

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Benign prostatic hyperplasia (BPH) is one of the main factors for lower urinary tract symptoms in elderly men. Surgical management of BPH is the mainstay of treatment in men with symptomatic BPH who are non-responsive to medical treatment, with transurethral resection of prostate (TURP) being the gold-standard surgical treatment [1]. With an increase in the population of elderly men, better diagnostic methods, growth in economic sector, and hope of better quality of life, there has been a progressive increase in the prevalence of BPH [2]. Approximately 30% of patients with BPH require treatment [3]. Even though TURP has a high success rate, the perioperative morbidity and operative safety specially in relation to bleeding pose serious concerns [4]. In addition to bleeding, retrograde ejaculation and transurethral resection (TUR) syndrome due to irrigant absorption are also relevant to intra and postoperative complications [5]. Despite technical advancements in TURP, blood transfusion rates are still 2.0% to 7.1%, TUR syndrome occurs in 2.0%, stress incontinence in 2.2%, retrograde ejaculation in 65.0% to 70.0%, urethral strictures in 3.8%, bladder neck contractures in 4.0% and early revision rates are 3.0% to 5.0% [4]. These, along with prolonged catheterization time, advocate for alternatives to this treatment modality that offer similar clinical results but fewer complications [6]. Laser vaporization of prostate (LVP) is one of these methods. Lasers generate different effects in tissues, like coagulation and vaporization [7]. Different types of laser like potassium-titanyl phosphate (KTP), holmium, diode and thulium are available. Of these, those gaining more popularity are the photo-selective vaporization of the prostate (PVP) using the KTP laser, and holmium laser enucleation of the prostate (HOLEP) [8]. In previous decades, multiple laser devices working at different wavelengths have been introduced. The neodymium-doped yttrium aluminum garnet (Nd: YAG) laser (wavelength: 1,064 nm) and the holmium: YAG (Ho: YAG) laser (wavelength: 2,140 nm) were early laser techniques [9]. PVP is done using KTP laser (wavelength: 532 nm) and causes efficient vaporization. It provides excellent hemostasis due to its property of being greatly absorbed by hemoglobin (Hb), but due to its minimal absorption in water, it has slow ablative properties, causing prolongation of operation time [10]. The semiconductor diode laser is thought to be the best in relation to its hemostatic properties, but due to postoperative dysuria, pain, and storage urinary symptoms, it was less acceptable [11]. A newly introduced diode laser, operating on the wavelength of 980 nm, is different in terms of its new fiber design, greater ablative properties of tissues, and efficient hemostasis due to its significant simultaneous absorption in water and Hb [12]. It has the advantage of a very low rate of perioperative complication and decreased stay at the hospital, with a short learning curve [9]. Therefore, the purpose of this study is to evaluate the initial experience and outcome of PVP for BPH with the use of a newly designed twister fiber and 980 nm diode laser system. To my knowledge this is the first-hand experience from Pakistan.
