

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Subaxial cervical spine injuries involving the articular pillars, facets, and posterior ligaments are common and operative management is controversial, with reports describing varying outcomes of anterior,1724) posterior,8) or combined approaches.211) Posterior cervical approach enables direct visualization of facet dislocations, and facilitates decompression of the central canal and neural foramina.23) Disadvantages of the approach include a relatively longer operative duration, increased muscle dissection, post-operative neck pain, increased blood loss, and a relatively higher risk of surgical site infection. In addition, the approach is unable to address ventral compressive disc herniation.416) Recently, anterior cervical discectomy and fusion (ACDF) and plate stabilization has been widely employed with a high success rate and good clinical results for subaxial cervical spine injuries.2224) Anterior cervical approach enables decompression of the spinal canal by removing the disc and thus avoiding further neurologic deterioration due to disc displacement.1327) Although autologous bone grafting has been considered the gold standard for ACDF, this method may lead to harvest-site morbidity such as chronic pain, hematoma, infection, injury of adjacent nerves, visceral herniation, and iliac crest fracture.9) This study evaluates the usefulness of the polyetheretherketone (PEEK) cage filled with demineralized bone matrix (DBM) and plate fixation in anterior interbody fusions for subaxial cervical spine injuries, by analyzing radiographic and clinical outcomes.
Go to : 
Materials and Methods
Patient population
A retrospective review of 174 patients who underwent single-level ACDF with plate fixation for post-traumatic subaxial cervical spinal injury at a single institution from March 2005 to June 2018 was conducted. This retrospective study was based on a review of the hospital charts, operative notes, and out-patient clinical, and radiographic follow-up data. We reviewed the patient charts for clinical variables such as age, sex, cause of injury, level of injury, and level of neurological compromise as determined by their Frankel scale12) on admission and on last obtainable follow-up examination. Follow-up <6 months were excluded. Patients with associated anterior cervical bone injuries, including unstable vertebral body fractures, were excluded from the study because these patients required a combined approach (anterior-, posterior-) or additional operation methods such as corpectomy. As a result, 98 patients were enrolled for this study. Diagnosis of lateral mass, or facet fracture was made with plain radiographs and computed tomography (CT) scan. Magnetic resonance imaging was performed to evaluate for disc or ligament disruption, epidural hematoma, cord compression, or contusion in all patients. High dose intravenous methylprednisolone was administered to patients with acute spinal cord injury presenting within 8 hours from injury, as per the National Acute Spinal Cord Injury Study II.5) A trial of reduction under general anesthesia was attempted with Gardner-Wells tongs application. Following reduction, anterior cervical stabilization was performed surgically with interbody fusion. All attempts were made to provide treatment within 24 hours of the traumatic event, when not limited by other concomitant injuries.
Surgical procedure
General anesthesia was used in all patients. A Standard Smith-Robinson method was performed to expose the involved segment. After the roots or the spinal cord were totally decompressed by removing the disc and osteophytes microscopically, and end-plate cartilage was removed by a high-speed burr and curette. PEEK cage was then packed with DBM (Grafton; Osteotech, Inc., Shrewsbury, NJ, USA) and the local osteophyte-derived bone chip, and was inserted into the intervertebral space. Finally, anterior plating was performed. The cage we used was the Solis cage (Stryker Spine, Allendale, NJ, USA). A Zephir (Medtronic Sofamor Danek Inc., Memphis, TN, USA) plate with unicortical titanium screws was used. Intraoperative fluoroscopy confirmed appropriate position of the cage and the alignment of the cervical spine. Postoperatively, all patients were braced in a Philadelphia cervical collar for 8 weeks and early ambulation was encouraged.
Radiologic assessment
Radiographic data were evaluated at 6 weeks, 3, 6, 9, and 12 months after operation, and then annually with upright antero-posterior and neutral lateral X-ray films. Flexion and extension radiographs were also obtained, at the 6-month postoperative follow-up and on subsequent visits. Segmental lordosis of the cervical spine was measured by Cobb's angle using neutral lateral radiographs. Interbody height (IBH) of fused segments (the length between the center of the superior end plate of the cranial vertebral body and the inferior end plate of the caudal vertebral body) was measured. Fusion was defined by the following criteria; 1) less than 2 mm change in the posterior interspinous process distance at treated level on lateral flexion-extension radiographs; 2) bridging bone between the end plates; 3) no sign of implant failure of the anterior plate system; and 4) less than 50% of radiolucency covering the outer surface of the implant.19) Additional evaluation was done by CT, in case of any suspicion regarding union. Complications that were related to plate, screw, and cage were checked. The development of adjacent segment degeneration (ASD) was evaluated using simple lateral radiographs at the final follow up. ASD was defined as narrowing of the disc height with anterior or posterior osteophyte formation, in a comparison of post-operative radiographs with the last follow-up radiographs.18) These measurements were performed by a single independent radiologist who was not involved in the surgery or care of these patients (Figure 1).
