

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Synovialcysts are commonly found in large joints, such as the shoulder, knee, and hip. Such lesions are often associated with labral or meniscal tears, and are known as paralabral or parameniscal cysts. In the hip, it has been suggested that labral tear may lead to increase of intra-articular pressure due to the loss of congruency between the femoral head and the acetabulum and the pressure can force synovial fluid through the area of labral tear and generate a cyst. It is well documented that the surgical treatments including open excision and arthroscopic decompression of parameniscal cysts in the knee and paralabral cysts in the shoulder have shown competent results. However, there is limited literature available regarding treatment options for paralabral cysts in the hip.
To the best of our knowledge, large acetabular paralabral cyst causing femoral vein compression is rare123). This report describes a case of acetabular paralabral cyst causing femoral vein compression that was treated with sono-guided cyst aspiration followed by arthroscopic labral debridement.
CASE REPORT
A 49-year-old household woman with no history of trauma and underlying disease presented diffuse edema of left lower extremity and mild left hip pain for 2 months. Her pain was insidious from its onset and was not preceded by any traumatic event. The patient said she recently tend to sit cross-legged and in a squatting position for a long duration during house work and was not involved in any sport activities. A visual analogue scale of pain was 3 points. She was able to walk but, the pain worsened when walking.
Physical examination of left hip showed no focal tenderness point and no limitation of range of motion. She had negative result on the Patrick's test and anterior impingement test.
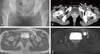
Radiographs of the left hip joint showed no dysplasia or bony abnormalities (Fig. 1). Because her chief complaint was diffuse edema of left lower extremity, computed tomography (CT) angiogram of lower extremity was performed for evaluation of vascular patency. CT angiogram showed a large multilobulated cyst compressing left common femoral vein (Fig. 1). Magnetic resonance imaging (MRI) showed a 60×31×96 mm sized paralabral cyst with increase of signal intensity suggesting labral tear (Fig. 1). The cystic lesion located anterior to acetabulum, medial and posterior to iliopsoas muscle (Fig. 2) and had connection with anterosuperior portion of acetabulum. The common femoral vein was flattened due to compression of the cyst and was displaced to anterior side.
One week before surgery, the cyst was aspirated two times under ultrasonography and yellowish fluid less than 1 mL came out. But until one week later, patient's symptom has not resolved and diffuse edema of left lower extremity has still remained. No medication was used for the patients. We suggest sono-guided aspiration one more time, but the patient doesn't want repeated aspiration anymore and she demands definitive procedure. So, arthroscopic surgery was performed under general anesthesia. Three standard portals (anterior, anterolateral, posterolateral) were used. Arthroscopic examination revealed anterosuperior labral tear with degeneration (Fig. 3). The torn labrum was seemed unrepairable so it has debrided using a shaver and thermal probe. Although we cannot find any cyst or cyst entry during arthroscope, yellowish fluid came out during debridement of labrum. We tried to look further to find cyst, but we couldn't. The patient was restricted to partial weight bearing using crutches and full weight bearing was permitted 4 weeks after surgery.
Three month postoperatively, the patient reported no left hip pain and improvement of lower extremity edema. CT angiogram at the 3-month follow up showed dissolution of cystic lesion (Fig. 4). At final follow-up one year postoperatively, the patient reported no problem.
DISCUSSION
In the hip, paralabral cysts are seen in 50% to 70% of patients with labral tears and in less than 5% of the general population3). Parameniscal cysts of the knee are seen in 4% to 6% of MRI scans and 90% of those had an associated meniscal tear. Tung et al.4) reported that paralabral cysts of the shoulder was seen in 2.3% of 2,211 MRI scans and an associated labral tear was found in 88%.
There is recent report about arthroscopic treatment for paralabral cysts of hip5). If left untreated, the cysts tend to enlarge over time. Although not all enlarged cyst require removal, but in patients with neurovascular compression due to cyst, surgical treatment may be effective at restoring function and preventing irreversible damage. Regarding surgical treatment, debridement of a paralabral cyst in the shoulder followed by labral repair has been shown to be an effective means that provides satisfactory improvement of symptoms. Hulet et al.6) reviewed a series of 105 lateral meniscal cysts treated surgically with cyst debridement and meniscal treatment. And they reported good or excellent results in 87% of cases at 5 year average follow-up. Similarly, in the hip, cyst debridement followed by labral treatment is generally accepted as the effective treatment, and it can be performed through either an open or arthroscopic approach. Sono-guided aspiration can be an option. Yukata et al.7) described use of ultrasound guided aspiration for a paralabral cyst compressing the obturator nerve. But the risk of recurrence increases with the use of only aspiration method treatment. With advances in arthroscopic techniques, arthroscopic surgery has become the preferred treatment to minimize the complication after surgical procedure8). A recent case report has shown excellent outcomes with arthroscopic treatment with decompression of the cyst and labral debridement, with improvement in Harris hip score, Western Ontario and McMaster Universities Osteoarthritis Index scores, and University of California, Los Angeles activity scores at 2 years' follow-up9).
Iliopsoas bursa is located lateral to the femoral vessels and nerve, and communicates with hip joint capsule 14.3% in adults. So, iliopsoas bursitis should be included in the differential diagnosis when patients typically present with anterior hip pain worsened by activity, especially hip extension. Although femoral nerve is in the same compartment of the iliopsoas bursa, femoral vein is in the different compartment. For this reason, compression of femoral vein by iliopsoas bursa is rarely occurred.
The current authors demonstrated a case of paralabral cyst in the hip that was treated with sono-guided cyst aspiration followed by arthroscopic labral debridement. It is not a generally recommended method to perform surgery without debridement or excision of the cyst. Before the surgery, the current authors considered two options for cyst decompression, which was ultrasonography guided aspiration or open excision. Of that, ultrasonography guided aspiration was chosen because open excision has a chance that develop into more serious complications and the patient desired a less invasive procedure. Kanauchi et al.10) described a case of an acetabular paralabral cyst causing femoral nerve palsy that was treated with cyst aspiration followed by arthroscopic labral repair and the results was satisfactory at least 18 months follow-up. Lee et al.5) described 3 cases of paralabral cyst causing entrapment neuropathy of the sciatic nerve treated arthroscopically. None of the patients had experienced recurrence of the cyst.
After the surgery, the current patient experienced a marked improvement in swelling and pain over the course of 3 months and repeat CT angiogram showed complete dissolution of the cystic lesion. The results remained satisfactory at least one year after surgery, although this is not a well-established treatment for acetabular paralabral cyst with labral tear.



 XML Download
XML Download