

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Transrectal ultrasonography (TRUS) guided prostate biopsy is usually performed when prostate cancer (PCa) is clinically suspected, such as when prostate-specific antigen (PSA) is high, a nodule is palpable on digital rectal exam, or a hypoechoic lesion is visible on ultrasonography (US). However, TRUS guided biopsies frequently fail to detect aggressive tumors or provide reliable parameters for pretreatment risk stratification due to its inherent limitations [1]. In addition, low PCa detection rates of repeat biopsies or patients with anterior lesions have also been pointed out as limitations of classical TRUS guided transrectal prostate biopsies [2].
Since the introduction of prostate imaging reporting and data system (PI-RADS) version 2 in 2015, several studies using multiparametric magnetic resonance imaging (mpMRI) with targeted biopsy have been reported [3]. However, without fusion TRUS, MRI-guided biopsy is not commonly used [45]. In addition, so far, US targeted biopsies cannot replace systematic biopsies because it is difficult to detect every clinically significant prostate cancer (csPCa) using US alone [6]. In this regard, magnetic resonance imaging and ultrasonography (MRI-US) fusion allows MRI information to be used for direct biopsy needles under TRUS guidance. This has the advantage of combining the superior diagnostic accuracy of MRI for targeting suspicious lesions with the practicality and familiarity of TRUS [7].
The ultimate aim of biopsy is to increase the detection rate of csPCa and lower the detection rate of insignificant PCa. Therefore, several institutions introduced MRI-US fusion biopsy where most used fusion biopsy through the transrectal approach [3]. Recently, Shoji et al. [7] reported promising results of transperineal MRI-US fusion biopsy. In their report, overall cancer detection rate was 70% and the median rates of the detection of biopsy proven significant cancer in targeted biopsies were 34.1%. Especially, cancer detection rates for PI-RADS 4 and 5 were 33.3% and 88.9%, respectively. However, to our knowledge, there have been no prior reportings of transperineal MRI-US fusion biopsy in Korea. So, herein, we describe our techniques of transperineal MRI-US fusion biopsy and report early results of 75 patients.
Go to : 
MATERIALS AND METHODS
1. Population
This study was approved by the Institutional Review Board of Korea University Medical Center (approval number: 2018AN0339) and informed patient consent for research was obtained from all patients prior to MRI fusion transperineal prostate biopsy. Between February 2018 and May 2018, 75 patients were recruited prospectively for MRI-US fusion transperineal biopsy. MRI was performed in patients who were clinically suspicious for PCa (a PSA greater than 4.0 ng/mL and less than 20 ng/mL or a visible hypoechoic lesion on TRUS or a palpable nodule upon digital rectal examination). Fifty-seven patients had no prior history of prostate biopsy. Eighteen patients had a history of one or more previous systemic transrectal prostate biopsies. Both groups were included in our study.
2. Description of biopsy techniques
1) mpMRI and fusion biopsy device
All mpMRI images include a T2WI (ideally 3 plane), a dynamic contrast enhancement T1WI (to a max B-value of 1,400 s/mm2 or greater), a diffusion WI and/or an apparent diffusion coefficient mapping. MRI images were reviewed by a senior radiologist and classified according to PI-RADSv2. The MRI-US fusion device used in our study was BioJet (Geoscan, Lakewood Ranch, FL, USA) which had previously been approved for clinical use by the U.S. Food and Drug Administration. MRI stored in the database of our institute were imported into the fusion system via either a thumb drive or the localized network system. The contour of the loaded mpMRI would then be drawn and computed to recreate a three-dimensional (3-D) model. Real-time TRUS would then be superimposed enabling us to visualize the region of interest (ROI) on the sonography.
2) Biopsy protocol
Prebiopsy MRI is performed to identify targets. After marking the prostate contour and ROI lesion, the fusion system blends both data sets of MRI and sonography. Then according to the MRI–derived targets on the transrectal US screen, biopsy was proceeded through a grid navigation on the US screen. Biopsies were performed by 3 urologists of varying years of experience in transperineal mapping who were all assessed to be competent in targeted biopsies.
Under monitored anesthesia care (MAC), patients were placed in the lithotomy position and the scrotum was supported with adhesive tape. Afterwards, a bi-planer 7.5 MHz ultrasound transducer was inserted transrectally (Fig. 1A). Finally, the probe was attached to a brachytherapy grid with 5-mm spacing and cradle. An 18-G automatic biopsy gun with a specimen size of 22 mm (Bard Magnum; Bard Medical, Covington, GA, USA) was used to extract biopsy cores (Fig. 1B).

