

 PDF
PDF ePub
ePub Citation
Citation Print
Print



I. Introduction
Temporomandibular disorders (TMDs) refer to a group of musculoskeletal disorders affecting the masticatory muscle and/or the temporomandibular joint (TMJ)1. Reportedly, 33% to 86% of individuals exhibit at least one sign of TMD, and 16% to 59% have at least one symptom234. Although the etiology of TMDs is not completely known, different factors such as occlusion, parafunction, emotional stress, hormones, physical trauma, microtrauma to the teeth, joint hypermobility, and dental treatments requiring extensive chair time have been considered in the etiology of TMDs in various studies5678910. Estrogen and progesterone receptors were detected in the human TMJ disc, suggesting that changes in reproductive hormones may play a role in the pathogenesis of joint disorders11. Therefore, hormonal changes in women during menopause may alter their susceptibility to joint disease.
Information regarding the role of female sexual hormones in the etiology of joint diseases is contradictory in the literature. Some studies have shown that estrogen is necessary for an intact TMJ structure121314151617. Madani et al.12 found the level of progesterone to be lower in a group of women with TMJ clicking; however, the estrogen level was the same in the patient and control groups. In another study, Abubaker et al.13 found that estrogen is necessary for development of collagen and protein in the structure of TMJ in rats. However, in other studies, a higher prevalence of TMDs with increased estrogen level was reported1617.
Several indices have been developed to assess the prevalence and severity of signs and symptoms of TMDs181920. One of the most feasible was developed by Helkimo20; the Helkimo clinical dysfunction index (Di) assesses the prevalence and severity of signs and symptoms in patients with TMD20.
A significant reduction in gonadal hormones occurs in postmenopausal women and is responsible for many disorders such as cardiovascular disease and neurologic disease2122. Although the relationships between menopause and certain joint diseases such as postmenopausal osteoarthritis and rheumatoid arthritis are known, information regarding the prevalence of TMDs in menopausal women is limited in the litrature2324. Therefore, in the present study, the prevalence and severity of TMDs were assessed using the Helkimo Di in menopausal and non-menopausal women who were referred to Shiraz Dental School for a consultation from February to November 2015.
II. Materials and Methods
This study was approved by the Ethical Committee of Shiraz University of Medical Sciences (approval no. 1479). The informed consent was waived for this retrospective study. A cross-sectional study was performed in 140 women 45 to 55 years of age who were referred to the prosthodontics department of Shiraz Dental School (Shiraz, Iran) from February to November 2013. All patients were informed regarding the study and agreed to participate. Menopausal women whose latest menstruation occurred at least 1 year prior or had not used medication containing sexual hormones for the last 3 months were selected. Among non-menopausal women, females who had a normal menstrual cycle and did not use drugs containing sexual hormones for the last 3 months were selected. All the subjects were generally healthy and did not have history of trauma or surgery in the TMJ region.
All participants were evaluated using the Helkimo clinical Di, which has five subscales for assessing clinical signs of TMDs (mobility, TMJ function, muscle pain, TMJ pain, and pain during mandibular movement index).(Table 1)
Finally, the values of the five indices were summed, and patients were classified into 4 groups according to clinical Di.(Table 1)
Clinical examination was performed twice by a trained dental student. All patients were examined on a dental unit using the same calipers and under the same light. Results of the clinical examination were recorded on a standardized chart according to Helkimo20. The data were analyzed using PASW Statistics (ver. 18.0; IBM Co., Armonk, NY, USA) and chi-square and Fisher's exact tests.
III. Results
A total of 140 women, 69 premenopausal (49.3%) and 71 postmenopausal (50.7%), were recruited for this cross-sectional study. The mean age of the menopausal women was 46.87 years, and that of non-menopausal women was 51.34 years.
Based on the Helkimo Di, 49.3% of subjects had no signs of TMD (Di 0), and 50.7% suffered from some degree of TMD (Di I, II, or III). Among menopausal women, 40.8% had mild TMD (Di I), 21.1% moderate (Di II), and 5.6% showed signs and symptoms of severe TMD (Di III). Among non-menopausal women, 23.2% had mild TMD (Di I), 7.2% moderate (Di II), and 2.9% suffered from severe TMD (Di III).(Table 2) TMD occurrence was significantly higher in menopausal women than non-menopausal women (P<0.001). The odds ratio of TMD occurrence between menopausal and non-menopausal women was 4.17.