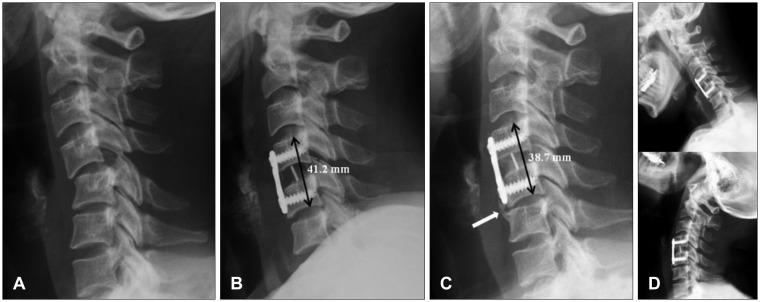 | FIGURE 1Imaging studies of C4 and C5 anterior cervical discectomy and fusion (ACDF). (A) Simple cervical lateral radiograph shows C4 and C5 subluxation. (B) Immediate postoperative radiograph shows satisfactory stabilization of injured segment after C4 and C5 ACDF. (C) Last follow-up radiograph at 27 months after surgery shows satisfactory fusion at the C4 and C5 level. However, some degrees of subsidence and development of adjacent segmental degeneration (white arrow) were observed. (D) Last follow-up flexion-extension radiographs show also stabilization with less than 2 mm change in the posterior interspinous process distance at the C4 and C5 level.
|
Clinical outcome assessment
Patient status was reviewed clinically at 1, 3, 6, 12 months postoperatively, and then annually. Clinical outcome was assessed using visual analog scale (VAS) scores for neck pain (0=no symptom; 10=maximum pain). Neurologic assessment was done using the grading scale of Frankel: Grade A had no motor or sensory function; Grade B had sensory but not motor function; Grade C had useless motor function with sensations; Grade D had useful motor function and sensation with some deficit; Grade E had normal motor function and sensation.12)
Statistical analysis
Data were analyzed using the SPSS program for Windows version 12.0 (SPSS Inc., Chicago, IL, USA). The independent t-test was used for analyses. Data have been presented as mean±standard deviation. For all analyses, a p-value of <0.05 was considered statistically significant.
Go to :
Results
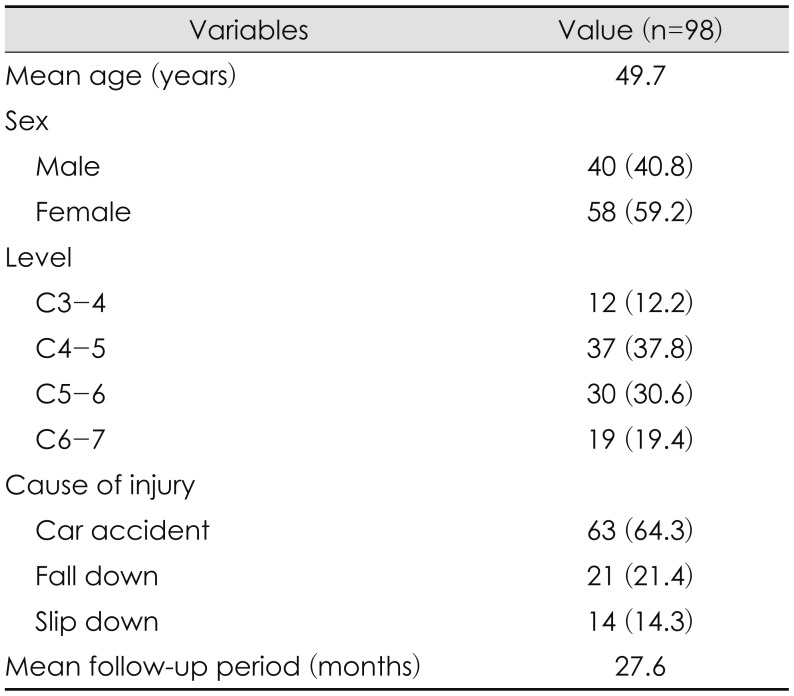
Clinical characteristics of the enrolled patients are summarized in Table 1. The study comprised of 40 males and 58 females with a mean age of 49.7 years (range, 17–78 years). Cervical injury was caused by a car accident in 63 cases, fall from height in 21 cases, and fall due to slipping in 14 cases. Plain lateral radiographs and cervical CT with sagittal and coronary reconstruction were obtained in all patients and demonstrated subluxation or dislocation at C3 to C4 in 12 patients, C4 to C5 in 37 patients, C5 to C6 in 30 patients, and at C6 to C7 in 19 patients. The most common level of dislocation was C4 and C5 level. The mean follow-up period was 27.6 months (range, 6–142 months).
