

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Traumatic optic neuropathy (TON) is an important cause of severe visual loss following blunt for penetrating head and facial trauma. To prevent a poor outcome, aggressive management is required. Treatment of TON is divided primarily into two categories: 1) high-dose steroid therapy; and 2) surgical decompression. Unfortunately, reliance on these approaches have been controversial, with a lack of evidence that steroids provide benefits over observation alone. Surgical management has been in the similar position regarding the benefits in improvement of visual acuity following TON.8,30)
However, optimal outcome following surgical decompression would be expected in the selected cases. Surgical decompression is performed by removing the bony fragments that impinges directly upon the nerve, or by decompressing the intra-canalicular optic nerve by removing structures surrounding the optic nerve.15) The transcranial approach can be used to decompress the optic nerve from the lateral-superior side of the optic canal (OC) and to decompress the nerve from the medial-inferior part of the OC via trans-nasal approach. In the large studies for TON that had been performed previously, neither medical treatment nor surgical treatment has shown to be a benefit to visual improvement.2026) However, research on optic nerve decompression (including direct TON) is ongoing, with many authors studying the optimal timing and surgical methods. TON is usually accompanied by head trauma. To treat TON complicated by traumatic brain injury, the neurosurgeon should possess knowledge and insight about appropriate surgical methods. In this article, we describe the current surgical strategy of TON, how to perform each method, and expected surgical outcomes.
Mechanism of Traumatic Optic Nerve Injury: Rationale for Surgical Decompression
Theoretically, direct TON is caused by direct damage of optic nerve, including optic nerve contusion, avulsion, laceration and is often accompanied by bony fracture around the optic nerve.19) On the other hand, indirect trauma has been reported to occur after blunt head trauma such as intraneural edema, hematoma, shearing of the optic nerve fibers, altered cerebrospinal fluid circulation, and impaired retroaxial transport of brain derived growth factors.26) Generally, it is not possible to directly measure the pressure on the optic nerve or in the OC after the occurrence of TON, but the status of optic nerve can be confirmed indirectly. According to longitudinal study that performed an analysis of optic nerve retinal nerve fiber layer (RNFL) thickness, circumpapillary RNFL and ganglion cell complexes (GCC) began to decrease starting two weeks after trauma and macular thickness decreased significantly after four weeks.18) Results of the study also suggest that treatment of TON should be performed within 20 weeks after trauma, since circumpapillary RNFL and GCC no longer change after 20 weeks. Because of these changes in the optic nerve, despite numerous reports that no significant differences in optic nerve are observed in TON following medical or surgical treatment, research continues to search for appropriate treatment methods.
Optimal Timing of Surgical Decompression
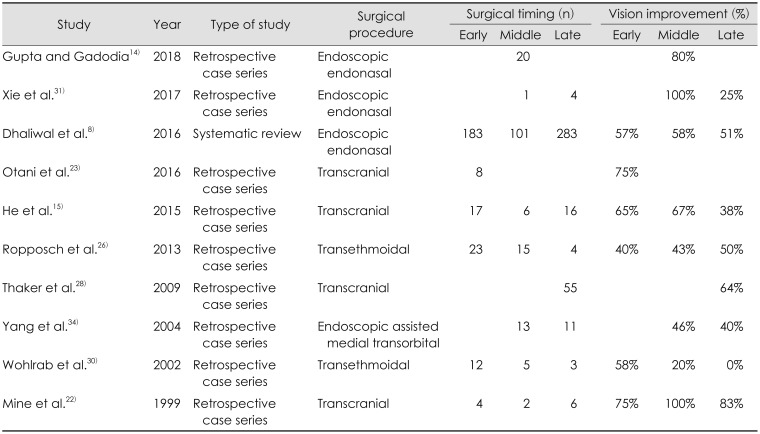
Although various studies have been investigating the optimal timing of intervention, large-scale prospective studies have not yet been conducted, and most authors have describing outcomes based on their own experiences. Emanuelli et al.11) reported surgery should be performed within 24 hours of steroids therapy. Wohlrab et al.30) reported that performing primary surgical decompression of the optic nerve within 48 hours of injury produced beneficial results. Many authors who performed optic nerve decompression described that it is better to perform surgery within three days. However, in a recent meta-analysis study of surgical timing, 57% in the early group (patients receiving surgery within <3 days) had visual improvement, while 51% in the late group (>7 days) alsoimproved.8) This suggests that delayed surgical intervention for TON is a better choice than not intervening at all without other treatments.
