

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Acute subdural hematoma (SDH) can be treated conservatively if the neurologic symptoms are mild or the size of the hematoma is small; however, immediate surgical treatment should be considered if patient shows loss of consciousness, worsening of neurological symptoms, or a large size of hematoma.715) The primary surgical treatment for acute SDH is to perform craniotomy which can remove hematoma completely, but there may be complications from general anesthesia and procedure itself. One may consider burr hole surgery for removal of hematoma, but it is difficult to secure the clear view of surgical sight, completely remove hematoma, and decrease intracranial pressure in short period of time. We report the result of burr hole drainage with additional urokinase for removal of hematoma in a limited situation where craniotomy is not possible.
Case Report
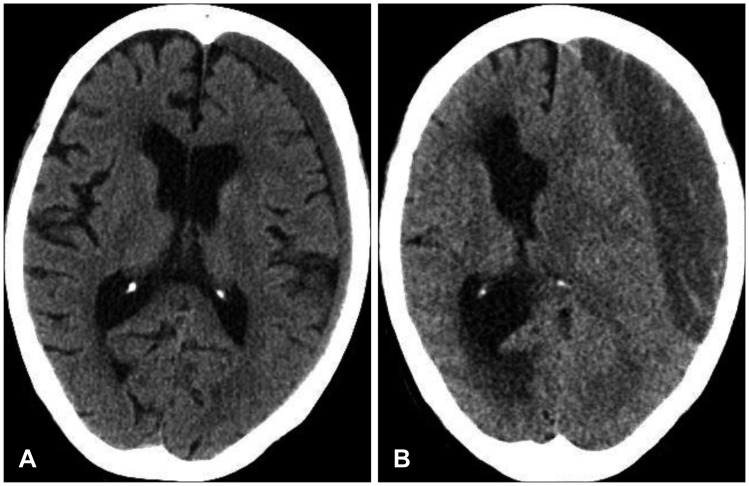
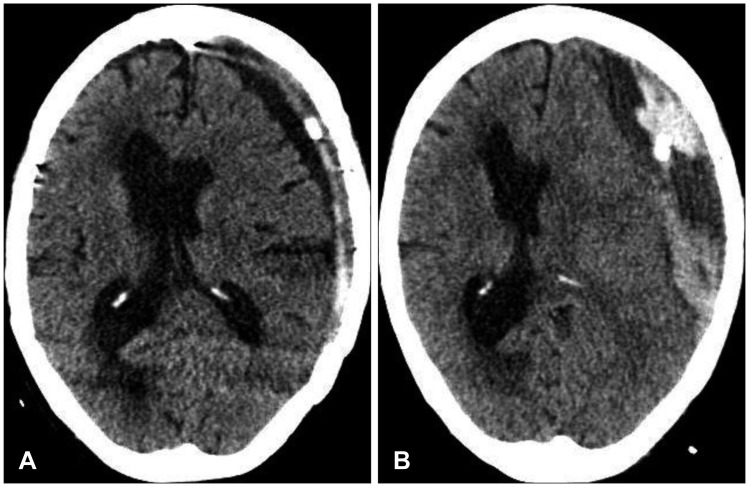
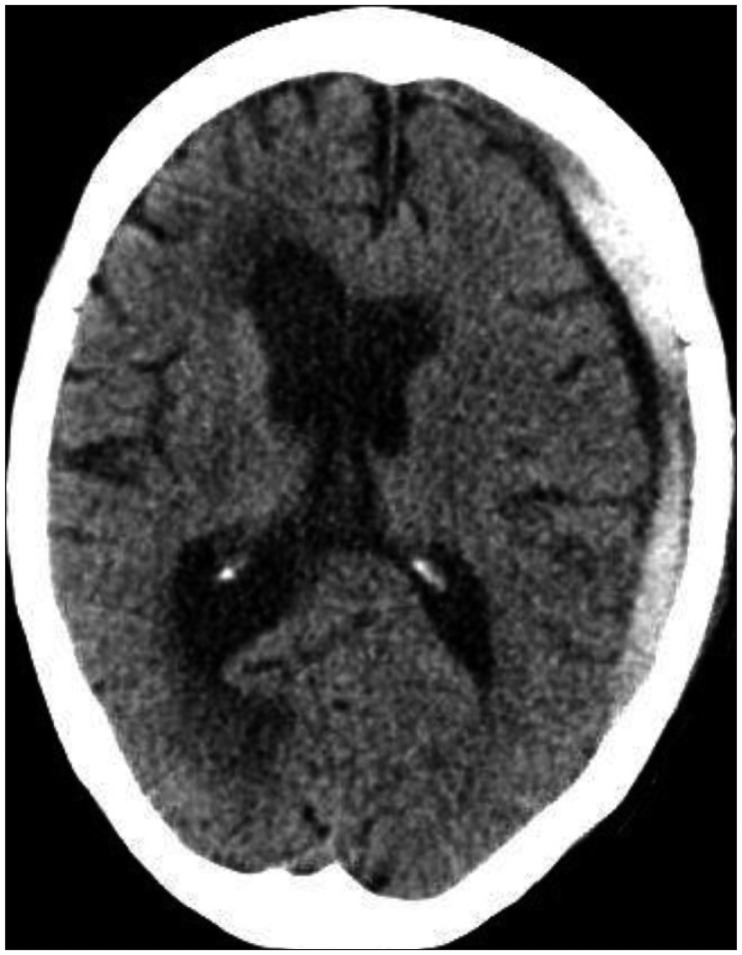
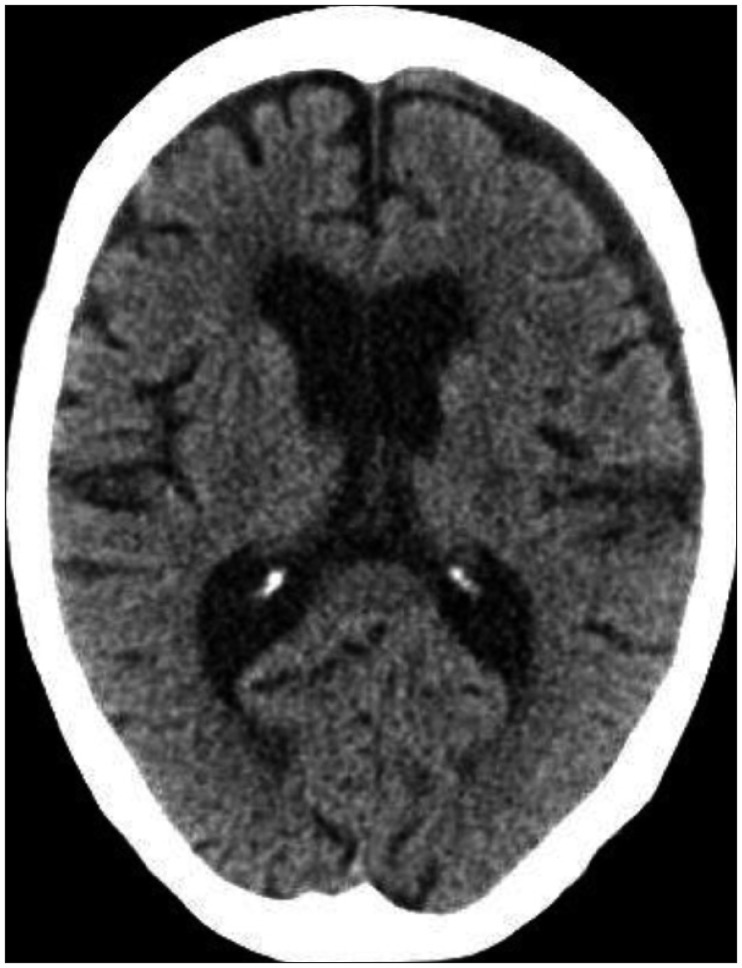
A 90-year-old female patient was admitted to our medical center due to a mental change. The patient was in a stuporous state, and Glasgow coma scale (GCS) was checked by E2M5V1. She had experienced a head injury two months before the admission, and a post-traumatic computed tomography (CT) scan performed immediately after trauma indicated chronic SDH in the left hemisphere (Figure 1A). Although she had no