Clinical results
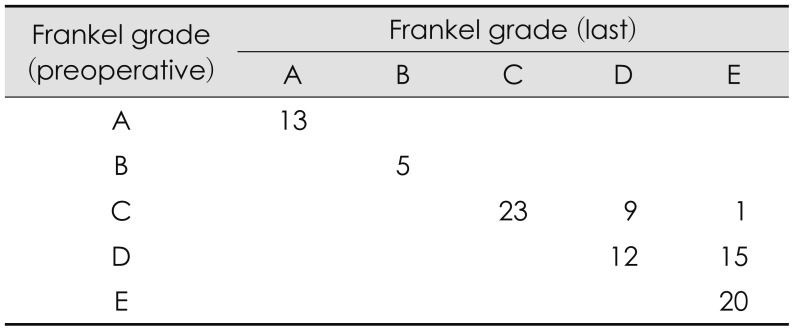
A summary of clinical outcomes is provided in Table 2. No change was observed in 13 patients with Frankel Grade A and 5 patients with Frankel Grade B. Thirty-three patients of Grade C, 27 patients of grade D, and 20 patients of Grade E showed an improvement to 23, 21, and 36 patients, respectively. As the final outcome, an improvement by at least on Frankel grade was observed in 21 patients (21.4%). No patient experienced neurological deterioration. Mean preoperative VAS score for neck pain was 8.3±0.9. The mean VAS score for neck pain at the final follow-up was 2.6±1.5. The postoperative difference was statistically significant compared with the preoperative score (p<0.05, χ2 analysis).
Radiographic results
All patients demonstrated solid fusion on their final follow-up studies. Each of them demonstrated radiographic evidence of complete formation of a bony bridge between the graft and the vertebral body. Fusion could be achieved on a mean of 15.1 weeks after surgery (range, 8–47 weeks). None of the 98 patients revealed segmental motion >2 mm at the operative level. The mean preoperative Cobb's angle was −3.7±7.9°. The mean Cobb's angle immediately after surgery was 3.9±6.3° and at final follow-up was 1.9±5.1°. The surgery resulted in a significant reduction in the regional kyphotic angle (p<0.05). The mean preoperative IBH was 36.9±1.7 mm. The mean IBH immediately after surgery was 40.8±2.0 mm and at the final follow-up it was 38.2±1.8 mm. The mean increase in height at final follow-up was 1.3 mm. The difference between preoperative IBH and final IBH measurements was significant (p<0.05). There were five patients (5%) who showed adjacent segment changes. However, no patient required additional surgery, due to absence of neurological deterioration. A summary of radiological outcomes is provided in Table 3.

Postoperative complications
No patient in our study developed a hematoma or wound infection after surgery. There was no patient with vertebral artery injury, recurrent laryngeal nerve palsy, or esophageal injuries. No case of hardware failure such as breakage or migration occurred during the follow-up period.
Go to :
Discussion
Reduction and stabilization of the injured segment is the basic principle in the treatment of subaxial cervical spine. Until now, Surgical strategies have reported successful outcomes in the treatment of subaxial cervical spine injuries using an anterior,1724) posterior,8) or combined approaches;211) however, the optimal approach has not yet been established.
