especially in the insurance, it is too obscure to solve all struggles.
Comprehensive analysis on the etiology of a certain case of CSH may lack objectivity, even though the assumption is correct. A scoring system using risk factors may provide the possibility more objectively and quantitatively. We made a design to evaluate the apportionment of trauma in CSH. We also evaluated the usability of this score.
Go to : 
Materials and Methods
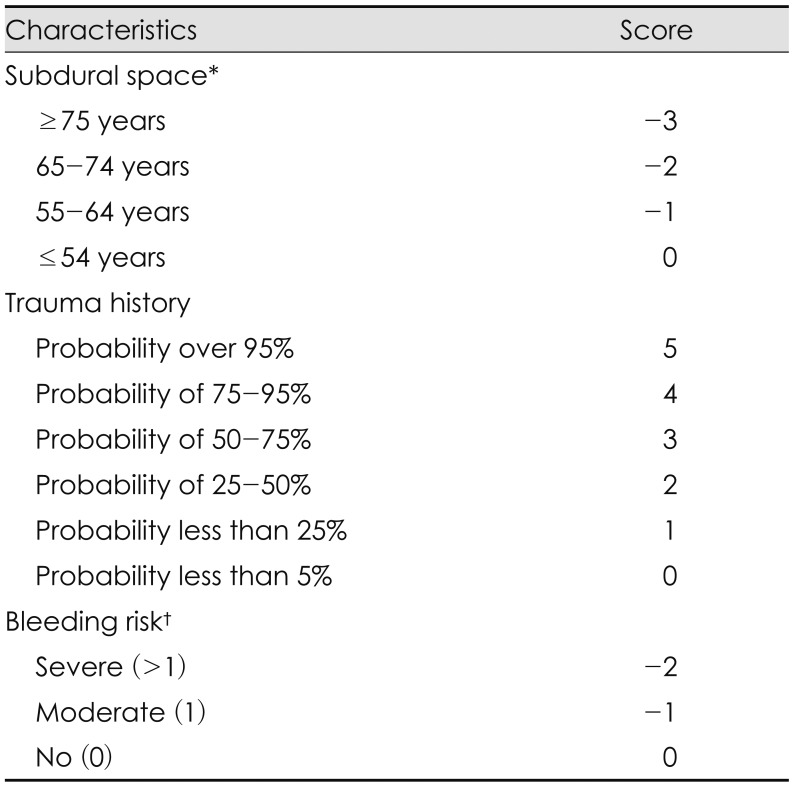
There are 3 key factors for production of CSH. The necessity of CSH is a potential subdural reservoir. Trauma and coagulopathy are important precipitating factors. We can assess the apportionment of trauma by comparing the relative importance of these three factors. This scoring method, so-called trauma apportionment score (TAS) for CSH, is consisted with three factors, such as subdural space, the history of trauma, and bleeding risk (Table 1). Potential subdural space, the essential factor for development of CSH, can be assessed by the age. If there is a definite cause of intracranial hypotension, such as CSF leakage, then we can add −1 on the subdural space score. The trauma score can be assessed by trauma history. If there is a definite evidence or document of head injury, the trauma score is 5. The bleeding risk score is severe, if there were more than 1 risk factors. TAS, the sum of the Subdural space, Trauma and Bleeding risk scores, may range from −5 to 5. We applied this score to consecutive 200 patients (158 men and 42 women) with CSH. Patient recruitment started in January 2012 and ended in December 2015. There were 39 cases of recurrent CSH within the study period. They were counted in each, consisting 239 cases. CSH was confirmed by computed tomography (CT) and/or magnetic resonance imaging (MRI). We retrospectively examined the history of trauma, medication, and past history from the medical records of these patients. We also examined the laboratory results related to the bleeding risk.
Statistical analysis was performed using the χ2 test or Fisher's exact test. For the statistical significance, we grouped the age into either ‘not more than’ or ‘above’ 65. Differences were considered significant if the probability value was less than 0.05.
