

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Hamate bone fracture is an uncommon injury, accounting for 2% of all carpal bone fractures. The common treatment of choice for hamate bone fractures is conservative treatment or excision of the hamate fracture fragment. We devised a new procedure that utilizes dorsal percutaneous compression screws for internal fixation. This technique was performed on two patients with left hamate hook base fractures. Tolerable active joint movement of the left wrist and fingers was permitted the first day post-surgery. Radiographs were taken after surgery, at 3 months, and at 6 months to determine the degree of union. No remarkable ligament injuries or nerve injuries were observed. This technique proved to be a relatively simple procedure when compared to the existing procedure while enabling early wrist movement. By preserving soft tissue, this procedure maintained blood supply decreasing risks of non-union. These advantages make this technique a recommendable new procedure for hamate hook fractures.
Figures and Tables
 | Fig. 1A 39-year-old woman. Preoperative plain radiographs of left wrist. Anteroposterior and lateral radiographs and computed tomography axial view shows that hamate bone hook fracture.
|
 | Fig. 2Intraoperative photographs shows positioning of the hook area of hamate bone in to a round circle from the dorsal approach utilizing the C-arm guide pin insertion through the center of the hamate bone hook after previous positioning.
|

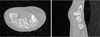
 | Fig. 5A 45-year-old man. Preoperative plain radiographs of left wrist. (A) Anteroposterior and lateral radiographs show scaphoid and hamate bone fracture. (B) Computed tomography axial view shows that scaphoid and hamate bone hook fracture.
|


References
1. Milch H. Fracture of the hamate bone. J Bone Joint Surg. 1934; 16:459–462.
2. Dobyns JH, Linscheid RL, Cooney WP 3rd. Fractures and dislocations on the wrist. In : Rockwood CA, Green DP, editors. Fractures in adults. 2nd ed. Philadelphia, PA: Lippincott Williams & Wilkins;1984. p. 411–451.
3. Stark HH, Jobe FW, Boyes JH, Ashworth CR. Fracture of the hook of the hamate in athletes. J Bone Joint Surg Am. 1977; 59:575–582.

4. Whalen JL, Bishop AT, Linscheid RL. Nonoperative treatment of acute hamate hook fractures. J Hand Surg Am. 1992; 17:507–511.
5. Watson HK, Rogers WD. Nonunion of the hook of the hamate: an argument for bone grafting the nonunion. J Hand Surg Am. 1989; 14:486–490.
6. Demirkan F, Calandruccio JH, Diangelo D. Biomechanical evaluation of flexor tendon function after hamate hook excision. J Hand Surg Am. 2003; 28:138–143.
7. Foucher G, Schuind F, Merle M, Brunelli F. Fractures of the hook of the hamate. J Hand Surg Br. 1985; 10:205–210.
8. Marchessault J, Conti M, Baratz ME. Carpal fractures in athletes excluding the scaphoid. Hand Clin. 2009; 25:371–388.
9. Smith P 3rd, Wright TW, Wallace PF, Dell PC. Excision of the hook of the hamate: a retrospective survey and review of the literature. J Hand Surg Am. 1988; 13:612–615.
10. Bishop AT, Beckenbaugh RD. Fracture of the hamate hook. J Hand Surg Am. 1988; 13:135–139.
 XML Download
XML Download