

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Prostate cancer ranks second among malignant cancers in men in the developed world (1). Localized prostate cancer can be treated with radical prostatectomy or radiotherapy, but 20–50% of patients suffer recurrence within 5 years after initial treatment (2345). Recurrent tumors can be treated with high-intensity focused ultrasound ablation, brachytherapy, cryotherapy or radical prostatectomy; in the absence of these treatments, metastasis can occur in 3 years (67). This highlights the importance of timely detection of recurrence. Unfortunately, the effectiveness of computed tomography and transrectal ultrasound in detecting recurrence is low (8), and the diagnostic accuracy of magnetic resonance imaging (MRI), primarily T2-weighted imaging (T2WI), can be compromised by changes resulting from radical prostatectomy or radiotherapy, including prostate shrinkage and loss of normal zonal anatomy.
Recent evidence suggests that the diagnostic accuracy of T2WI can be increased by incorporating data from functional MRI, including diffusion-weighted imaging (DWI)-MRI, dynamic contrast-enhanced (DCE)-MRI, and 1H-magnetic resonance spectroscopy (1H-MRS)-MRI (910). However, an optimal imaging strategy for diagnosing recurrent prostate cancer has not been defined.
A previous meta-analysis of a relatively small number of studies examined the accuracy of functional MRI and T2WI for detecting locally recurrent prostate cancer (11). However, that work did not include DWI-MRI, and a Z test was not performed to determine whether sensitivity and specificity differed significantly between the two types of MRI analysis. Therefore, we conducted a new meta-analysis with a larger number of studies, strict inclusion criteria, and rigorous methodology to determine whether adding functional MRI data to T2WI can improve diagnosis of locally recurrent prostate cancer.
MATERIALS AND METHODS
This meta-analysis was conducted according to the recommendations of the Cochrane Collaboration (12). The analysis results are reported according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses statement (13).
Literature Search
PubMed, Embase, the Cochrane Central Register of Controlled Trials, and the Cochrane Database of Systematic Reviews were comprehensively searched using the following search phrases: “(MRI OR magnetic resonance imaging OR MR) AND (prostate cancer OR prostatic) AND (sensitivity OR specificity OR false negative OR false positive OR diagnosis OR detection OR accuracy).” The search was designed to identify all full-length English language articles published between January 1, 1995 and December 31, 2016. The reference lists of all retrieved articles were reviewed to identify additional relevant articles.
Inclusion Criteria
Studies were included in this meta-analysis if 1) T2WI, DCE, DWI, and/or 1H-MRS-MRI were used to identify and characterize locally recurrent prostate cancer, 2) they used histopathology and/or follow-up clinical analysis and imaging at 6 months post-surgery as the reference standard, and 3) reported results in a 2 × 2 contingency table or in a way that such a table could be reconstructed. When data were presented in more than one article, the article with the larger sample size was chosen.
Data Extraction and Quality Assessment
Three reviewers assessed all retrieved articles independently and disagreements were resolved by consensus. The same reviewers as conducted the literature search also independently extracted relevant data from each study using a standardized data extraction form. To resolve disagreement among the reviewers, a fourth reviewer assessed all discrepant items, and the majority opinion was used in the analysis. Data on the following items were extracted from each study: author; year of publication; sample size; description of study population (age); study design (prospective, retrospective, or unknown); and numbers of true positives (TPs), false positives (FPs), false negatives (FNs), and true negatives (TNs) in the detection of locally recurrent prostate cancer, on a per-lesion and per-patient basis. When reported data were insufficient to construct a 2 × 2 table, we requested additional information from the authors.
We estimated the quality of included studies by using the Quality Assessment on Diagnostic Accuracy Studies-2 (QUADAS-2) quality assessment tool for studies of diagnostic accuracy (1415). Each item is assessed as “yes” (high quality), “no” (low quality), or “unclear” (inadequate information provided). The quality assessment was performed by two researchers independently using Review Manager 5.3, and disagreements were resolved by consensus.