Go to :
Results
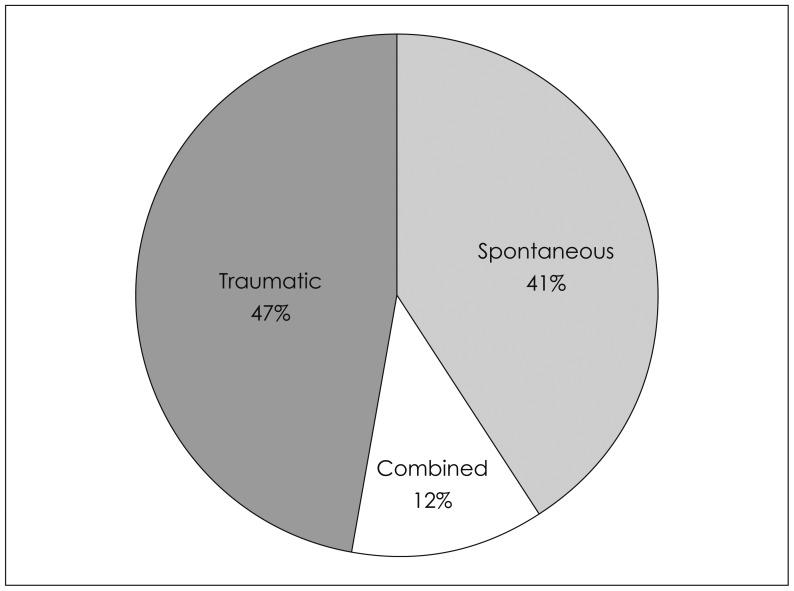
Actually TAS ranged from −5 to 5. The most common score was 0 (Table 2). TAS was positive in 112 cases, negative in 97 cases and 0 in 30 cases. If we defined the estimated cause was combined, when the TAS is −1 to 1, the cause of CSH was combined in 107 cases (Figure 1). If we defined the estimated cause was combined, when the TAS is 0, the cause of CSH was combined in 30 cases (Figure 2). In either criteria, traumatic CSHs were more common than spontaneous CSHs.
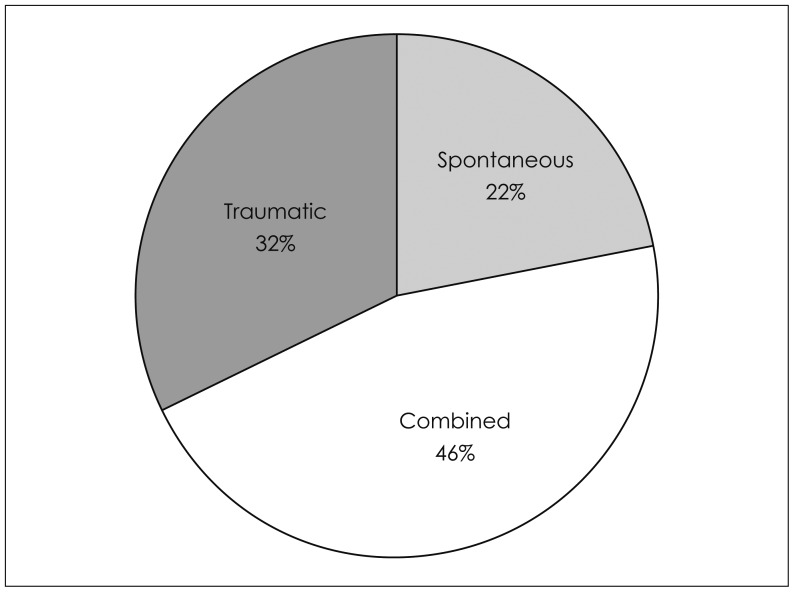 | FIGURE 1Distribution of the estimated causes of 239 cases of chronic subdural hematomas. When the trauma apportionment score is −1 to 1, the cause is regarded as combined. This extended criteria may be suitable for a legal judgment or an economical estimation.
|
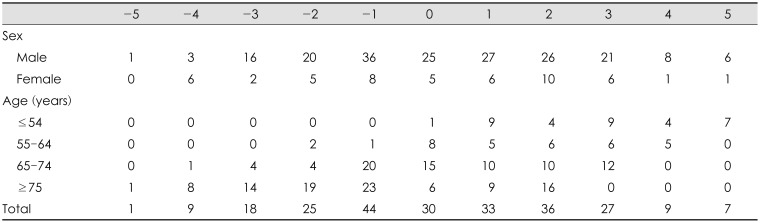
There was no sexual difference. However, there is a statistically significant difference in the age distribution (p<0.01, by Fisher's exact test). In either criteria, spontaneous CSHs were more common in the old age. We tried to illustrate 6 cases including TAS −5, 5, 0, the oldest, the youngest and a recurrent case.