Indications and Contraindications of Surgery
Several authors who reported on optic nerve decompression surgery have presented the following indications for surgery: 1) History of traumatic face and head injury with and without OC injury;2333) 2) progressive loss of vision not associated with non-traumatic intraocular lesions;142333) 3) a lack of evidence of damage or avulsion to the intracranial portion of the optic nerve;1430) 4) Prolonged absolute latency or amplitude reduction in preoperative visual evoked potential (VEP) scan;1524) 5) failure to respond to steroid therapy;6141623) and 6) the presence of bony fragments compressing the optic nerve or a hematoma near the optic nerve.
Contraindications for optic nerve decompression are as follows:12) 1) complete disruption of the nerve of chiasm; 2) complete atrophy of the nerve; 3) Carotid-cavernous fistula; and 4) Inadequate medical condition to perform general anesthesia.
Preoperative Evaluation
In order to determine the condition of the visual functions, multidisciplinary teams should perform a variety of ophthalmologic evaluations, including vision tests, relative afferent pupillary defect, color vision, visual field and fundus examinations. Computed tomography (CT) scan can detect the relationship between the optic nerve and canal, and also can detect fractures of surrounding bony structures. A recent three-dimensional (3D) reconstructive CT scan provides a coronal & sagittal view, which is useful for surgeon to display an image at a desired angle. Similarly, magnetic resonance imaging can facilitate diagnosis of direct injury by tracing the optic nerve and can help assess the degree of damage to surrounding blood vessels and soft tissues. VEP can help to predict the prognosis of the final visual outcomes.27)
Surgical Technique
Classic external ethmoidectomy and medial trans-orbital approach
Traditionally, access to the medial portion of the orbit has been initiated via external ethmoidectomy.4213034) This technique provides excellent access to the ethmoid sinus and the medial wall of orbit. The incision is made along the medical canthus starting from the inferior margin of the medial aspect of the eyebrow. The periosteum is elevated and the lacrimal bone and lamina papyracea are removed to decompress the orbital cavity and approach the OC. However, external ethmoidectomy is associated with disadvantages such as unpleasant scar and facial dysplasia and as a result, has been utilized less frequently in recent years for optic nerve decompression. An endoscopic assisted medial transorbital approach has been introduced to overcome these drawbacks. Medial transconjunctival incision is performed, and subperiosteal dissection is performed posteriorly. A diamond burr is used to drill the medial wall of the apex of the orbit, the OC, and the optic foramen. Bony defects in the posterior of the medial orbital wall allow access to the medial OC ring. Tilt the orbital contents lateral sides and remove the thinning OC ring that has been made with a diamond burr.
Transcranial approach
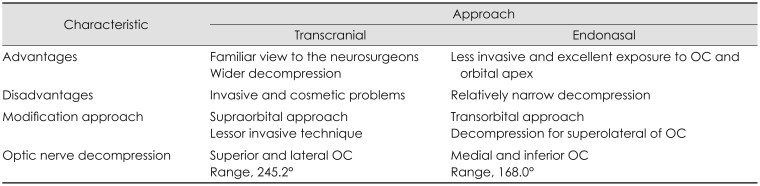
Transcranial approach provides a wide surgical corridor while showing a familiar view to the neurosurgeons.51335) In the morphometric analysis, the range of OC decompression via transcranial route was 245.2 degrees, which enabled wider decompression than endonasal route.13) However, the transcranial approach is more invasive and associated with more cosmetic problems than the endonasal approach and brain retraction may cause serious complications.
To perform the transcranial approach under general anesthesia, with the supine position taken, fixed with 3-pin head fixator, the head is rotated 5 to 30 degrees contralaterally and extended 10 to 15 degrees. If a neuro-navigation system can be installed, it will help surgeons to identify the anatomical location during surgery. After making a general curved linear incision, a craniotomy is performed allowing for a pterional approach. Extradural anterior clinoidectomy is performed after sphenoid ridge flattening. Arachnoid dissection, cisternal opening, and lumbar drainage for brain relaxation may allow drilling without a retractor. When performing anterior clinoidectomy, the OC and strut should be completely unroofed to the superolateral side and caution should be taken to avoid damage to the periorbita. Care should be taken to drill the upper surface of the OC. Saline irrigation should be maintained to prevent thermal damage to the optic nerve during drilling. If the anterior clinoid process (ACP) is small, remove it with small rongeur carefully. However, if the ACP and optic strut are thickened, remove some of them by drilling. After dura incision is made, the optic nerve is decompressed by splitting the falciform ligament, the optic nerve sheath, and annular ligament.
Recently, minimally invasive optic nerve surgery has been actively studied and the optic nerve decompression through the supraorbital approach has been introduced.25,29) Based on the previously introduced supraciliary keyhole approach, extradural unroofing of the OC is performed using an endoscope. The supraorbital approach is fast and cosmetically effective, with the disadvantage that it is somewhat smaller than the classic transcranial approach in OC exposure. However, only cadaveric studies have been published without clinical applications, further research is needed.