Statistical Analysis
On the basis of the data extracted from individual studies, we constructed 2 × 2 contingency tables showing TP, FP, TN, and FN to calculate the pooled sensitivity, specificity, positive likelihood ratio, negative likelihood ratio, and diagnostic odds ratio (DOR) with corresponding 95% confidence intervals (CIs). These pooled data were fitted into a hierarchical summary receiver operating characteristic (HSROC) curve generated using hierarchical logistic regression (1617). We calculated the logarithm of the DOR for all included studies when exploring heterogeneity through sensitivity analyses.
Publication bias was assessed using a scatter plot in which the inverse of the square root of the effective sample size (ESS1/2) was plotted as a function of log DOR. A symmetric funnel shape for the plot suggests absence of publication bias. Quantitative testing for publication bias was conducted using regression of the log DOR against ESS1/2 and weighting according to the ESS. A p value < 0.1 indicated significant asymmetry (1819). All statistical tests were two-sided, and calculations were performed using Stata 13 (StataCorp LLC, College Station, TX, USA).
RESULTS
Search Results and Study Selection
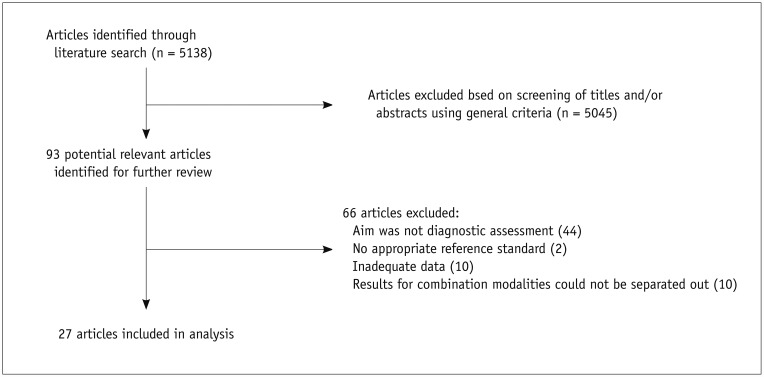
Database searches and manual searches of reference lists identified 5138 potentially relevant abstracts, of which all but 93 were eliminated after review of titles and abstracts. After reading the full texts of the 93 articles, we excluded 66 because 1) the aim was not to assess the diagnostic value of MRI for identification and characterization of locally recurrent prostate cancer (n = 44), 2) histopathology analysis and/or follow-up clinical analysis and imaging at 6 months post-surgery were not used as the reference standard (n = 2), 3) sufficient date were not reported for constructing 2 × 2 tables (n = 10), or 4) results were reported for combinations of imaging modalities but not for individual modalities (n = 10). Finally, 27 articles (202122232425262728293031323334353637383940414243444546) fulfilled all inclusion criteria and were selected for data extraction and data analysis (Fig. 1).
Study Characteristics
Study characteristics are shown in Supplementary Table 1 (in the online-only Data Supplement). Of the 27 studies, 15 were published after January 1, 2010 (212223242530343738394042434445). The number of patients per study ranged widely from 11 to 176, and the number of sectors ranged from 42 to 318. Results were analyzed on a per-patient basis in 20 studies (2223242526282930323334353637383940444546) and on a per-lesion basis in 10 studies (20212325262731414243). A pelvic phased-array coil was used in 13 studies, an endorectal coil in two studies, and a combination of the two in 12 studies. MRI was performed on a 1.5T device in 18 studies, on a 3T device in five studies, and on either a 1.5T or 3T device in four studies. Recurrent prostate cancer was confirmed by transrectal ultrasound-guided biopsy in 20 studies, and by a combination of biopsy, positron emission tomography, and clinical data in 7 studies.
Among 13 studies of patients who underwent radical prostatectomy and were analyzed on a per-patient basis, six (242832353638) reported the diagnostic accuracy of T2WI alone, two (3334) reported the diagnostic accuracy of the combination of 1H-MRS-MRI and T2WI, eight (2333363738394447) reported the diagnostic accuracy of the combination of DCE-MRI and T2WI, and three (222444) reported the diagnostic accuracy of the combination of DWI-MRI and T2WI.