On the workstation, the operator fused the real-time TRUS image and 3-D MRI model that included the prostate contour and ROI. Using an US probe which senses the 3-D movement, the 2-D image created from the 3-D MRI model synchronously moves with the real-time TRUS image. Biopsy was performed using MRI-TRUS fusion image navigation. The operator started with biopsies targeting the center of the ROI, and then moved on to the 12 systematic biopsies. Using the interactive needle guiding system, the biopsy template coordinates were shown on the monitor when the operator marked the target point of the ROI on the workstation. Subsequent insertion of the needle at the template coordinates and retrieval of prostate specimens were carried out by viewing the sagittal image of the prostate (Fig. 2). Immediately after each biopsy, the spatial punctured needle orbits were recorded on the 2-D TRUS image of the axial and sagittal plane, and on the 3-D MRI model (Fig. 3).
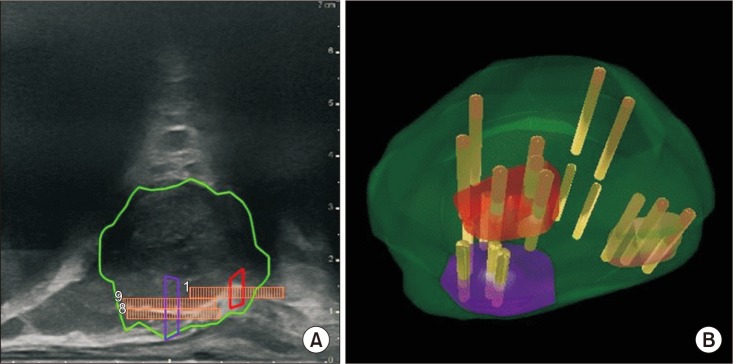 | Fig. 2(A) Sagittal Real-time US targeting of the ROI. ROI 1 (red), ROI 2 (purple), and prostate contour (green). Note that the 3-D model is made, demonstrating the biopsy tract (yellow rod). (B) A 3-D magnetic resonance imaging model assembled by axial and sagittal plane images. ROI, region of interest; 3-D, three-dimensional.
|
 | Fig. 3(A) A 69-year-old man with prostate-specific antigen (PSA) 8.7, Gleason 4+3 cancer in 5 core after initial biopsy. Left transitional lesion of highest suspicion identified on multiparametric magnetic resonance imaging (arrows). (B) A 67-year-old man with PSA 5.6, Gleason 3+3 cancer in 2 core after initial biopsy (from left to right; T2-weighted image, Apparent-diffusion coefficient, dynamic contrast enhancement T1WI) (arrows).
|
3. Outcomes
We investigated the overall cancer detection rate and csPCa detection rate. csPCa missed by either targeted biopsy or systematic biopsy were also evaluated. In addition, cancer detection rate and csPCa detection rate according to PI-RADS score were analyzed. The overall and csPCa detection rate between initial and repeat biopsies were also evaluated. A csPCa was defined as ≥Gleason's score (GS) 7 (3+4).
4. Statistical analysis
Analysis of patient demographics along with clinical and pathologic variables using descriptive statistics was performed. For categorical variables, Fisher's exact test and chi-square test were used for statistical analysis and are specified as percentage. Statistical analysis was done using IBM SPSS Statistics ver. 20.0 software (IBM Co., Armonk, NY, USA). A p-value of <0.05 was considered statistically significant.
Go to :
RESULTS
A summary of patient demographics is presented in Table 1. A total of 75 patients clinically suspected for PCa underwent mpMRI and subsequent categorization according to PI-RADS classification of 1 to 5. The mean age of the 75 patients was 68.8 years (range, 49–83 years). The mean preoperative PSA value was 12.7 ng/mL (range, 2.5–82.6 ng/mL). The mean preoperative prostate volume was 43.4 mL (range, 7.8–154.8 mL). The mean biopsy time was 37.1 minutes which accounts for the MRI-TRUS fusion time and needle puncture time. The mean biopsy cores taken per patient was 18.3. For target biopsies, 3–5 cores were regularly taken per target lesion. The mean core number per ROI was 4.6 cores.

Table 1
Patient characteristics
![]()
Comparative results between systematic biopsy and targeted biopsy are summarized in Table 2. The overall detection rate of PCa was 61.3% (46/75 patients). The detection rate of PCa and csPCa were both significantly higher in targeted biopsies than in systematic biopsies (PCa detection rate, 57.3% vs. 41.3%; p<0.05. csPCa detection rate, 41.3% vs. 26.7%; p<0.05). Three cases of target biopsy missed but detected by systematic biopsy were all non-significant cancers. On the other hand, 15 cases were systematic biopsy missed but target biopsy proven PCas in which seven were significant cancers.