Endonasal approach
A number of advantages of approaching the base of the skull via endoscopic endonasal approach have been noted.1,3,8,10,14,17) This technique is less invasive and shows excellent exposure to OC and orbital apex than classic transcranial approach.
Under general anesthesia, the patients were prepared similar to the endoscopic endonasal approach described above. Following decongestion of the nasal mucosa using epinephrine-soaked cotton, a 4 mm, 0 degree, rigid endoscope is introduced inside the nostril and middle turbinectomy, and a posterior ethmoidectomy is performed. After the sphenoid ostium is confirmed, sphenoidotomy and posterior septectomy are performed. Sphenoidotomy is widely performed laterally to ensure sufficient space for optic nerve and internal carotid artery (ICA). Anatomical landmarks such as optic carotid recess, OC, ICA, posterior ethmoidal artery and resection of thin lamina papyracea should be identified. Decompression of the OC should be performed in a gentle manner using a diamond drill, and continuous irrigation should be maintained to prevent thermal injury. Unroofing of the OC should proceed to the distal to proximal area to identify the opticocarotid recess and minimize injury to the ICA and dura. Also, the bone covering the OC should be removed very carefully by making it thin like an egg shell.
After performing inferomedial portion of OC decompression, the optic nerve sheath is opened using a sickle knife. When incising the optic nerve sheath, the incision on the superomedially side of OC may prevent damage to the ophthalmic artery.19) However, there is some controversy about the optic nerve sheath opening because indirect TON has no effect on the visual outcome.32) Surgical procedures for opening the OC using a 45 degrees endoscope without posterior ethmoidectomy and middle turbinectomy have also been reported, but the surgical field may be limited if the endoscope is unfamiliar.6)
Through the above method, it has been observed that the OC can be decompressed an average of 168 degrees, but there are restrictions on the superolateral part of the OC. To overcome the limitations associated with using the endonasal approach on the superolateral side, total circumference decompression through the combined trans-orbital approach was studied.910) Start by making a 2.5 cm or greater incision along the eyelid wrinkle line as previously reported and identify the orbicularis oculi muscle.27) Once the superolateral border of the orbital rim is identified, and the superior and inferior orbital fissure is confirmed by carefully dissecting the periosteum. Near the superior orbital fissure, recurrent meningeal artery may be seen in cranioorbital foramen. If possible, peel off the periorbita without injury so that it makes easier to proceed with surgery. The orbital contents are protected using silastic sheets and displaced to infero-medially. Bony decompression of the OC is performed by drilling carefully from greater wing to lessor wing of sphenoid. Morphometric analysis suggests that 360 degrees OC decompression is possible when this approach and endonasal route are simultaneously performed. However, since only cadaveric studies have been conducted, more clinical studies are needed.
Choice of surgical approach
Each approach is summarized in Table 1. When the bony fragment is found around the OC, it should be removed during operation. So, the surgical approach should be chosen that allows easy access to the displaced fragment. And associated lesions will be the other consideration to determine the surgical approach. If the ipsilateral TON is accompanied with a large ipsilateral hematoma in the frontal lobe, the transcranial approach is the appropriate choice to remove the hematoma and decompress the OC at the same time. When the wide decompression for the OC is planned, either surgical approaches are appropriate. To avoid the potential for brain injury, endoscopic transnasal or transorbital approach may be preferred choice of surgical procedure.
Outcome of OC Decompression
Table 2 summarizes surgical results according to the method and timing of surgery. A comparison of treatment outcomes for endonasal and transcranial approaches has not been reported. The majority of studies were retrospective analyses of each method, and show favorable outcomes. In the case of transcranial optic nerve decompression for TON, 30% to 70% in patients showed improvement in their vision.153435) Endoscopic endonasal approach for TON was reported to improve visual acuity in 51% to 58% of cases, albeit with a time difference. In addition, better results were obtained in patients with good pre-operative visual acuity than in patients with complete blindness. Patients with no light perception, light perception, hand motion and finger count had a response to endoscopic endonasal surgery of 41%, 89%, 93%, and 84%, retrospectively.8) In addition, the combination of surgical and medical treatment (steroid therapy) do not produce better results than the medical treatment alone.26,34)
The global complication rate of endoscopic endonasal approach was reported as 9.1%, and 3.1% of severe complications such as iatrogenic carotid and ophthalmic artery injury, cerebrospinal fluid leakage, vision deterioration and infections were accounted.8)
Conclusion
As previously described, optic nerve decompression can be performed in a variety of ways and methods. However, it is not yet clear which approach is best. Furthermore, since different methods of decompressing the optic nerve offer different strengths and weakness, it is important to consider various approaches depending on the patient's condition and needs.
 XML Download
XML Download