

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Chiropractic treatment of the cervical area is a technique used often in recent years to treat musculoskeletal lesions, but it can occasionally lead to significant complications, such as dissection of the vertebral artery (VA), vertebralbasilar insufficiency, and cerebellar or brainstem infarction.127910) Complications are relatively rare, but they can be fatal and should not be neglected. We describe the case of a patient who suffered from infarction of the posterior inferior cerebellar artery (PICA) after a cervical chiropractic manipulation.
Case Report
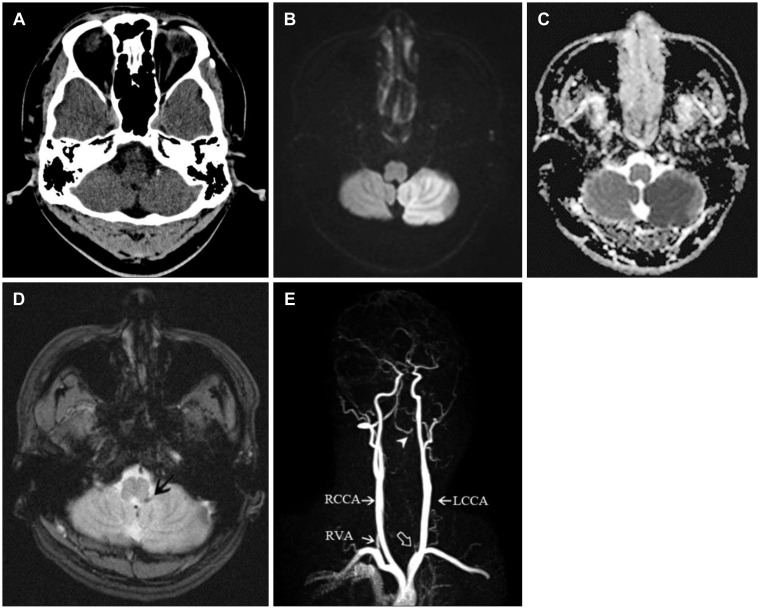
A 39-year-old man visited the emergency room with a dizziness and balance impairment that occurred 6 hours before. At the time of admission, the patient showed alert consciousness, but neurological examinations showed the signs of cerebellar dysfunction. Finger to nose, heel to shin and rapid alternating movement test showed that cerebellar function was impaired on the left side, with intact function of the right side. Blood pressure was 150/80 mmHg, and pulse rate was 88 beats/min with normal sinus rhythm of electrocardiography. He had no underlying disease and no medication use. Routine laboratory tests of blood and electrolytes, were within normal ranges. He initially denied any trauma, but remembered severe pain when he underwent a cervical chiropractic manipulation about two weeks prior. Upon imaging, skull and cervical spine radiographs were normal. Brain computed tomography (CT) showed normal cerebellar parenchyma (Figure 1A). But magnetic resonance (MR) imaging (MRI) revealed acute infarction in the left PICA territory (Figure 1B and C). Gradient echo image suggested blood clot in left PICA (Figure 1D). MR angiography revealed complete occlusion of left VA with retrograde blood flow (Figure 1E).
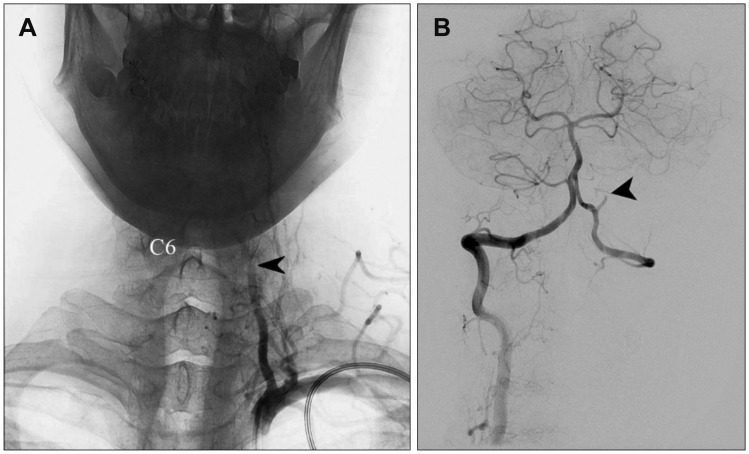
Transfemoral cerebral angiography revealed the occlusion of left VA at V1/2 junction. And it showed the retrograde blood flow to the left VA to the V2 segment (C1 level) and also showed the occlusion of left PICA (Figure 2A and B). After angiography, the patient was admitted to a neurological intensive care unit, and he received antiplatelet therapy with the use of Aspirin® 100 mg/day (Bayer AG, Leverkusen, Germany). There was no embolic source in the heart transthoracic echocardiogram and heart CT. And doppler ultrasonography did not reveal atherosclerosis of both internal, external carotid arteries. So it is unlikely that the infarction was caused by cardiac thrombosis or other vascular abnormalities.
