

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Purpose
This study aimed to evaluate the relation between the degree of wrist joint distraction and postoperative restoration of joint function after performed external fixation with distraction of wrist joint in distal radius fracture.
Methods
This study was conducted retrospectively on 55 patients who underwent reduction using external fixation for distal intra-articular radius fracture from January 2007 to December 2014. The degree of pre- and post-operative distraction was measured radiographically using the carpal height ratio (CHR). For postoperative functional assessment, range of motion of the wrist, Gartland Werley classification, grip strength, and pinch strength were measured.
Results
In the functional assessment based on the Gartland Werley classification, excellent was reported by 31 patients, good; 16 patients, fair; 8 patients, and poor; 0 patients. The mean CHR was 0.519 preoperatively and 0.565 immediately after surgery. The mean postoperative CHR of excellent group was 0.581, demonstrating better clinical outcome in distraction than other groups. Eight case of joint stiffness was manifested when CHR value was lower than 0.54 and only 1 case of joint stiffness was manifested when CHR value was higher than 0.54, showing a tendency for lower incidence of joint stiffness when distracted over 0.54 of CHR.
Conclusion
External fixation after sufficient distraction of the wrist joint produced an excellent outcome in the functional assessment. The better the prognosis in the Gartland Werley classification, the higher the CHR and the group with a CHR greater than 0.54 immediately after surgery showed less joint stiffness than the lower group.
Figures and Tables
 | Fig. 1Carpal height ratio: dividing the distance from the distal radius and the base of the 3rd metacarpal A to the length of the 3rd metacarpal B.
|
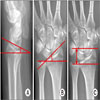 | Fig. 2(A) Distal radius volar tilt: the angle between a line along the distal radial articular surface and the line perpendicular to the longitudinal axis of the radius at the joint margin (normal range, 2°–20°). (B) Radial inclination: the angle between one line connecting the radial styloid tip and the ulnar aspect of the distal radius and a second line perpendicular to the longitudinal axis of the radius (average, 23°). (C) Radial height: the distance between two parallel lines drawn perpendicular to the long axis of the radial shaft, one from the tip of the radial styloid and the other from the ulnar corner of the lunate fossa (average, 12 mm).
|
 | Fig. 3(A) The intraoperative X-ray of an intra-articular distal radius fracture. Preoperative CHR was 0.52. (B) The intraoperative X-ray of an intra-articular distal radius fracture after performed closed reduction by distraction. (C) The intraoperative X-ray of an intra-articular distal radius fracture after applied with external fixator. (D) The postoperative posterior-anterior X-ray of an intra-articular distal radius fracture treated with external fixation. Postoperative CHR was 0.57 and increased about 10%. CHR: carpal height ratio.
|
 | Fig. 4The CHR was increased by 11% postoperatively, and the carpal height ratio decreased with time. The CHR was the most decreased after 2 weeks of the external fixation. (A) Preoperative X-ray. CHR=0.52. (B) Postoperative X-ray. CHR=0.58. (C) POD 2 weeks. CHR=0.54. (D) POD 4 weeks. CHR=0.53. (E) POD 6 weeks. CHR=0.52. (F) After external fixation removal. CHR=0.51. CHR: carpal height ratio, POD: postoperative day.
|
 | Fig. 5A 46-year-old female patient was admitted to the hospital with slip down. (A) The posterior-anterior X-ray of an intra-articular distal radius fracture. Preoperative CHR was 0.53. (B) The posterior-anterior X-ray of an intra-articular distal radius fracture treated with spanning external fixation. Postoperative CHR in this case was 0.59 and increased about 11%. CHR: carpal height ratio.
|
 | Fig. 6A 58-year-old male patient was admitted to the hospital with 2-m-high fall down. (A) The posterior-anterior X-ray of an intra-articular distal radius fracture. Preoperative CHR was 0.57. (B) The posterior-anterior X-ray of an intra-articular distal radius fracture treated with spanning external fixation. Postoperative CHR in this case was 0.52 and increased about 9%. CHR: carpal height ratio.
|

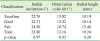
Table 2
Comparison of Carpal height ratio (postoperative) for each group using Tukey honestly significant difference

![]()
References
1. Liporace FA, Adams MR, Capo JT, Koval KJ. Distal radius fractures. J Orthop Trauma. 2009; 23:739–748.