Among 7 studies of patients who underwent radiotherapy and were analyzed on a per-patient basis, five (2326294046) reported the diagnostic accuracy of T2WI, three (232646) reported the diagnostic accuracy of the combination of DCE-MRI and T2WI, and three (232530) reported the diagnostic accuracy of the combination of DWI-MRI and T2WI. Among 11 studies of radiotherapy patients who were analyzed on a sextant biopsy basis, eight (2021232627314243) reported the diagnostic accuracy of T2WI, three (314041) reported the diagnostic accuracy of the combination of 1H-MRS-MRI and T2WI, five (2123262743) reported the diagnostic accuracy of DCE-MRI and T2WI, and six (202123254243) reported the diagnostic accuracy of DWI-MRI and T2WI.
Quality Assessment and Publication Bias
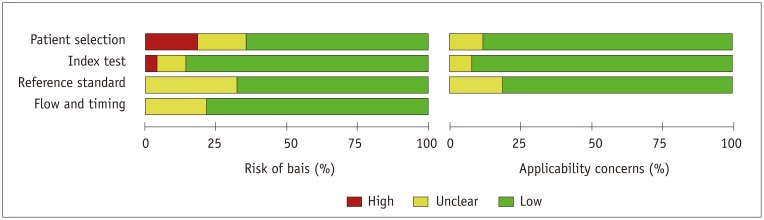
Study design was clearly stated as prospective in 9 studies (202326282930334447), whereas the study design was unclear in 7 studies (22273134353642). A graphical display of the evaluation of the risk of bias and concerns regarding the applicability of the selected studies is shown in Figure 2. Regarding risk of bias and patient selection domain, 7 studies received ratings of “unclear” for patient inclusion criteria (22273134353642). Regarding the domain index test, 22 studies adequately described the method of T2WI index testing as well as how it was performed and interpreted, whereas six (222731343536) were unclear in this regard. A total of 24 studies adequately described the method of functional MRI index testing and how it was performed and interpreted, whereas 4 studies were unclear (22273142). Regarding domain flow and timing, the interval between the index test and reference standard was unclear in 8 studies (2124253132373839). Three studies (252637) explicitly reported that pathologists were blinded to imaging results, whereas this was unclear in the other studies. Statistical testing to quantitate Deeks' funnel plot asymmetry obtained a p value < 0.1 for per-patient and per-sextant biopsy analyses after radiotherapy (Supplementary Figs. 1, 2 in the online-only Data Supplement), suggesting a significant risk of publication bias. However, no significant risk of publication bias was found in patient analysis after radical prostatectomy (Supplementary Fig. 3 in the online-only Data Supplement).
Data Analysis
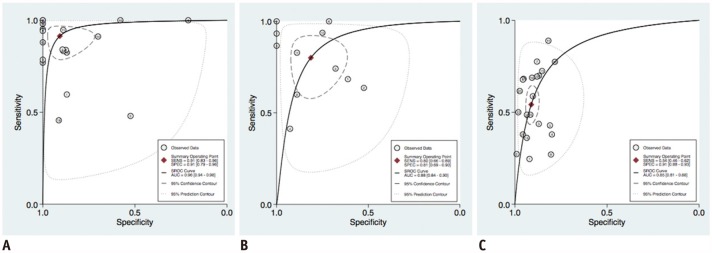
Supplementary Table 2 (in the online-only Data Supplement) shows TPs, FPs, FNs, TNs, sensitivity, specificity, and DOR for each study population. Meta-analysis of 13 studies of patients who underwent radical prostatectomy and were analyzed on a per-patient basis showed a pooled sensitivity of 91% (95% CI 83–96%) and specificity of 91% (95% CI 79–96%). The area under the HSROC curve (AUC) was 0.96 (95% CI 0.94–0.98) (Fig. 3A). The major source of heterogeneity was T2WI data from 1 study (36) (Supplementary Fig. 4 in the online-only Data Supplement); however, omitting this study and recalculating log DOR obtained a similar sensitivity of 93%, specificity of 91%, and HSROC area of 0.97 (Supplementary Table 3 in the online-only Data Supplement). These results suggest that no single study excessively influenced the meta-analysis.
Meta-analysis of 7 studies of patients who underwent radiotherapy and were analyzed on a per-patient basis showed a pooled sensitivity of 80% (95% CI 66–89%) and specificity of 81% (95% CI 69–90%), and the AUC was 0.88 (95% CI 0.84–0.90) (Fig. 3B). No obvious heterogeneity was identified by calculating log DOR over all included studies (p > 0.05). When we systematically removed one study at a time and recalculated the log DOR for the remaining studies, we obtained similar results as with all studies. These results also suggest that no single study excessively influenced the meta-analysis (Supplementary Table 3 in the online-only Data Supplement).