Go to : 
MATERIALS AND METHODS
A prospective study was performed from November 2016 to December 2017. Patients who were diagnosed with bladder outlet obstruction secondary to BPH and underwent PVP with diode laser were enrolled in this study. Prior to study, written informed consent was taken from all patients. Surgery was indicated in patients who were refractory to medical treatment, had recurrent urinary retention, value maximum urinary flow rate (Qmax) of ≤15 mL/s even on medical treatment, and International Prostate Symptom Score (IPSS) of more than 19. Patients with prostate-specific antigen >4.0 ng/dL, history of prostate or bladder cancer, neurogenic bladder, urethral structures, or previous bladder, urethral, or prostate surgery were excluded. Those patients in which the procedures were converted to TURP and those patients who were lost to follow were also excluded from the study. Prostate size was measured with trans-rectal ultrasound. Anti-platelet drugs (clopidogrel & acetylsalicylic acid) were only stopped on the day of surgery. All demographic data, baseline, and perioperative parameters of the patients were recorded. PVP was performed by a single surgeon. Prostate vaporization was carried out with a diode laser at 980 nm (Biolitec Diode 180W laser; Biolitec, Biomedical technology GmbH, Jena, Germany) in a continuous wave mode with a 600 nm (twister) fiber. Spinal anesthesia was given to all patients. Normal saline was used as irrigant fluid through 23 Fr cystoscope sheath with 30-degree optical lens. Vaporization procedure was started from bladder neck at 6o'clock position and continued sideways onto both lateral lobes up to 12o'clock position. Like TURP, vaporization was continued to remove all prostate tissue that was causing obstruction until an adequate surgical cavity was formed. Good urinary stream was assured after the completion of procedure. 22 Fr 3-way Foley's catheter was passed and slow irrigation was started. For the removal of catheter, factors, such as prostate size, patient's comfort, bowel status, and degree of hematuria were considered. Patients were discharged soon after successful trial without catheter. Patients were evaluated by IPSS, post void residual (PVR) and uroflowmetry at 3 months and 6 months after surgery. Parameters like postoperative complications, operative time, total energy applied, and duration of catheterization were recorded. For statistical analysis, we used IBM SPSS Statistics ver. 19.0 software (IBM Co., Armonk, NY, USA). Postoperative Qmax, PVR, and IPSS scores were compared with preoperative values by using the Student t-test (paired); p-values of less than 0.05 were defined as statistically significant.
Ethical approval
This study was reviewed and approved by the Institutional Ethical Review Committee of The Kidney Centre Post Graduate Training Institute (approval number: 54-URO-082017). All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Go to :
RESULTS
Initially 110 patients were enrolled in the study, one patient was lost to follow and 9 patients were converted to TURP. Therefore, a total of 100 patients were included in the final analysis. The mean age was 65.82±10.42 years, mean prostate size was 67.35±16.42 g, operative time was 55.85±18.01 minutes and total energy was 198.68±49.12 kJ. Mean catheterization time was 43.14±7.26 hours (Table 1).
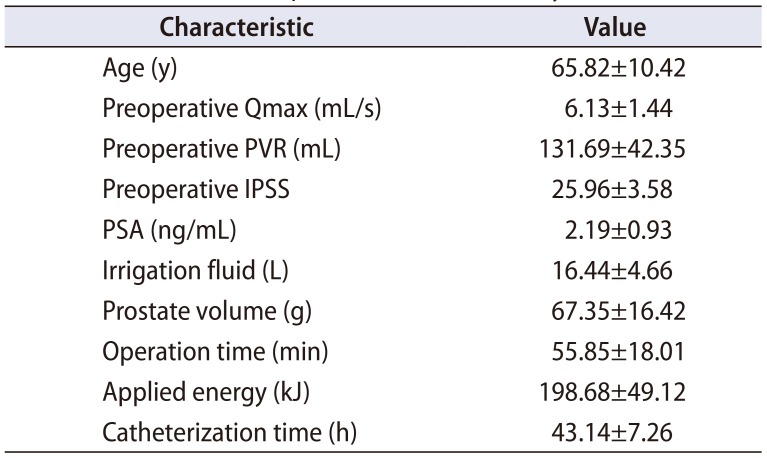
Table 1
Characteristics of patients enrolled in study
![]()
Baseline mean Qmax was 6.13±1.44 mL/s, PVR was 131.69±42.35 mL and IPSS was 25.96±3.58. At 3 months follow-up, significant improvements were noted (p<0.001) in IPSS 7.13±1.76 (−18.83), Qmax 18.22±4.78 mL/s (+12.09) and PVR 22.12±8.71 mL (−109.57). At 6 months, sustained improvements were again seen (p<0.001) in IPSS 7.04±1.69 (−18.92), Qmax 19.22±4.75 mL/s (+13.09) and PVR 18.89±5.39 mL (−112.80) (Table 2). Among laboratory parameters, mean Hb was 12.88±1.34 gm/dL and creatinine (Cr) was 1.08±0.29 mg/dL. No significant changes were observed in postoperative Hb, serum Cr, sodium and K (Table 3). No significant difference in postoperative Hb was seen in patients (n=24) who were on anti-platelet drugs compared to patients (n=76) who were not on any antiplatelet drugs (Table 3). The most frequent problems were burning micturition (35%) and terminal dysuria (29%). The 10% patients had minor hematuria (not requiring transfusion) and 4% patients had stress incontinence for few days after successful trial of catheter which were managed conservatively. Nine patients were converted to TURP due to very large prostate size (>90 g) which had significant prolonged operative time and bleeding. Interestingly, all of these patients were with catheters preoperatively for various periods. Out of these, seven of them required blood transfusion (Table 4).

