

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Dietary habits have shifted from eating food for survival in the past to being health conscious in modern society. As consumers' interest in the relationship between food intake and health status has increased, food selection factors are changing from taste, price, and nutrition to health. As a result, dietary supplement use has been increasing significantly throughout the world [1].
Dietary supplements, as defined by the Dietary Supplement Health and Education Act (DSHEA) of 1994 in the US, are products intended to supplement the diet such as vitamins, minerals, amino acids, other dietary substances, and/or herbs or other botanicals [2]. Dietary supplements sales in the US have grown by 10% per year since surpassing $ 17 billion in 2000 [3]. Dietary supplements are commonly used worldwide. For example, dietary supplement use was reported in 48.8% of adults in the US [4], in 45.1% of women and 25.2% of men in the UK [5], and in 49% of adults in Italy [6]. In South Korea, 22.1% of adults reported using the dietary supplements [7], which was lower than that in Western countries. According to the type of dietary supplements, multi-vitamin and minerals (MVMs) were most commonly used (33.5% among supplement users), followed by omega-3/fish oil (17.5%), vitamin C (13.3%), red ginseng (9.0%), and glucosamine/chondroitin (4.0%) [7].
MVM supplements can be used for the purpose of supplying nutrients to people who might lack nutrients in special situations such as patients, pregnant women, or vegetarians [8]. A majority of MVM supplements contain various nutrients. Especially minerals are essential nutrients to maintain life and health, and perform important functions in forming bones and teeth, in maintaining acid-base equilibrium and body fluid balance, and in serving as nerve-stimulating substances and hormone components [9]. Although mineral intake requirements are small, dietary supplements may be used to supply minerals because they are diverse, but it is difficult to meet their requirements only through meals in some populations. When people use dietary supplements, they should consult with health professionals about what nutrients may help maintaining and improving their health. However, dietary supplement users tend to be more high health conscious and follow healthy eating habits and lifestyle, so their supplement use for long periods habitually but without checking on the nutritional status of the supplements may lead to unbalanced nutrition and unhealthy status.
In the current situation of rapid increase in the production and consumption of dietary supplements, the general population uses the supplements without considering proper mineral intakes. Therefore, in order to induce the proper selection of MVM supplements, research on evaluating the kinds and contents of minerals in various dietary supplements is needed.
The purpose of this study was to evaluate the contents of minerals in most commonly sold MVM supplements in South Korea and to compare mineral dose of MVMs with Dietary Reference Intakes (DRIs) by supplement target population.
MATERIALS AND METHODS
Materials
In September fist to the end of October in 2017, we surveyed MVM supplements sold in South Korea through off-line and on-line. Total 149 dietary supplements were identified through the internet search engines (Google, Naver, Daum, and Zum) with search terms of “dietary supplements,” “mineral supplements,” and “MVMs.”
For each dietary supplement, the price, origin, method of administration, dosage, and mineral contents claimed on the label were investigated. Of those 149 dietary supplements, those without mineral or single mineral were excluded from this study, leaving a final analytic sample of 90 MVM supplements.
Analysis of mineral contents in MVMs
Fourteen minerals were found in 90 MVM supplements: calcium, phosphorus, sodium, potassium, magnesium, iron, zinc, copper, manganese, iodine, selenium, molybdenum, chromium, and boron. The price and number of minerals of the 90 MVM supplements was analyzed and compared according to their price per bottle (low, medium, high) and the origin (domestic, imported). The daily supply of 14 minerals from MVM supplements was analyzed and compared according to target population (adults, men, women, and children). Regarding 9 minerals (calcium, magnesium, iron, zinc, copper, manganese, iodine, selenium, and chromium) contained in at least 30% of MVM supplements, the daily dose of each mineral was compared with its DRI by MVM target populations. DRIs used in this study included recommended intake (RI), adequate intake (AI), and tolerable upper intake level (UL). Target reference values used in this study were the DRIs of 19- to 29-year-old men and women, and 3- to 5-year-old children [10].
