

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Dear Editor:
Onychopapilloma is an idiopathic benign neoplasm of the nail matrix and nail bed1. It is a relatively new nail tumor as the term “onychopapilloma” was first established in 2000 by Baran and Perrin1. To date, less than 100 cases have been reported in the literature2. It typically presents as longitudinal erthronychia extending from the lunula to the distal nail. However, clinical diagnosis is often challenging because it frequently resembles other conditions. The majority of cases were reported in Western countries. Reports in Asia have been rare. To our knowledge, only two reports from Korea have been published34.
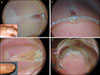
A 62-year-old woman with distal red streaks on her left thumbnail was referred for evaluation. The lesion, which was mildly tender, was noted 15 years prior. On physical examination, a 2-mm longitudinal erythronychia was localized on the distal left thumb. Dermoscopy revealed a homogeneous whitish band from the lunula edge with distal splinter hemorrhages (Fig. 1A). Nail edge dermoscopy showed a localized distal subungual keratosis at the hyponychium (Fig. 1B). Histopathologic examination of excisional biopsy specimen showed an elongated digitating papillomatous acanthotic epidermis, with the superficial layer displaying keratinous zone and ample eosinophilic cytoplasm (Fig. 2). These findings were consistent for onychopapilloma.
Our second case was a 59-year-old woman who presented with a 1-year history of yellowish discoloration and distal onycholysis of the right fifth fingernail. Dermoscopy showed a V-shaped yellowish band extending from the lunula border to the free edge of the nail plate (Fig. 1C). Splinter hemorrhages were present. Nail edge dermoscopy revealed a hyperkeratotic mass lifting the nail plate (Fig. 1D). We received the patient;s consent form about publishing all photographic materials. Histopathologic findings revealed acanthosis and hyperkeratosis with the upper layers of the nail bed containing eosinophilic cytoplasm of which were compatible with onychopapilloma (Supplementary Fig. 1).
Baran and Perrin first reported the condition in 1995 as “localized multinucleate distal subungual keratosis.”5 The term was later replaced with “onychopapilloma” following the histopathologic review of cases with a lack of multinucleate cells in the majority1. Reports on onychopapilloma are limited in the Asian population. In addition to the rarity of this disease, its unfamiliarity may be contributory to the lack of reported cases in Asia.
Onychopapilloma classically presents as localized longitudinal erythronychia, leukonychia, melanonychia, or splinter hemorrhage2. Dermoscopy enables clinicians to observe the detailed morphology of subtle changes within the lesion. Dermoscopic findings of onychopapilloma were recently reported as red bands, keratotic subungual masses, and splinter hemorrhages2. In both our cases, dermoscopy following initial inspection provided further detailed description of morphologic changes due to onychopapilloma. Both cases disclosed white or yellow homogenous bands, splinter hemorrhages, and keratotic subungual masses. The bands were not longitudinal. Although the pathogenesis of onychopapilloma is not fully understood, it is thought to affect the distal matrix23.Therefore, we propose that band sparing of the proximal nail is a distinguishing trait of onychopapilloma.
In conclusion, we report two rare cases of onychopapilloma, which occurred in Asia. Dermoscopic assessment of subtle changes of the nail and its margins facilitates the recognition of onychopapilloma in the clinical setting.

 XML Download
XML Download