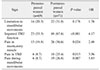
The prevalence of clinical signs and symptoms of TMDs in menopausal women is summarized in Table 3. Among these clinical signs and symptoms, pain in the TMJ and pain during mandibular movements were the least prevalent findings in menopausal and non-menopausal women, respectively. The most common finding in both groups was minor problems in TMJ function and was approximately 2 times more common in menopausal women than non-menopausal women. All TMD criteria based on Helkimo Di, except range of mandibular movement, were significantly more common in menopausal women.
IV. Discussion
Based on the results from this study, occurrence of TMDs was significantly more frequent in menopausal women than non-menopausal women; except for minor problems in mandibular movement (P=0.178), all other Helkimo indices were significantly higher in menopausal women. LeResche et al.25 reported the highest TMD pain level in women when estrogen was at its lowest level during the menstrual cycle. In another study, Haskin et al.26 showed an inverse relationship between blood estrogen level and joint pain, which is in agreement with the current study results.
Some studies272829 have shown that estrogen has an important role in the development of TMJ structure. Yasuoka et al.15 showed that ovarian hormone deficiency in ovariectomized rats resulted in destructive changes to the TMJ structure, which could be prevented by estradiol replacement. Reportedly, estrogen deficiency in rats during puberty changes serum calcitonin and parathyroid hormone levels, causing alterations in rat TMJ structure14. In another study, Abubaker et al.13 showed the necessity of estrogen for development of collagen and protein in the structure of the TMJ disc of the rat. Regarding these findings, reduction in estrogen level during menopause may result in less development of the TMJ structure; therefore, increased severity and prevalence of TMDs in menopausal women could be expected based on the results from these studies.
In addition, anti-nociceptive and inflammatory effects of estradiol, the most common form of estrogen, have been demonstrated in several studies2728. Fischer et al.27 showed that nociceptive behavior induced by injection of formalin or glutamate into the TMJ is higher at low serum estradiol level in female rats, and vice versa. Torres-Chávez et al.28 found that estradiol reduces plasma extravasations and neutrophil migration, two parameters of TMJ inflammation. This anti-inflammatory effect of estradiol reduces damage to the TMJ.
Results of several studies have shown that reduction in plasma estrogen level reduced the inflammatory factors in TMJ293031. For example, Yun et al.29 found that estrogen could stimulate expression of proinflammatory cytokines such as interleukin (IL)-6, IL-8, and IL-18, which would increase TMD. Contrary to the present study results, several studies reported TMD increase when sexual hormone levels increase1632. Landi et al.16 found that patients with TMD had significantly higher serum level of estrogen. LeResche et al.32 showed that TMD was less frequent in menopausal women, and use of postmenopausal estrogen increased TMD in women. However, a later study did not show any relationship between estrogen replacement therapy and increased risk of TMD in women33. Dose-dependent effect of estrogen in the physiopathology of TMDs might explain this contrast. In other words, a physiological level of estrogen is necessary for proper development of the TMJ structure, but higher levels could result in inflammation and TMD34. Another reason might be the different criteria used in these studies and current investigation for diagnosis of TMDs1131.
One limitation of this study was lack of measurement of exact hormonal levels in the study participants. Another limitation was the relatively small study group. Although, the number of subjects was adequate for statistical analysis, future studies with a larger cohort of women are recommended for more feasible results.
V. Conclusion
Within the limitations of this study, the prevalence and severity of TMDs were higher in menopausal women than non-menopausal women. Therefore, TMDs, like other common conditions such as arthritis and osteoporosis that affect menopausal women, should be taken into consideration by dental and medical professionals.


 XML Download
XML Download