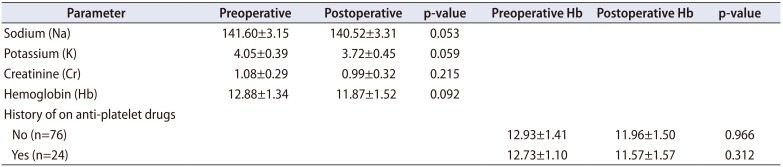
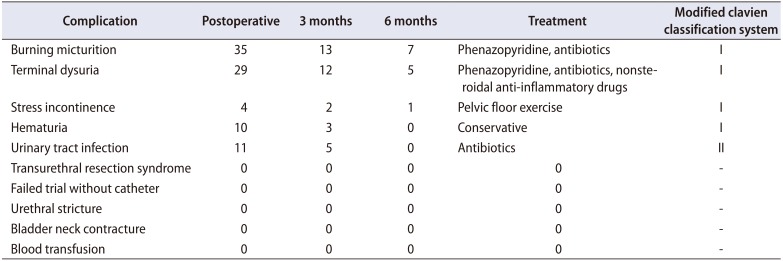
Table 2
Preoperative comparison with three and six months' outcome parameters
Values are presented as mean±standard deviation.
Qmax, maximum urinary flow rate; PVR, post void residual; IPSS, International Prostate Symptom Score.
a:Significant comparison of preoperative vs. 3 months and p-value is calculated by Paired t-test.
b:Significant comparison of preoperative vs. 6 months and p-value is calculated by Paired t-test.
![]()
Table 3
Laboratory parameters in preoperative and postoperative
![]()
Table 4
Complications of diode laser vaporization
![]()
Go to :
DISCUSSION
TURP is the most commonly performed and gold standard procedure in the surgical management of BPH [13]. Factors associated with increased complication rates of TURP include learning period, older patients, patients with cardiopulmonary comorbidities, and hemostatic disorders. Bleeding requiring blood transfusion, urethral stenosis, TUR syndrome, and prolonged catheterization times are still the most significant complications [414]. Despite its clinical outcome, this increased complication rate has led to the need for development of alternative techniques of prostate ablation with similar clinical results but with lesser complications. Amongst these, laser ablation and vaporization procedures, such as KTP, diode, and HOLEP are promising surgical techniques [91516]. It can be a challenge to select the appropriate laser to be used in the treatment of BPH. The parameters that must be considered include its effectiveness, mechanism, durability, rate of complications, catheterization time, hospital stay, and cost effectiveness. Therefore, it is necessary to know how laser works and its properties. Laser (light amplification by stimulated emission of radiation) can be produced by different medium with specific wavelength and direction [11]. The medium and the excitation source establish the wavelength and the mode of emission (continuous or pulse) of each laser type [17]. The prostatic tissue absorbs energy by its chromophores which are water and Hb. Absorption coefficients of these chromophores change with different wavelengths, resulting in differences in absorption of energy amongst laser types. Intracellular temperature is raised when energy is absorbed by prostatic tissue, leading to coagulation and subsequently vaporization of tissue [1718]. In the treatment of BPH, the medium used in the treatment of BPH is either a crystal or semiconductor. Crystals used are Ho: YAG, thulium: YAG (Tm: YAG), KTP and lithium triborate, and semiconductors used are diode lasers. Multiple laser types, with different wavelengths and hence differing properties have been developed and substantial testing of their clinical safety, efficacy, and durability has been done [9]. Among these, HOLEP has functional outcomes similar to those of TURP and open prostatectomy, but its biggest limitation is longer operation time and a steep learning curve [919]. On the other hand, the safety of PVP with KTP laser (532 nm wavelength) and its effectiveness is well established and has the advantage of treating patients on anticoagulant