neurologic symptoms at first, symptoms such as dysphagia and right-sided weakness gradually appeared. The follow-up brain CT scan showed increase in volume of the hematoma at the left hemisphere (Figure 1B). She got the burr hole trephination with closed drainage in the left parietal area under the general anesthesia. Follow-up CT scan performed the day after the surgery revealed well-drained chronic SDH (Figure 2A). Her right side motor weakness improved after surgery and GCS was checked by E3M6V3. On day 3 after surgery, the patient abruptly showed stuporous mentality and CT scan revealed acute hematoma inside a cavity of chronic SDH with the midline shift toward the right (Figure 2B). The CT image indicated newly development acute SDH over the pre-existing chronic SDH cavity. Her family did not want more surgical treatment because of her age, and they wanted conservative therapy. We decided to liquefy and drain the solid hematoma by urokinase irrigation using the existing closed drainage system. 17,000 IU of urokinase was injected into the hematoma cavity once daily for 2 days and clamped for 30 minutes. The total drainage volume was 183 mL for two days, and only a small amount of residual hematoma was observed in the CT scan performed two days after irrigation (Figure 3). The patient made a remarkable recovery and had little neurological deficit. GCS was checked by E4M6V4 when discharged. A two-month follow-up CT scan indicated excellent brain re-expansion (Figure 4).
