

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Abstract
Triceps tendon avulsion from the olecranon is a rare injury. Missed or delayed diagnosis may result in a weakness of strength or a decreased range of motion of the elbow. This injury is usually caused by a fall on the outstretched hand or a direct blow to the posterior arm. In addition, the rupture of the triceps tendon is implicated by a sudden eccentric contraction of the triceps muscle. To determine whether the rupture is complete or incomplete is critical to guide the treatment method. A small avulsed fragment from the olecranon may be detected on lateral radiographs of the elbow. We report three cases of the triceps tendon avulsion with a bony flake from the olecranon, which were surgically treated, along with a brief review of the literature.
Figures and Tables
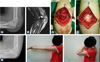
Fig. 1
(A) Lateral radiograph with an avulsed fragment posterior to elbow joint. (B) magnetic resonance imaging shows a diffuse subcutaneous contusion and combined hematoma at posterior aspect of left elbow. The triceps tendon is avulsed from the olecranon. (C) Intraoperative photograph shows a complete avulsion of triceps tendon. (D) Avulsed tendon is repaired on the olecranon using a Krachow-type suture. (E) Radiograph performed at 28 months follow-up shows a bony union of avulsed fragment. (F, G) Clinical photos show a normal range of motion of left elbow at final follow-up.

References
1. Anzel SH, Covey KW, Weiner AD, Lipscomb PR. Disruption of muscles and tendons; an analysis of 1, 014 cases. Surgery. 1959. 45:406–414.
2. Mair SD, Isbell WM, Gill TJ, Schlegel TF, Hawkins RJ. Triceps tendon ruptures in professional football players. Am J Sports Med. 2004. 32:431–434.

3. Yeh PC, Dodds SD, Smart LR, Mazzocca AD, Sethi PM. Distal triceps rupture. J Am Acad Orthop Surg. 2010. 18:31–40.
4. van Riet RP, Morrey BF, Ho E, O'Driscoll SW. Surgical treatment of distal triceps ruptures. J Bone Joint Surg Am. 2003. 85:1961–1967.
5. Downey R, Jacobson JA, Fessell DP, Tran N, Morag Y, Kim SM. Sonography of partial-thickness tears of the distal triceps brachii tendon. J Ultrasound Med. 2011. 30:1351–1356.
6. Bach BR Jr, Warren RF, Wickiewicz TL. Triceps rupture. A case report and literature review. Am J Sports Med. 1987. 15:285–289.
7. Lambers K, Ring D. Elbow fracture-dislocation with triceps avulsion: report of 2 cases. J Hand Surg Am. 2011. 36:625–627.
8. Farrar EL 3rd, Lippert FG 3rd. Avulsion of the triceps tendon. Clin Orthop Relat Res. 1981. (161):242–246.
9. Weng PW, Wang SJ, Wu SS. Misdiagnosed avulsion fracture of the triceps tendon from the olecranon insertion: case report. Clin J Sport Med. 2006. 16:364–365.
 XML Download
XML Download