Statistical analysis
Statistical analysis of all data was conducted using SAS version 9.3 (SAS Institute, Cary, NC, USA). The average and standard deviations for all variables were calculated. As the types of minerals contained in the MVM supplements varied, the number of samples calculating mean contents of each mineral differed. In other words, if an MVM supplement did not contain a certain mineral, the MVM supplements was excluded for calculating average contents of that certain mineral. To determine mean differences in mineral contents of MVM supplements by target populations (adult men, adult women and children), post hoc analysis using Duncan's test was conducted when indicated by analysis of variance test. Statistical significance was determined at a level of p < 0.05.
RESULTS
Mineral contents of MVM supplements
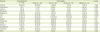
General characteristics and mineral contents of 90 MVM supplements are shown in Table 1. Average price of MVM supplements was $41.3 per bottle, with a price of $0.9 per day and the average number of minerals contained in the MVM supplements was 4.7. There was no significant difference in the number of minerals by the price. Imported MVM supplements were more expensive and contained a higher number of minerals compared with domestic ones.
Table 1
Price and mineral content of multi-vitamin and minerals in the dietary supplements

Values are expressed as means ± standard deviation.
*,†Different marks in a row indicate significant difference determined by Duncan's multiple-range test at p < 0.05.
![]()
Table 2 shows proportions of MVM supplements that contain minerals by MVM target populations. Among the 90 MVM supplements, zinc was found in 85 supplements, manganese in 56 supplements, magnesium in 52 supplements, and calcium in 49 supplements. By target populations, 54 MVM supplements were targeted for adults, 10 for men, 17 for women, and 9 for children. By target populations, iron was found in 58.8% of supplements targeted to women, iodine was found in 80.0% of supplements targeted for men and selenium was found in 82.4% of supplements targeted for women and 80.0% of supplements targeted for men. Mineral number was significantly higher in MVMs for men (5.5) or women (5.7) than for children (3.7). The daily doses of calcium, magnesium, iron, zinc, and iodine were significantly different according to MVM targets. Especially, iron content was the highest in MVMs for women (Table 3).
Table 2
Proportion of MVM supplements containing minerals according to MVM target populations
![]()
Table 3
Daily dose of minerals in the MVM supplements according to MVM target population
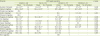
Values are expressed as mean ± standard deviation.
MVM, multi-vitamin and mineral.
*,†Different marks in a row indicate significant difference determined by Duncan's multiple-range test at p < 0.05.
![]()
Daily dose of mineral in the MVMs compared with DRIs
Table 4 shows a daily dose of mineral in the MVM supplements compared with RI or AI according to MVM target populations. Magnesium content was significantly higher in the MVM supplements for adults and iron content was higher in the MVM supplements for women compared with other MVM supplements target population. Figure 1 illustrates percentage of mineral contents compared to RI or AI. In all the MVM supplements, daily dose of calcium was the lowest at 34.0% of the RI, and that of chromium was the highest at 218.7% of AI. Furthermore, daily dose of zinc, copper, selenium, and chromium were higher than their RIs or AI.
Table 4
Percentages of daily dose of minerals in the multi-vitamin and minerals (MVM) supplements compared to reference daily intakes according to MVM target papulation
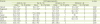
Values are expressed as mean ± standard deviation; Reference daily intakes indicate recommended intake for calcium, magnesium, iron, zinc, copper, iodine, and selenium, and adequate intake for manganese and chromium.
*,†Different marks in a row indicate significant difference determined by Duncan's multiple-range test at p < 0.05.
![]()
 | Figure 1Percentage of daily mineral content in the multi-vitamin and minerals supplements compared to reference daily intakes. Reference daily intakes indicate recommended intake for calcium, magnesium, iron, zinc, copper, iodine, and selenium, and adequate intake for manganese and chromium.Bar graphs are expressed as mean ± standard deviation.
|
DISCUSSION
The purpose of this study was to evaluate the mineral contents of MVM supplements by comparing with their DRIs. This study found that 14 minerals were found in 90 kinds of MVM supplements sold in South Korea and 9 minerals were found in more than 30% of MVM supplements. Compared with their DRIs, daily doses of 9 minerals ranged from 34.0% of RI for calcium to 218.7% of AI for chromium. Additionally, daily doses of zinc, copper, selenium, and chromium were higher than their RIs or AIs.