Discussion
The number of elderly patients who are diagnosed with acute SDH or chronic SDH due to head trauma is increasing with the growth of elderly population. Despite advances in surgical and anesthetic techniques, the outcome of surgery for head trauma in the elderly is very poor because body's ability to maintain homeostasis decreases with aging, and various underlying diseases easily lead to complex systemic complication.817) Thus, careful selection and precise judgment are important in determining surgical treatment.
A weak physical condition or low physiological reserve due to aging cannot be a contraindication to surgery.3) These factors rather delay operation, and such postponement rather increases the postoperative mortality rate in elderly patients. Often, guardians refuse craniotomy of elderly patients diagnosed with acute SDH and prefer conservative treatment even in the situation where the surgery is desperately needed because of the prejudice that old man may not tolerate brain surgery. In such cases delayed surgery, performed as last resort, depletes patient's recuperative, so it is not helpful at all for patient. When it is hard to persuade guardians, we believe that burr hole drainage of hematoma using urokinase is an option of treatment for patients with acute SDH.
In acute SDH, the hematoma should be removed immediately by craniotomy if the neurological condition gets worse with increase in intracranial pressure due to large size of hematoma, or if the thickness of the hematoma is more than 10 mm with midline shift more than 5 mm.2) It is difficult to drain the hematoma through burr hole because hematoma becomes solid in acute SDH unlike chronic SDH which contains liquid contents.916) Craniotomy should be considered for patient with thick, wide acute hematoma, but it may develop complications due to long surgical hours, general anesthesia, profuse bleeding, etc. Especially, it may be hard for elderly patient to undergo craniotomy who has high risk associated with general anesthesia due to underlying diseases or clotting problem due to antiplatelets or anticoagulants use.14) Rather, burr hole hematoma drainage with urokinase may be considered for those limited situations if the patient shows mild neurologic disorder and does not have high intracranial pressure.
Burr hole hematoma drainage with urokinase is commonly used as safe method to lower intracranial pressure or remove hematoma due to acute intracerebral hematoma or acute intraventricular hemorrhage.46) Treatment of chronic SDH or traumatic epidural/subdural hematoma which does not require emergency craniotomy with urokinase through burr hole shows good result as well.151011) Since this method slowly dissolves hematoma, the expansion of the contralateral lesion caused by craniotomy can be prevented as well as rebleeding and pneumocephalus. The disadvantage, however, is that it takes effort to dissolve hematoma using urokinase and patient's recovery pace is slow.
The rate of recovery after burr hole surgery of chronic SDH is high, but postoperative complications often occur. The common complications after chronic SDH surgery are acute SDH and tension pneumocephalus. Additionally, subarachnoid hemorrhage, supratentorial hemorrhage, intracerebral hemorrhage, intraventricular hemorrhage, and remote cerebellar hemorrhages may occur rarely.12) The most common complication in recent studies is acute SDH. It seems to be the result of direct flow of fresh blood from the scalp injury into the subdural space.13)
In this case report, the patient was admitted for chronic SDH and treated with burr hole surgery after which acute SDH occurred as postoperative complication. Although her family wanted conservative therapy, we removed the hematoma with urokinase and achieved good outcome. In limited cases where acute SDH develops as complication after drainage of chronic SDH, urokinase irrigation may be used if the patient has a few neurological change or is not in good physical condition for craniotomy.
Conclusion
Although this is a case report of only one patient, we believe that burr hole drainage of hematoma with urokinase is effective minimally invasive treatment which can be safely performed in patients with acute or subacute subdural hematoma as reported in other studies. We believe that this surgical approach is a good choice for patients who have risk of complication from general anesthesia or have family pessimistic about surgery. Safety and result of procedure should be further analyzed in near future with more cases through clinical experiences.
 XML Download
XML Download