Case 1
This 52 year old male patient visited our department with headache. He had a history of head injury about 3 months ago. He had a small acute subdural hematoma on the right side at that time (Figure 3B), which was resolved without surgery. He had no history or evidence of coagulopathy. CT scan on admission revealed a CSH on the left side (Figure 3A). The assessed TAS was 5 (Subdural space 0, Trauma 5, Bleeding risk 0).
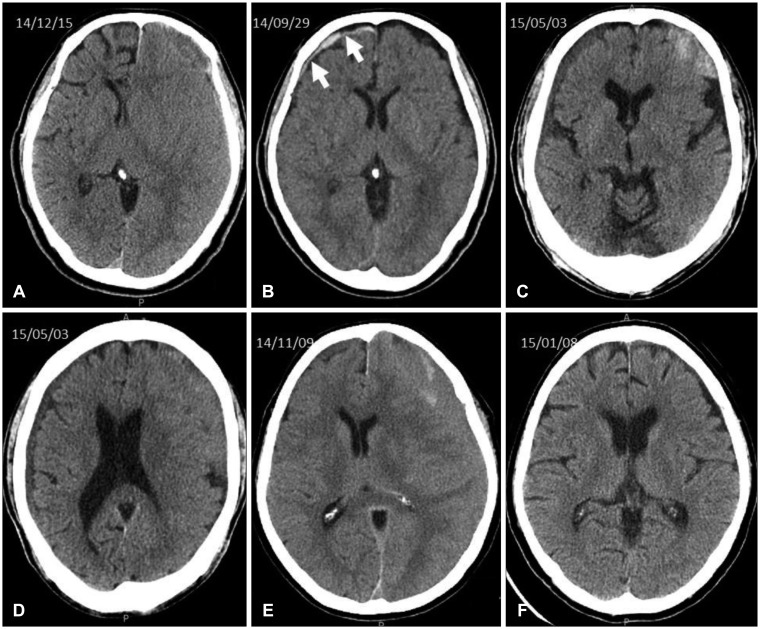 | FIGURE 3Computed tomography scans of Case 1 to 3. A chronic subdural hematoma (A) was developed on the opposite side of the acute subdural hematoma (B) after trauma in Case 1. Bilateral hematomas (C, D) were found in Case 2. Isodense chronic subdural hematoma on the left side (E) was resolved after a burr-hole drainage (F) in Case 3.
|
Case 2
This 80 year old male patient was admitted via emergency room with hemiparesis on the right side. He was suffered from atrial fibrillation, congestive heart failure, hypertension, and diabetes. He took warfarin. International normalized ratio was 2.43 on admission. He had no history of trauma. CT scan on admission revealed CSHs on both sides (Figure 3C and D). The assessed TAS was −5 (Subdural space −3, Trauma 0, Bleeding risk −2).
Case 3
This 76 year old female patient visited our department with general weakness and mental confusion for 2 days. She was suffered from hypertension and diabetes. She slipped down in the bathroom about 3 months before admission. She had no evidence of coagulopathy. CT scan on admission revealed a CSH on the left side (Figure 3E and F). The assessed TAS was 0 (Subdural space −3, Trauma 3, Bleeding risk 0).