2. Grewal R, Perey B, Wilmink M, Stothers K. A randomized prospective study on the treatment of intra-articular distal radius fractures: open reduction and internal fixation with dorsal plating versus mini open reduction, percutaneous fixation, and external fixation. J Hand Surg Am. 2005; 30:764–772.
3. Wright TW, Horodyski MB, Smith DW. Functional outcome of unstable distal radius fractures: ORIF with a volar fixed-angle tine plate versus external fixation. J Hand Surg Am. 2005; 30:289–299.
4. Schuind F, Donkerwolcke M, Rasquin C, Burny F. External fixation of fractures of the distal radius: a study of 225 case. J Hand Surg Am. 1989; 14:404–407.
5. Capo JT, Rosy W, Henry P, Maurer RJ, Naidu S, Chen L. External fixation of distal radius fractures: effect of distraction and duration. J Hand Surg Am. 2009; 34:1605–1611.
6. Cho DY, Kim JH, Kim H. The effect on the wrist function with the distraction on external fixator in the severe comminuted distal radius fracture. J Korean Soc Surg Hand. 1999; 4:35–41.
7. Youm Y, Flatt AE. Kinematics of the wrist. Clin Orthop Relat Res. 1980; 21–32.
8. Gartland JJ Jr, Werley CW. Evaluation of healed Colles' fractures. J Bone Joint Surg Am. 1951; 33-A:895–907.
9. Kambouroglou GK, Axelrod TS. Complications of the AO/ASIF titanium distal radius plate system (pi plate) in internal fixation of the distal radius: a brief report. J Hand Surg Am. 1998; 23:737–741.
10. Arora R, Lutz M, Hennerbichler A, et al. Complications following internal fixation of unstable distal radius fracture with a palmar locking-plate. J Orthop Trauma. 2007; 21:316–322.
11. Rozental TD, Blazar PE. Functional outcome and complications after volar plating for dorsally displaced, unstable fractures of the distal radius. J Hand Surg Am. 2006; 31:359–365.
12. Kapoor H, Agarwal A, Dhaon BK. Displaced intra-articular fractures of distal radius: a comparative evaluation of results following closed reduction, external fixation and open reduction with internal fixation. Injury. 2000; 31:75–79.
13. Margaliot Z, Haase SC, Kotsis SV, Kim HM, Chung KC. A meta-analysis of outcomes of external fixation versus plate osteosynthesis for unstable distal radius fractures. J Hand Surg Am. 2005; 30:1185–1199.
14. Ahlborg HG, Josefsson PO. Pin-tract complications in external fixation of fractures of the distal radius. Acta Orthop Scand. 1999; 70:116–118.
15. Jonsson U. External fixation for redislocated Colles' fractures. Acta Orthop Scand. 1983; 54:878–883.
16. Roumen RM, Hesp WL, Bruggink ED. Unstable Colles' fractures in eldery patients. J Bone Joint Surg Br. 1991; 73:307–311.
17. Kaempffe FA. External fixation for distal radius fractures: adverse effects of excess distraction. Am J Orthop (Belle Mead NJ). 1996; 25:205–209.
18. Biyani A, Simison AJ, Klenerman L. Fractures of the distal radius and ulna. J Hand Surg Br. 1995; 20:357–364.
19. Papadonikolakis A, Shen J, Garrett JP, Davis SM, Ruch DS. The effect of increasing distraction on digital motion after external fixation of the wrist. J Hand Surg Am. 2005; 30:773–779.
20. Loebig TG, Badia A, Anderson DD, Baratz ME. Correlation of wrist ligamentotaxis with carpal distraction: implications for external fixation. J Hand Surg Am. 1997; 22:1052–1056.
 XML Download
XML Download