Table 2
Comparative results between systematic biopsy and targeted biopsy
![]()
A summary of csPCa detection according to PI-RADS score is presented in Table 3. Cancer detection rates with corresponding PI-RADS score results showed an overall cancer detection rate of 61.3% (46 patients among 75). Detection rate of csPCa, defined as PCa Gleason's score of 7 or more, was 42.7% (32 among 75 patients). Specifically, detection rates for PI-RADS score 4 and 5 were 44.8% and 84.2%, respectively. There were no csPCa that were ‘missed’ or not detected via targeted biopsy but detected with systematic biopsies. In contrast, the rate of csPCa that were missed by systematic biopsies was 25.0% (8 out of 32 diagnosed csPCa patients).

Table 3
Detection of csPCa by targeted biopsy for 75 patients according to PI-RADS score and zonal anatomy
![]()
In addition, the PCa detection rate was derived according to zonal anatomy of the prostate and the corresponding PI-RADS scores (Table 3). The rate of cancer detection in the peripheral zone and transitional zone was 58.1% and 53.1%, respectively. Multiple ROI lesions that were simultaneously identified in the transitional and peripheral zone of the MRI resulted in a cancer detection rate of 66.7%. Regardless of the zonal lesion, a PI-RADS score of 5 showed obviously higher rates of cancer detection (89.5%, n=17/19) compared to PI-RADS 3 or 4.
Comparative results between initial biopsies and repeat biopsies are summarized in Table 4. The total number of patients without prior history of prostate biopsy was 57 patients (76.0%) while 18 patients (24.0%) had at least one prior history of prostate biopsy. There were no significant differences in the age, PSA, PSA density or number of anterior portion cancer lesions between the two groups. Prostate size was significantly larger in the repeat biopsy group (39.8 mL for first biopsies vs. 54.7 mL for repeat biopsies, p<0.05). There was a tendency for ROI lesions in repeat biopsies to be located in the anterior portion, but there was no statistical significance (p=0.103). PCa detection rate and csPCa detection rate for repeat biopsies were 61.1% and 55.6% and showed no significant difference from initial biopsies.

Table 4
First biopsy vs. repeat biopsy results
![]()
Go to :
DISCUSSION
The current initial standard biopsy for diagnosing Pca in men at risk is a TRUS guided 10–12 systematic biopsy. However, this test is most oftenly performed without visualization of the tumor location, inevitably leading to a 10–12 core random prostate biopsy. A number of studies reported high sensitivity and specificity of mpMRI with further introduction into the methods of MRI targeted prostate biopsy [891011]. The advantage of MRI-US fusion biopsy is that it combines the superior diagnostic accuracy of MRI with the familiarity of transrectal US biopsy [7]. Although overall cancer detection rate should seem to be higher in MRI-US fusion targeted biopsy than in systematic biopsy, several studies have shown inconsistent results [12]. Meanwhile, in regard to the detection of clinically significant cancer, relatively consistent results have been reported. Detection of clinically significant cancers seem to be higher in MRI-US fusion targeted biopsies than in standard biopsies. Valerio et al. [13] reported that MRI-US fusion targeted biopsies detect more clinically significant cancers (median, 33.3% vs. 23.6%) compared with standard biopsy techniques. MRI-US fusion targeted biopsy was able to detect some clinically significant cancers that would have been missed by using only standard biopsy (median, 9.1%; range, 5%–16.2%). In our study, the detection rate of PCa and csPCa were both significantly higher in targeted biopsies than in systematic biopsies (PCa detection rate, 57.3% vs. 41.3%; p<0.05. csPCa detection rate, 41.3% vs. 26.7%; p<0.05). In addition, three cases of target biopsy missed but detected by systematic biopsy were all non-significant cancers. On the other hand, 15 cases of systematic biopsy missed but detected by target biopsy consisted of seven significant and eight insignificant cancers. Therefore, MRI-US fusion targeted biopsy may improve the detection of high risk cancer and may also provide benefit in risk stratification.