Case 4
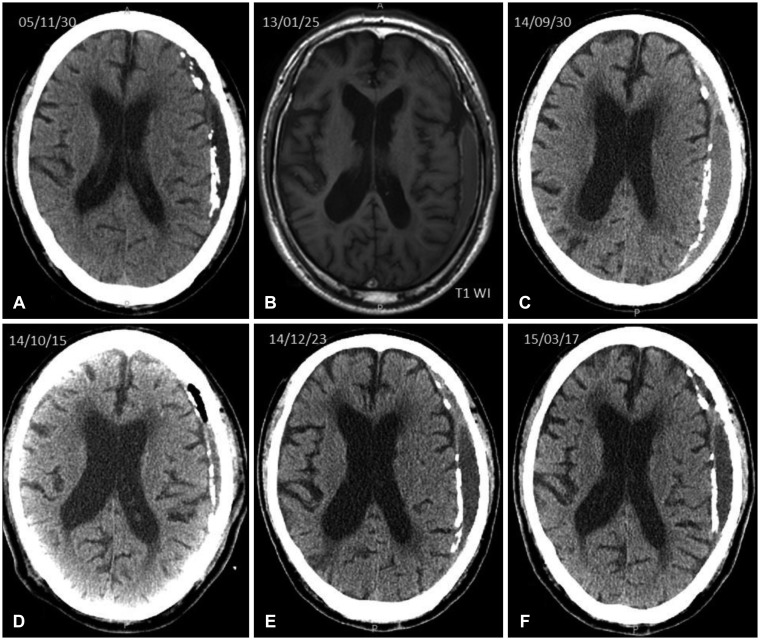
This 88 year old male patient was admitted to our hospital. He suffered from atrial fibrillation, coronary artery stenosis, hypertension, and dementia. He took aspirin and anticoagulants from 2004. He had no history of trauma. He had a long history of CSH. CT scan in 2005, about 10 years prior to admission revealed a CSH on the left side with partial calcification (Figure 4A), which was conservatively managed. In 2014, he was admitted to our department with general weakness and drowsy mentality for a week. A burr hole was made on October 14, 2014 (Figure 4D). There was steady improvement in symptoms. In March 2015, was admitted to department of neurology with decreased mentality and urinary incontinence. Although the CT on admission revealed CSH (Figure 4F), no specific treatment was done for the CSH. The assessed TAS was −4 (Subdural space −3, Trauma 0, Bleeding risk −1).
Case 5
This 37 year old male patient visited our department with pulsatile headache for 3 weeks. He had no history of trauma. He had no evidence of coagulopathy. CT scan on admission revealed a CSH on the left side (Figure 5A) with an arachnoid cyst on the same side (Figure 5B). The assessed TAS was −1 (Subdural space −1 due to a definite cause of intracranial hypotension, Trauma 0, Bleeding risk 0).
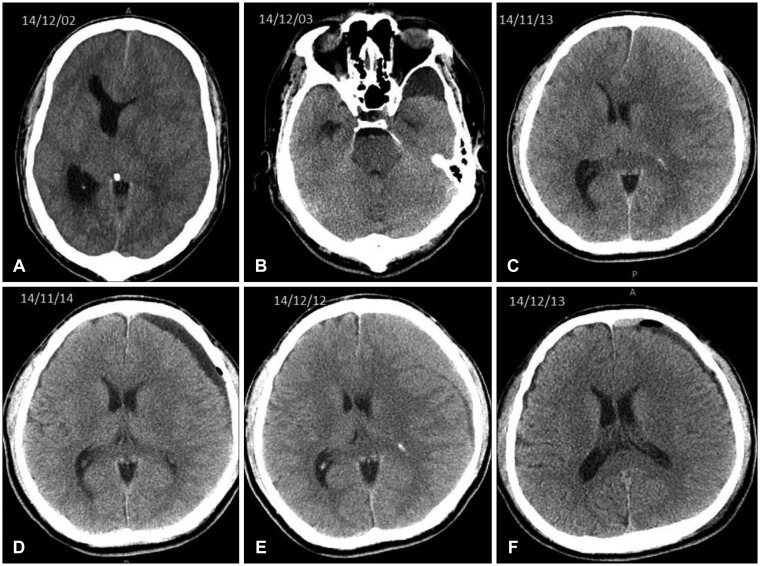 | FIGURE 5Computed tomography scans of Case 5 and 6. An arachnoid cyst on the left temporal pole (B) was noticed after burr-hole drainage of the chronic subdural hematoma on the same side (A) in Case 5. An isodense chronic subdural hematoma (C) were drained by a burr-hole (D) in Case 6. However, it recurred on the same side (E). The hematoma was resolved after a burr-hole drainage (F).
|
Case 6
This 52 year old male patient visited our department with severe headache for 3 days. He had no history of systemic illness. He had a history of direct hitting on his head about a month before admission. He had no evidence of coagulopathy. CT scan on admission revealed a CSH on the left side (Figure 5C). The assessed TAS was 3 (Subdural space 0, Trauma 3, Bleeding risk 0). He recovered after a burr-hole drainage (Figure 5D). He re-visited our department with severe headache for 4 days, 29 days after the first visit. He had no history of trauma and no evidence of coagulopathy at this time. CT scan on admission revealed a CSH on the same side (Figure 5E). At this time, the assessed TAS was 0 (Subdural space 0, Trauma 0, Bleeding risk 0).
