

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Desmoplastic fibroblastoma, also known as collagenous fibroma, is a benign fibrous neoplasm composed of spindle to stellate-shaped fibroblasts sparsely distributed in the rich collagenous matrix. Since Evans' first description in 19951, approximately 100 cases of desmoplastic fibroblastoma have been reported in the English literature. It has conventionally been presented as a well-circumscribed, solitary, non-tender, and slow-growing mass in the subcutaneous tissue or intramuscular region23, commonly affecting individuals between the ages of 50 and 70 years4. Desmoplastic fibroblastoma most commonly appears in the arm and shoulder, but it has also been reported to appear on the neck, back, hip, and extremities5. The current treatment of choice is complete surgical excision, and there have not been any reports of recurrence or metastases thus far3. Herein, we report an extraordinary case of desmoplastic fibroblastoma that presented as a tiny painful mass on the scalp with clinical, pathological, and immnohistochemical findings.
CASE REPORT
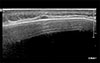
An 82-year-old man presented a tiny painful tender mass on the left posterior scalp over the course of 6 months. On physical examination, the mass was very small; it was not palpable. At the beginning, the lesion seemed to cause pain only upon touching; but with progression, patient complained of pain even in resting state. Pain was intermittent and aggravated with cold air exposure. Previously at another hospital, he was treated using triamcinolone acetonide and hyaluronidase intralesional injection, but with no effect. Ultrasonography showed a 0.4×0.2×0.4 cm-sized hypoechoic nodule on aponeurosis with no compressibility and no vascularity (Fig. 1). However, the lesion was too small to be characterized on an ultrasonography. The patient did not want surgical removal.
After 10 weeks, the patient revisited our clinic with aggravated pain in the lesion. The pain was so severe that he was unable to sleep for the past three days. There was no apparent change on palpation. An emergency operation was performed under the impression of nerve origin tumor (Fig. 2). We received the patient's consent form about publishing all photographic materials. Macroscopically, the tumor was oval in shape and firm, with a size of 0.5×0.3×0.3 cm. Microscopically, the tumor was composed of spindle-shaped cells embedded in the dense collagenous stroma, with moderately increased cellularity and nuclear pleomorphism (Fig. 3). No mitosis or necrosis was observed. Immunohistochemically, spindle-shaped cells were positive for vimentin, but negative for α-SMA, CD34, and S100. The degree of proliferation measured with Ki-67 showed only a mild expression (Fig. 4). Based on the pathological findings, the tumor was finally diagnosed as a desmoplastic fibroblastoma. Pain disappeared after surgery, and there were no signs of recurrence during the three-month follow-up period.
DISCUSSION
Although there have been reports of the clinicopathological features of desmoplastic fibroblastoma since 1995, it may be an unfamiliar tumor to many dermatologists due to its rarity34. According to Miettinen and Fetsch5, desmoplastic fibroblastoma has been observed in the arms (24%), shoulders (19%), posterior area of the neck or upper back (14%), ankles and feet (14%), legs (14%), hands (8%), as well as the abdominal wall and hip (6%). To the best of our knowledge, this is the first report of desmoplastic fibroblastoma presented on the scalp, aside from some other unusual locations on the head, such as oral cavities, parotid gland, forehead, and orbital rims6789. Furthermore, our case is unique in that severe pain and tenderness were accompanied with the tumor, which is highly unusual. In most previous cases, patients displayed no subjective symptoms, including pain or tenderness. Additionally, with respect to size, our case was unusually smaller than the typical desmoplastic fibroblastoma observed previously to have a maximum diameter of approximately 4 cm15. Neurological symptoms have not been reported as a feature of desmoplastic fibroblastoma, despite frequent nerve entrapment of the tumor5. Only in one previous report, desmoplastic fibroblastoma on the right neck resulted in sensorimotor deficit of the right arm and shoulder3. In that case, however, the neurological symptom was likely due to the compression of the right upper cervical plexus and the right spinal accessory nerve by the tumor. In our case, the tumor was too small to invade or affect any adjacent nerves, and according to our microscopic findings, there was no evidence of nerve invasion.
Histologically, desmoplastic fibroblastoma is a hypocellular tumor with spindle to stellate-shaped fibroblasts in the dense fibroumyxoid stroma10. With respect to the immunohistochemistry of desmoplastic fibroblastoma, our results were consistent with previous reports: Positivity for vimentin, variable expressions of α-SMA, and negativity for CD34, desmin, and S10011.
Differential diagnosis for desmoplastic fibroblastoma includes fibromatosis, neurofibroma and low grade fibromyxoid sarcoma. Fibromatosis is more cellular and has more prominent vascular structures than desmoplastic fibroblastoma2. Neurofibroma may have similar fibromyxoid stroma but cells are strongly positive for S10012. A low grade fibromyxoid sarcoma is distinguishable from desmoplastic fibroblastoma by increased cellularity and characteristic swirling, whorled growth pattern13.
Conclusively, we reported a unique case of desmoplastic fibroblastoma on the scalp presenting with unusual tenderness and pain. Complete excision was performed, resulting in complete improvement of pain and tenderness.



 XML Download
XML Download