and antiplatelet agents [20]. Due to a high affinity for Hb, it has good hemostasis property with low morbidity, good medium term results, and small learning curve but prolong operative time [1621]. On the contrary, newly developed diode lasers are less known to the world. They are semiconductors that generate and emit monochromatic light, which on passing through a crystal leads to the final wavelength [11]. Multiple diode lasers of different wavelengths (940, 980, or 1,470 nm) are available. Unlike KTP laser, 980 nm wavelength diode laser has the highest simultaneous absorption of water and Hb, leading to better and quick tissue ablation with excellent hemostasis [12]. These lasers have a major disadvantage of near-infrared wavelength which causes coagulation necrosis due to deep optical penetration. Dysuria, sloughing, and long-lasting storage symptoms occur due to the necrotic tissue [22]. To overcome this, new diode laser systems are designed to reduce depth of penetration by modulation of their frequency, pulsation, power, and fiber design. A quartz head contact laser fiber was introduced to reduce penetration depth, leading to a decrease in incidence of dysuria from 42% to 17%, and in the passage of slough from 52% to 16% [23]. The diode laser can be applied continuously or in pulsed mode. We used the continuous-wave mode with newly designed twister fiber. Fiber modifications led to a significant reduction in surgical time [23]. Wendt-Nordahl et al. [12] extensively studied diode laser. Various characteristics of KTP lasers (532 nm and 80 W) were compared with diode laser (980 nm and 120 W) in a well-established, isolated, perfused porcine kidney model. The diode laser has a thinner coagulation zone (290.1 µm vs. 666.9 µm; p<0.05) and tissue ablative properties were 7.24 g/10 min, nearly double that of KTP laser (3.99 g/10 min). This is lesser than in TURP, which has a resection capacity of 8.28 g/30 s. They reported parallel bleeding rates (0.21 vs. 0.14 g of Hb/min). The diode laser has coagulation rim of 0.5 mm (range, 0.2–1 mm) in prostate tissue and does not have any areas of hemorrhage [24]. As energy is mainly absorbed at the surface of prostatic tissue, it provides larger ablative and better hemostatic properties, even in patients who are on oral anticoagulation. Therefore, there is no need to discontinue anticoagulant therapy before procedure [12]. In the diode laser at 980 nm, the speed of vaporization does not depend on the tissue being mucosa or fibromuscular stroma, which is not the case with other lasers [2425]. Furthermore, diode laser also has the advantage of lower energy consumption and does not require high voltage connection, improving mobility of the laser generator, as compared to KPT and Ho: YAG laser devices [2627]. Although above evidence is highly suggestive that 980 nm diode laser is a novel technology for laser prostectomy, but in terms of surgical outcome, evidence is still sparse. Hundred patients were included in this study who underwent diode laser PVP and significant improvements in mean IPSS, Qmax & PVR were observed, and results are comparable to the similar case series (Table 5) [242528]. In recent