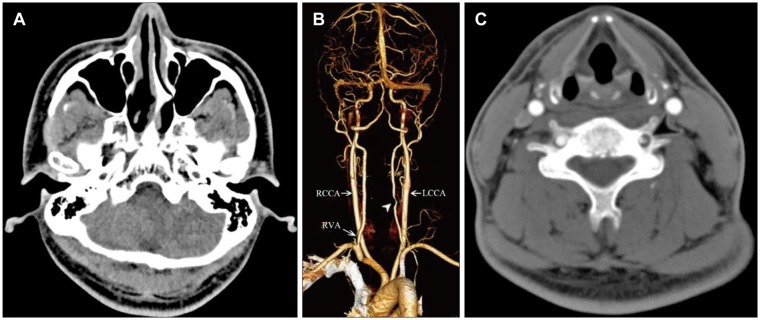
At 1 month later, axial CT imaging showed the change to the chronic phase of left PICA infarction (Figure 3A). And in neck CT subtraction angiography, previously obstructed VA flow was partially improved at V1/2 level (Figure 3B). Maximum intensity projection image from enhanced CT suggested suspicious dissected wall of left VA (Figure 3C).
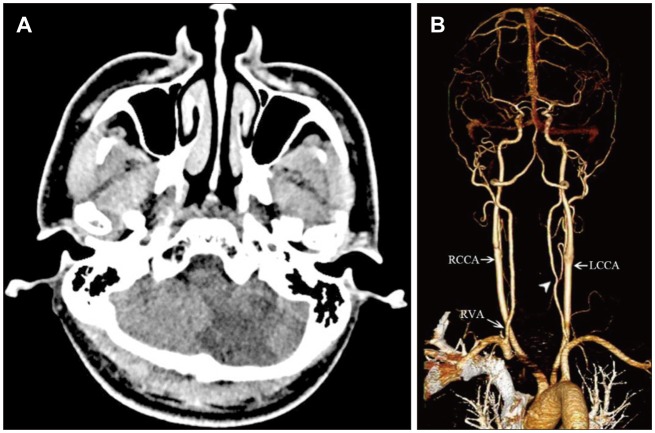
Three weeks later, he was discharged without sequelae and was regularly followed up with at an outpatient clinic using antiplatelet agents. During a follow-up at 3 months, brain and neck CT angiography showed low density in left PICA territory but showed more improved state of VA dissection at the left V1/2 junction with focal stenosis remained compared to the previous study (Figure 4A and B).
MRI vessel wall study was not performed at the first time so we did not prove the intravascular thrombosis directly. However, it could be diagnosed as a dissection because he was relatively young and healthy person and was improved so fast by only medical treatment.
Discussion
To treat cervical and lumbar pain, chiropractic manipulation is considered an alternative therapy.17) This procedure can injure the neck vessels, typically representing the cervical segment of the VA, and this could produce a cerebral stroke and disability symptoms.9) Rates of VA dissection following a cervical manipulation are rarely reported, so the exact incidence is unknown.18)
VA dissection can injure the intima or media of the vessel, causing hematoma formation in the subadventitial or subintimal layer. As a result, blood flow is stopped and thrombosis or distal embolism of the dissection site appears.310) Focal ischemia occurs several hours or weeks after such a dissection, which occurs either because blood flow is reduced from the arterial blood supply or because the risk of thrombosis and embolism is increased due to the turbulence and irregularities in the vessel wall at the dissected location.24)
Any part of the carotid artery and VA can be injured, depending on the direction, degree, and force of cervical manipulation.56) But, damage to the V3 portion is the most common injury that may occur after chiropractic manipulation related to anatomical structures. The VA is located horizontally in a groove in the upper side of the atlas' posterior arch. During abruptly forced neck rotation and stretching, the gap between the atlas and the atlanto-occipital membrane, which the VA penetrates, can be stretched, resulting in dissection.1) In our case, it appeared that the V1/2 junction had been dissected due to excessive lateral bending of the neck, thought to be caused by an impact to the left transverse foramen of the sixth cervical spine, through which the left VA passes. It is presumed that there was a mechanical injury to the vessel wall at the time of the procedure, which caused dissection and then the thrombus generated, and two weeks after small emboli caused the occlusion of PICA.
Low-speed, high-amplitude manipulations that consist of a series of smooth, repetitive movements are configured in certain areas of the neck, and this does not often cause damage. However, a sudden thrust or high-speed, low-amplitude manipulation is often considered the cause of VA dissection.1) In particular, this type of manipulation can be theorized to result in a sudden, symmetrical rotation of the extended cervical vertebrae, leading to damage to the high cervical and proximal parts of the carotid artery and VA.
Rothwell et al.8) have not found an association between chiropractic treatment and stroke in elderly patients, but this may reflect a number of factors. Chiropractors assume that younger patient can actively manipulate the neck to increase the likelihood of arterial injury, and they tend to look for younger and more active chiropractic adjustments more often.
Dissection is unthinkable, and the results can be severe, so early diagnosis and treatment are essential. Patients with a recent history of seizure(s), dizziness, balance decline, and cervical chiropractic treatment should consider the possibility of VA dissection. The treatment for this is anticoagulant or antiplatelet therapy.310) Surgical intervention only applies to patients with persistent and fatal symptoms that are untreatable. Intravascular therapy, including balloon angioplasty and stenting, may be used as an initial treatment only if pharmacological treatment fails.310)
 XML Download
XML Download