Go to :
Discussion
TAS is a simple tool for quantitative assessment of the causality of a CSH. Since the pathophysiology of CSH is not yet clear,21) differentiation of the cause of CSH may be not easy. Actually the most common score was 0, which implies that the causality of a CSH is combined or obscure. By this narrow criteria, the cause of CSH was combined in 30 cases (12.6%). If we extend the criteria as −1 to 1, the cause of CSH was combined in 107 cases (44.8%). In either criteria, traumatic CSHs were more common than spontaneous CSHs.
We selected 3 key factors for production of CSH by a computerized search of the National Library of Medicine (PubMed) database of the up-to-date literature (published from 2010–2014). Sufficient subdural space, coagulopathy and trauma were three common causes of CSH. Although the number of papers did not have a value by itself, since papers did not have equal frequency or importance, it may represent relative importance or apportionment of certain factors.11) There are still many theories such as microbleed theory, anticoagulant and profibrinolytic theory, and inflammatory and growth factors theory,18) however the majority of CSHs are suspected by an undiagnosed trivial head injury. This assumption is hard to explain why CSH is rare in the young with severe head injury, while the majority of CSH occur in the old even without trauma.12) The origin of a CSH is multiple. It can be developed spontaneously, or changed from a subdural hygroma or an acute subdural hematoma. Although trauma may separate the dural border cell layer, a significant number of CSHs, often more than a half of cases, lacks any history of trauma.1516) A more important prerequisite is sufficient potential subdural space that is aging, degeneration of the brain. We cannot measure the subdural space accurately, since pre- or post- operative CT scans cannot represent the degree of atrophy. The age can be a reliable substitute of the subdural space, because the most common and universal cause of cerebral atrophy is the aging.22) Cross-sectional MRI studies of cortical thickness and volume have shown age effects on large areas of the brain.820) Spontaneous CSHs were more common in the old age, which means cerebral atrophy has an important role in development of CSH. When there was a definite evidence of trauma, such as CT scans or a medical documentation, the score for trauma history in Table 1 is definitely 5. However, frequently there was no hard evidences of trauma. Even in such cases, the doctor may choose any score of the trauma probability by the best estimation using comprehensive circumstances of all possible information.
In Case 1, the CSH occur on the opposite side of the acute subdural hematoma. Actually the origin of this CSH was not the acute one. However, the trauma initiated the development of CSH. In Case 6, the first CSH occurred after a definite history of trauma. However, the recurrent CSH occurred without any trauma, thus the recurrent CSH should be classified as a spontaneous one. If there is a sufficient potential subdural space, such as a severe brain atrophy and an evidence of coagulopathy, CSH can be non-traumatic even with a definite history of trauma.
At this time, we should answer whether CSH is a traumatic lesion or a degenerative lesion. CSH was regarded as a stroke in 17th century,6) changed as an inflammatory disease in 19th century, and became a traumatic lesion in 20th century.14) Modifying Virchow's description, CSH is sometimes traumatic, but most often caused by severe degeneration of the brain. Now, it would be reasonable that CSH is a degenerative lesion. In the insurance, a customer subscribed to Disaster agencies insurance would insist that the cause was trauma, to receive more payout. At this time, doctors should pay attention to seek the correct or the most probable cause of CSH. In this situation, TAS can be a useful tool.
TAS is simple and easy to apply. However, it was not designed by a quantitative estimation. Modification of factors may result misinterpretation. Although the cause may remain obscure in nearly a half of CSHs, the probability of misclassification would be low, when we use the extended (−1 to 1) criterion. TAS with a narrow criterion can be a useful tool for medical assessment. However, for a legal judgment or an economical estimation, the extended criterion would be suitable.
Go to :
 XML Download
XML Download