years a few clinical trials with different techniques of diode laser enucleation have been reported [2930], comparing diode laser enucleation of the prostate with bipolar TURP and reported equal improvement in functional outcomes with shorter hospital stay and catheterization time in patients who were treated with diode laser enucleation. However, there are only two randomized clinical trial reports on efficacy and safety of diode LVP in comparison with TURP. Both studies revealed that PVP with a diode laser is effective and a safe alternate to TURP for the treatment of BPH. PVP has the advantage of shorter catheterization time and hospitalization, and no need for discontinuation of anticoagulant therapy [2627]. The literature has reported high rates of dysuria and burning micturition [152627]. In this study, dysuria and burning micturition were 29% and 35% respectively. Furthermore, few studies have also reported high re-operation rates (8%–33%) and persisting stress urinary incontinence (9.1%) [1526]. We did not encounter this in this study. As with any other laser vaporization technique, diode laser also has same limitation of lack of tissue retrieval for histopathology [9]. Therefore patients must be evaluated for prostate cancer prior to diode laser vaporization through prostate specific antigen, digital rectal examination, and prostate biopsy wherever indicated. We excluded all patients who had clinical suspicion of prostate cancer. Another drawback of diode laser is the cost. Although it costs less compared to other lasers treatment for BPH but is still more expensive than TURP. In The Kidney Centre Post Graduate Training Institute, diode laser is 30% more expensive than TURP. There are a few limitations in our study. Preoperative and postoperative sexual dysfunction was not included in the study protocol. Other limitations were lack of long-term follow-up and unavailability of late complication data. Due to inappropriate selection of patients in initial days of our learning curve, 9 patients were converted to TURP due to very large prostate size (Table 4).
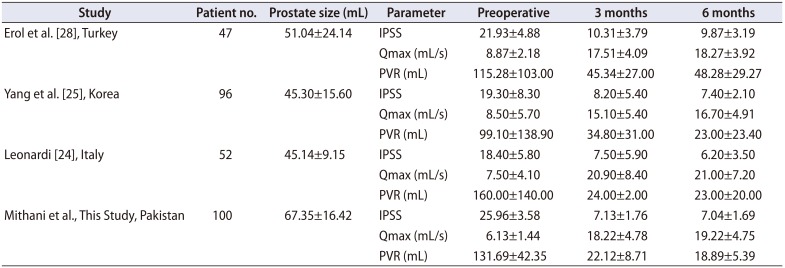
Table 5
Study outcomes comparison with other studies
| Study | Patient no. | Prostate size (mL) | Parameter | Preoperative | 3 months | 6 months |
|---|---|---|---|---|---|---|
| Erol et al. [28], Turkey | 47 | 51.04±24.14 | IPSS | 21.93±4.88 | 10.31±3.79 | 9.87±3.19 |
| Qmax (mL/s) | 8.87±2.18 | 17.51±4.09 | 18.27±3.92 | |||
| PVR (mL) | 115.28±103.00 | 45.34±27.00 | 48.28±29.27 | |||
| Yang et al. [25], Korea | 96 | 45.30±15.60 | IPSS | 19.30±8.30 | 8.20±5.40 | 7.40±2.10 |
| Qmax (mL/s) | 8.50±5.70 | 15.10±5.40 | 16.70±4.91 | |||
| PVR (mL) | 99.10±138.90 | 34.80±31.00 | 23.00±23.40 | |||
| Leonardi [24], Italy | 52 | 45.14±9.15 | IPSS | 18.40±5.80 | 7.50±5.90 | 6.20±3.50 |
| Qmax (mL/s) | 7.50±4.10 | 20.90±8.40 | 21.00±7.20 | |||
| PVR (mL) | 160.00±140.00 | 24.00±2.00 | 23.00±20.00 | |||
| Mithani et al., This Study, Pakistan | 100 | 67.35±16.42 | IPSS | 25.96±3.58 | 7.13±1.76 | 7.04±1.69 |
| Qmax (mL/s) | 6.13±1.44 | 18.22±4.78 | 19.22±4.75 | |||
| PVR (mL) | 131.69±42.35 | 22.12±8.71 | 18.89±5.39 |
![]()
Go to :
 XML Download
XML Download