Current National Comprehensive Cancer Network and European Association of Urology guidelines suggest that performing mpMRI before repeat biopsy and targeting of ROI during repeat biopsy should be considered [1415]. Schoots et al. [3] reported that MRI-US biopsies improved the detection rate of csPCa in patients with previous negative biopsies over initial biopsies (relative sensitivity, 1.54; 95% confidence interval [CI], 1.05–2.57 vs. 1.10; 95% CI, 1.00–1.22). In traditional TRUS guided biopsy, the peripheral zone is mainly targeted, since it is closer to the rectum and 70%–80% of tumors are located in this region. Due to the relative size of the TZ and difficulty of adequate sampling through a transrectal approach, in the setting of a primary biopsy, cancer detection rates upon TZ sampling have ranged from 1.8% to 4.3%, suggesting a limited role for routine use of anterior and central gland biopsy [161718]. As a result, anterior tumors are likely to be missed at random transrectal US–guided biopsies [19] and the paucity of anterior gland sampling explain the elevated false negative rate, reported to be as high as 47% [20]. In our study, the PCa detection rate of patients in repeat biopsies was 61.1% (11 patients among 18). Taking into account that second and third biopsy results are reported to be approximately 24% and 17%, respectively [21], the PCa detection rate of repeat biopsies was relatively high. In this study, the mean prostate size in repeat biopsy patients was larger than in initial biopsy patients (39.8 mL vs. 54.7 mL). In addition, the percentage of anterior tumor location seemed to be higher in repeat biopsies (35.1% vs. 55.5%). Thus, it is reasonable to consider MRI fusion biopsy in patients who are clinically suspicious for PCa and have a large prostate size because random systematic biopsy has a higher probability to miss the cancer in large sized prostate patients. In addition, patients with prior history of biopsy tend to have a higher rate of anterior located tumor, even though statistically insignificant. Therefore, a transperineal approach might be able to increase the detection of tumor in this location; however, there have been no comparative studies between transrectal fusion and transperineal fusion biopsies so far. Future comparative studies with larger numbers of patients are needed to figure out whether if the transperineal approach is superior to the transrectal approach in detecting tumors located in the anterior portion of the prostate.
As we have seen, MRI-US fusion biopsy improves detection of csPCa, but it remains questionable whether if it can replace systematic biopsy. In overall, data of MRI-US fusion biopsies in the initial biopsy setting are yet insufficient [22]. Baco et al. [23] reported a randomized controlled trial to evaluate ef f icacy of a two core targeted prostate biopsy with traditional 12-core biopsy. The detection rate in overall and in csPCa showed no significant differences between the two groups (p=0.4, p=0.2, respectively). Especially in PI-RADS score 4%5, 97% of the patients were detected by targeted biopsy, thus giving some rationale to the assumption that targeted biopsy alone could replace systematic biopsy in PI-RADS 4–5. Shoji et al. [7] also reported 100% cancer detection rate in PI-RADS 5 at the peripheral zone. In our study, the detection rate of PI-RADS 4 and 5 were 70.0% and 89.5%, respectively. Especially, only in two cases of PI-RADS 5 were shown to have no tumor in the final pathologic report and remain in question whether they were missed cancer lesions or radiologic reading errors. Therefore, more extensive studies should be performed to evaluate MRI-US fusion target biopsy alone in PI-RADS 5 of the peripheral zone as a candidate for the replacement of combined systematic and target biopsy.
There are several limitations to this study. First, the reproducibility of the transrectal US findings is operator dependent. The literature suggests that differences in PCa detection rates by transrectal US among operators are probably related to differences in expertise and/or technique [24]. Therefore, standardization of techniques is required for successful biopsy. Next, the present study did not compare biopsy results with pathological findings from whole-gland specimens. Therefore, although locations and pathological grades of clinically significant cancers and index lesions corresponded with the targeted biopsy results, it is difficult to exclude the possibility that a clinically important cancer has been missed without pathological analysis of whole-gland specimens. Third, the number of patients included in the present study was small to evaluate the accurate cancer detection rate. In addition, although it has not been specified in the results, there were no complications associated with infection such as UTI or sepsis. The transperineal approach has advantages over transrectal prostate biopsy in aspects of lower risk of sepsis and septic shock. However, we realize that a disadvantage of transperineal prostate biopsy is that it mandates MAC anesthesia. Further research into the risk/benefit for either methods is necessary for adequate patient selection to undergo MRI fusion transperineal prostate biopsy.
Go to :
CONCLUSIONS
The results of our early experience showed that multiparametric MRI-TRUS targeted biopsies result in high overall and csPCa detection rate. Although it may be premature to recommend MRI targeted biopsies in the initial biopsy setting, it could be considered when patients have a large prostate size or an anterior ROI lesion. In addition, as in other studies, our study suggests that multiparametric MRI-TRUS targeted biopsy should be considered in repeat biopsies and in high PI-RADS scores. Before this approach is incorporated into standard practice across all centers, consideration must be given to the need for the required expertise and skills and the current impediments to wider dissemination.
Go to :
 XML Download
XML Download