In the environment of increasing dietary supplement use, Elia et al. [11] conducted a systematic review and found that the use of oral nutritional supplements in community and care homes was associated with clinically relevant benefits such as improved quality of life, reduced infections, and reduced falls, suggesting cost effectiveness. However, Guallar et al. [12] argued that they found no convincing evidence if such dietary supplements provide benefit in well-nourished adults, or could be harmful. In 2010, Americans spent $28.1 billion on dietary supplements [13], and the most popular nutritional supplement was MVMs [14]. In the present study, imported MVMs were more expensive and contained a higher number of minerals than domestic ones. However, there was no significant difference in the number of minerals contained in MVM supplements according to their prices. Because MVM supplements are commonly used by the public in South Korea, and contain various essential nutrients, MVM supplements users should select it based on nutrient contents, considering their own nutritional status rather than price, efficacy, and manufacturer.
It is most desirable that all nutrients, including minerals, are ingested through meals. Based on these assumptions, each country including South Korea has set the DRIs as a national standard of nutrient intake for health [10]. The dietary standard initially established to prevent nutritional deficiencies was the Recommended Dietary Allowance. However, because health problems due to excessive intake or imbalance of nutrients as well as nutritional deficiencies, various DRIs such as Estimated Average Requirement, RI, AI, and UL are provided. Especially, UL is set based on scientific evidence of adverse effects due to excessive intake of nutrients. Exceeding the UL of nutrient intake through a normal diet is rare, but it may occur with high dietary supplement use. Furthermore, this national standard is often not followed by dietary supplement manufacturers who include larger amounts of nutrients in their products than recommended [15].
In this study, daily dose of minerals in the MVM supplements was below UL except for chromium, for which UL has not been established. When daily dose of minerals in the MVMs was compared to their DRIs, that of calcium was the lowest at 34.0% of RI and that of chromium was the highest at 218.7% of AI. In addition, daily doses of zinc, copper, selenium, and chromium were higher than their RIs or AI. These results show that mineral intakes may exceed the adequate level if MVM supplements are used in the situation in which enough minerals are consumed through foods. However, the intake of various minerals is difficult to meet the DRIs such as RI or AI only through foods in some population [1617], so the use of MVM supplements in this situation may be useful for adequate mineral intake. As mineral contents are diverse among the MVM supplements, the supplements should be selected based on the usual mineral intake status of individuals.
In South Korea, the standards and specifications for the mineral contents of health functional foods are set to be similar to DRIs. However, the standard values for the daily dose of minerals in MVM supplements have not been established. Consumers determine the daily dose through the label claims of MVM supplements. However, the actual ingredient contents of MVM supplements might not be consistent with their label claims, because the ingredients might be added in amounts exceeding the label claims in order to compensate for losses during shelf life. The Dietary Supplement Ingredient Database (DSID) provides estimated levels of ingredients in dietary supplement products sold in the US [18]. Recently, DSID-4 reported estimated levels of 11 minerals in the MVM supplements for adults [19]. For chromium, the most common label level per serving in the MVM supplements for adults was 120 µg and the estimated levels were different from the labels ranging from 20% to 40% above the label. Our study also found that the daily dose of chromium in the MVM supplements was the highest among the minerals reaching 218.7% of AI. Chromium is included in the MVM supplements for adults because of its efficacy in improving blood sugar levels and insulin metabolism [20]. However, the UL of chromium has not been set yet, as there is no enough evidence in South Korea. Therefore, it is necessary to pay special attention to the daily dose of chromium from MVM supplements along with providing its standard value in dietary supplements.
This study has several limitations. The number of MVM supplements investigated is small and the mineral contents using label claims of MVM supplements might be different from the actual amount. The evaluation of mineral contents in the MVM supplements is also limited because we did not directly analyze the contents. Nevertheless, this study is meaningful to focus on the MVM supplements commonly sold in South Korea.
CONCLUSION
Ninety MVM supplements commonly sold in South Korea contained 14 minerals. Of those, 9 minerals were found in more than 30% of MVM supplements. When the daily mineral contents of MVM supplements was compared to the DRIs, that of calcium was the lowest at 34.0% of RI and that of chromium was the highest at 218.7% of AI. Additionally, daily doses of zinc, copper, selenium, and chromium were higher than their RI or AI values. There is a great need to educate the public for the adequate selection and use of MVM supplements based on the contents of MVM supplements and individual's mineral intake derived from the diet, because mineral contents in the MVM supplements are wide ranged.
 XML Download
XML Download