Meta-analysis of 11 studies of patients who underwent radiotherapy alone and were analyzed on a sextant biopsy basis showed a pooled sensitivity of 54% (95% CI 46–62%) and specificity of 91% (95% CI 88–93%), and the AUC was 0.85 (95% CI 0.80–0.88) (Fig. 3C). The major source of heterogeneity was four T2WI data sets (23262743) (Supplementary Fig. 5 in the online-only Data Supplement). Removing these studies and recalculating log DOR over the remaining studies obtained a sensitivity of 59%, specificity of 92%, and HSROC area of 0.88 (Supplementary Table 3 in the online-only Data Supplement), which were not significantly different from the original results (p > 0.05).
Subgroup Analysis
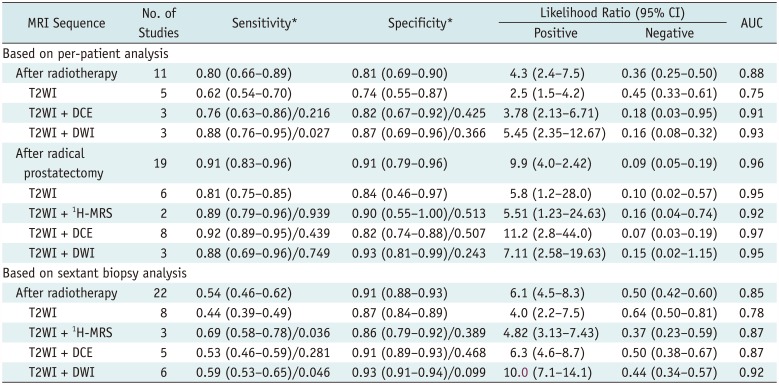
The results of subgroup analysis are shown in Table 1 and Supplementary Figs. 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16 (in the online-only Data Supplement). For patients who underwent radiotherapy, the combination of DWI-MRI and T2WI was associated with significantly higher sensitivity than T2WI alone, based on per-patient analysis (p = 0.027) as well as sextant biopsy analysis (p = 0.046). Among these patients, sensitivity was also significantly higher for the combination of 1H-MRS-MRI and T2WI than for T2WI alone (p = 0.036) based on sextant biopsy analysis.
DISCUSSION
T2-weighted imging alone is often used to detect locally recurrent prostate cancer because it can identify tumors based on their morphology at a reasonable cost, but its diagnostic accuracy is controversial. Our review included 13 studies involving patients treated with radical prostatectomy who were analyzed on a per-patient basis; sensitivity in these studies ranged from 48% to 100% and specificity ranged from 21% to 100%. Among these patients, T2WI alone was associated with a pooled sensitivity of 81%, specificity of 84%, and an AUC of 0.96. Adding functional MRI to T2WI did not significantly improve the accuracy of recurrent prostate cancer detection (p > 0.05). Given the cost of these additional sequences, the available evidence seems to indicate that adding functional MRI to T2WI may not provide benefit over T2WI for monitoring patients who undergo radical prostatectomy.
Our review also included 19 studies of patients who underwent radiotherapy, in which sensitivity of T2WI ranged from 25% to 78% and specificity ranged from 52% to 100%. T2WI performed poorly in detecting locally recurrent prostate cancer after radiotherapy, obtaining an AUC of only 0.75 based on per-patient analysis and 0.78 based on sextant biopsy analysis. This may reflect that, after external beam radiation therapy, the prostate gland shows diffuse, low T2 signal intensity and indistinct zonal anatomy (41). This highlights the importance of improving imaging methods to detect locally recurrent prostate cancer following radiotherapy.
Our meta-analyses showed that the AUC increased from 0.87 with T2WI alone to 0.91 with the combination of DCE-MRI and T2WI, based on per-patient or sextant biopsy analysis. Our results are consistent with several studies reporting that DCE-MRI, which has been in pre-clinical and clinical use for more than two decades, can detect locally recurrent prostate cancer. One study (26), for example, found that sensitivity was significantly higher with DCE-MRI (72%) than with T2WI (38%) on a sextant biopsy basis, although specificity was similar (85% vs. 80%). Another study (45) found that the sensitivity of DCE-MRI was higher than that of T2WI (93% vs. 86%), whereas specificity was similarly high in both cases (100%). The available evidence suggests that DCE-MRI is a promising tool for detecting locally recurrent prostate cancer.