Posterior stabilization techniques have been employed with good results using wires, hooks, screws, and rod systems.1028) The advantages of posterior cervical approach include direct visualization of facet dislocations and decompression of the central canal and neural foramina.23) However, disadvantages include a relatively longer operative duration, increased muscle dissection, post-operative neck pain, increased blood loss, and a relatively higher risk of surgical site infection. Moreover, although the incidence of disc disruption may be as high as 40% in unilateral facet dislocation and 80% in cases of bilateral cervical facet dislocation,26) the approach is unable to address ventral compressive disc disruption.416) Without appropriate management, disc disruption could cause neurological deterioration and anterior collapse of the disc space, which could lead to a kyphotic deformity.14)
On the other hand, anterior cervical approach enables decompression of the spinal canal by removing the disc, thus avoiding neurological deterioration by further disc displacement.1327) Majority of patients in this study had fractures involving the posterior lateral masses or facets. Fractures of the cervical lateral masses of facet joints often result in rotational instability of the cervical spine. These fracture patterns often occur in compression-extension injuries, leading to annular disruption of the disc.3) In our experience, we have almost always encountered grossly disrupted discs during surgery, and these findings have led to our preference of the anterior approach. Additionally, anterior plate fixation after ACDF could provide effective stabilization with the advantage of single motion specific segment fusion in cervical facet dislocation. Whereas, posterior screw fixation disadvantage was seen with posterior elements fractures, often necessitate longer fusion levels. Biomechanical studies however, have reported the suitability of posterior screw fixation over anterior plate fixation for subaxial cervical spine injuries.731) Despite these studies, the use of ACDF and plate fixation as the primary method of stabilization for subaxial cervical spine injuries is gaining popularity among spinal trauma surgeons, with a high success rate and good clinical results.17222430) In this study, all patients were successfully stabilized through the anterior approach, and there was no instability at the last follow-up. The stabilization rate in this study is favorably comparable to previous literature reports, which range from 86.2% to 100%.17203233) Therefore, ACDF and plate fixation could be an excellent treatment option for traumatic subaxial cervical spine injuries. If there is some disadvantage of ACDF, autologous bone graft has been considered as the gold standard, causing harvestsite morbidity such as chronic pain, hematoma, infection, injury of adjacent nerves, visceral herniation, and iliac crest fracture.9) These risks of autologous bone graft morbidity have been widely reported, suggesting the need for an alternative fusion method that obviates iliac crest harvest.29) Various materials have therefore been developed and used for interbody grafts with the ACDF, in order to avoid morbidity associated with autologous bone grafts. Representatively, PEEK material cages have been developed to achieve immediate stability and successful bone fusion.625) Titanium spikes provide immediate solid fixation between the cage and the vertebral body, reducing the risk of cage migration. Many of the complications associated with iliac crest harvest have been significantly reduced with the use of the cages. Additionally, DBM, which contains bone morphogenic proteins, was introduced as a bone inductive substance. Some types of DBM have both osteoinductive and osteoconductive capability.15) In this respect, the use of DBM can be a good option for fusion. In our previous report, Kim et al.20), demonstrated that ACDF using a PEEK cage filled with DBM followed by anterior plate fixation in subaxial cervical injury showed no statistically significant difference in fusion rates and satisfactory clinical outcomes without donor site pain, as compared with autologous bone grafts. Kandziora et al.19) compared the use of titanium cage filled with osteosynthetic material and anterior plate fixation to the use of autologous tricortical iliac crest bone graft. They also reported no statistically significant difference in fusion rates and clinical outcomes. Furthermore, Hattou et al.17) reported 29 cervical spine injury cases treated by ACDF using a PEEK cage filled with synthetic bone graft and anterior plate fixation. They reported that the fusion rate was 86.2% and synthetic bone graft has the advantage of shorter operating time and avoiding postoperative morbidity related to iliac harvesting. In our study, 100% fusion rate was achieved by use of PEEK cage filled with DBM and anterior plate fixation, and no morbidity was observed. Although the correction of the kyphotic angle and IBH was slowly lost in many cases by the last radiographic follow-up, severe collapse or significant instability did not develop. Clinical outcomes such as pain, function, and patient satisfaction were excellent. From these results, with advantages of no donor site morbidity and no graft-related complications, the PEEK cage filled with DBM and anterior plate fixation seems to be safe and effective for the treatment of single-level subaxial cervical spine injuries.
While this study is currently the largest till date compared with those identified in the literature, with 98 patients undergoing PEEK cage filled with DBM and anterior plate fixation in subaxial cervical spine injuries, limitations do exist related to the retrospective nature of this database leading to a selection bias owing to lack of record keeping. Additionally, long-term radiographic and clinical follow-up are limited by a relatively poor follow-up, due to this particular patient population. In the present study, the mean follow-up period was 27.6 months (range, 6–142 months) and our loss to follow-up was 76 patients (43%). However, this numerical value is comparable to previous literature reports, wherein the loss to follow-up ranges from 29.2% to 49%.12132) Most importantly, we did not analyze according to the injury mechanism or subaxial injury classification, but according to previous reports,1730) anterior-only fixation would be enough for cervical spine injuries regardless of the injury mechanism or subaxial injury classification. Prospective studies with long-term clinical follow-up are required.
Go to :
 XML Download
XML Download