Our meta-analysis showed that adding 1H-MRS-MRI to T2WI increased the AUC from 0.78 to 0.87 for patients who underwent radiotherapy and who were analyzed on a sextant biopsy basis. Adding 1H-MRS imaging to T2WI significantly increased sensitivity (p = 0.036) while maintaining specificity (p > 0.05). 1H-MRS-MRI aids in the detection of cancer by providing metabolic rather than anatomical information, which may help compensate for radiation-induced anatomic changes that reduce T2WI contrast after radiotherapy. 1H-MRS can metabolically differentiate between healthy prostatic glandular cells, which secrete large amounts of citrate, and malignant prostatic cells, which stop producing citrate (41). 1H-MRS can also detect the increased levels of choline in the cell membrane of many types of tumor cells (4148). Our meta-analysis supports the notion that 1H-MRS-MRI can strengthen the accuracy of T2WI for detecting locally recurrent prostate cancer following radiotherapy.
Nevertheless, the usefulness of 1H-MRS-MRI for this purpose is limited by the dependence of its sensitivity on the patient's Gleason score. Whereas the sensitivity of 1H-MRS-MRI for detecting lesions of any Gleason score is 56%, the sensitivity falls to 44% for tumors with a Gleason score of 6 and rises to 89% for tumors with a Gleason score of at least 8 (49). The usefulness of 1H-MRS-MRI is also limited because prostate cancer treatment often leads to undetectable levels of citrate and choline. In addition, several processes other than cancer can trigger an increase in choline and/or a decrease in citrate; these processes include androgen deprivation and inflammation (31), as well as radiation therapy (50).
Our meta-analyses showed that the addition of DWI-MRI to T2WI improved the AUC to 0.92 based on per-patient analysis and 0.93 based on sextant biopsy analysis, and this improvement was particularly evident in sensitivity. DWI-MRI yields quantitative and qualitative information about cell structure and membrane integrity based on contrast provided by proton diffusion within water (51). It can detect the reduced movement of water molecules that occurs when locally recurrent prostate cancer disrupts the normal glandular architecture and replaces it with fibrotic stroma and aggregated tumor cells.
This study had some limitations. The first crucial issue is that the studies addressing the accuracy of MRI used either salvage radical prostatectomy specimens or transrectal ultrasound-guided biopsies as the reference standard. Salvage radical prostatectomy introduces a selection bias, so this group might not be representative of all prostate cancer patients who experience biochemical failure. In fact, they are likely to over-represent more favorable radio-recurrent cancer among the population with biochemical failure after radiotherapy. Transrectal ultrasound-guided biopsies also introduce bias because the peripheral zone tends to be over-sampled, whereas anterior, transition, apical, and midline areas tend to be under-sampled.
Second, our meta-analysis was limited by heterogeneity in the experience of the radiologists, approaches to image interpretation, and methodological quality across the included studies. We attempted to minimize this heterogeneity by applying strict, narrow inclusion criteria, by assessing methodological quality using the QUADAS-2 tool, and by performing subgroup analysis based on the type of functional MRI. Nevertheless, heterogeneity may still have influenced our meta-analysis results. Third, the apparent lack of blinding and lack of clear prospective design of many studies in our review may imply a greater risk of bias in patient treatment and data analysis. Fourth, our analysis indicated a significant risk of publication bias in per-patient analysis of patients who underwent radiotherapy. Fifth, the relatively small number of studies reporting on each type of functional MRI meant that we could not correct for more than one study factor simultaneously, which may have rendered our results less robust.
In conclusion, T2WI-based detection of locally recurrent prostate cancer may be no more accurate with the addition of functional MRI in the case of patients who undergo radical prostatectomy, but it may become more sensitive with the addition of DCE-MRI, DWI-MRI, and 1H-MRS-MRI in the case of patients who undergo radiotherapy.
 XML Download
XML Download