

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Soft-tissue calcification is a broad category of lesions that are frequently found by radiologists in daily practice. Using a simple algorithm based on distribution patterns, combined with detailed clinical information, such as history and laboratory testing, soft-tissue calcifications can be systematically evaluated. Calcinosis is a condition characterized by deposition of calcium in the skin, subcutaneous tissue, muscles, or visceral organs. This classification algorithm begins with the distribution pattern of the calcific deposits (Fig. 1) into one of two forms: calcinosis universalis or calcinosis circumscripta.
Calcinosis Universalis
Calcinosis universalis, also termed “dermal calcinosis” or “diffuse interstitial calcinosis,” is defined as diffuse deposition of calcium in the skin, subcutaneous cellular tissue, tendons, or muscles (1). The exact pathogenesis of calcinosis deposition remains unknown; however, it may be an intracellular accumulation of calcium secondary to an altered cellular membrane due to trauma or inflammation (2). Calcinosis universalis is a recognized presentation of connective tissue diseases, especially in juvenile dermatomyositis and polymyositis (3). Juvenile dermatomyositis accounts for up to 40% of these lesions; they are less common in adult-onset dermatomyositis, which accounts for 10% (24). Radiographically, they feature extensive sheet-like distributions of calcification (Fig. 2) (3).
Calcinosis Circumscripta
Calcinosis circumscripta manifests as localized or isolated calcification. According to serum levels of calcium and phosphate, these lesions can be further categorized into dystrophic, iatrogenic, metastatic, and idiopathic subtypes (Fig. 1). Dystrophic calcification is defined as calcification in altered necrotic tissue resulting from an underlying inflammatory process. It occurs in patients whose serum calcium and phosphorus levels are normal (5). Iatrogenic calcification results from a previous procedure or treatment such as repeated injections.
When soft-tissue calcification occurs with an elevated serum calcium-phosphorus ion product, it is known as metastatic calcification. In these cases, amorphous calcium phosphate and calcium hydroxyapatite crystals are deposited in multiple locations including the visceral organs (5). Idiopathic calcification is associated with a normal serum calcium level but elevated phosphate levels (6). Primary tumoral calcinosis is a hereditary metabolic dysfunction of phosphate regulation associated with massive periarticular calcinosis (3).
Dystrophic Calcification
Depending on the involved locations, dystrophic calcification can be grouped into the following causes: vascular-related (chronic venous insufficiency, Mönckeberg's arteriosclerosis, phleboliths and venous malformation); joint-related (calcium pyrophosphate deposition disease, tuberculous trochanteric bursitis); soft-tissue related (synovial sarcoma, myositis ossificans [MO], parasitic infection, connective tissue disease); and tendon/ligamentrelated (degenerative calcification, calcific tendinitis, and Pellegrini-Stieda lesion/syndrome) (Fig. 1).
Vascular Disease-Related Calcifications
Chronic Venous Insufficiency
Chronic venous insufficiency manifests as variable cutaneous findings including varicose veins, edema, hyperpigmentation, ulcerations and, occasionally, subcutaneous calcification. Two patterns of calcification are encountered on plain radiographs: punctate and trabecular/reticular types (Fig. 3) (7). The incidence of calcification correlates with disease duration and severity. Patients with longer disease duration present primarily with the trabecular type (7). Besides, the presence of these calcification causes poor wound healing. In addition, wavy and irregular periosteal reactions (Fig. 4) secondary to increased mean interstitial fluid pressure is occasionally found to exert pressure on the periosteum (8).
Mönckeberg's Arteriosclerosis
Two forms of arterial calcifications due to aging are recognized on radiography: those of the arterial intima (atherosclerosis); and those of the tunica media (Mönckeberg's arteriosclerosis) (9). Mönckeberg's arteriosclerosis refers to medial calcification deposits in the medium and small muscular arteries of the lower limbs and do not cause luminal narrowing. Currently, the exact etiology of this type of atherosclerosis remains unclear; they are primarily incidental findings that appear as a “railroad track” pattern (Fig. 5) (10).
Phleboliths
Phleboliths refer to calcifications within venous structures. They are usually characterized by spherical or round nodular shapes (Fig. 6).
Venous Malformations
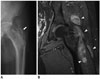
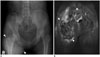
Vascular malformations are categorized as low-flow malformations (venous, lymphatic, capillary, capillary-venous, and capillary-lymphatic-venous) or high-flow malformations (arteriovenous malformations and arteriovenous fistulas) (11). They are the most common peripheral vascular malformations, and occur in the head and neck (40%), trunk (20%), and extremities (40%) (1112). They are frequently incorrectly referred to as “cavernous hemangiomas.” On magnetic resonance (MR) images, they usually present as septated or tubular lesions with hypointensity on T1-weighted images and increased signal intensity on T2-weighted images (Fig. 7). Heterogeneous signal intensity on T1-weighted images from hemorrhage or the presence of protein content is not uncommon (11). Marked diffuse enhancement of the slow-flowing venous channels on delayed postcontrast T1-weighted images is characteristic of venous malformation (11). Another helpful diagnostic clue is the presence of phleboliths (Figs. 7, 8) (1113).
Calcifications in Joint-Related Diseases
Calcium Pyrophosphate Dehydrate Deposition Disease
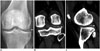
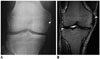
Calcium pyrophosphate dihydrate crystal deposition (CPPD) disease is defined as the deposition of CPPD crystals in hyaline cartilage, fibrocartilage, and other soft tissues inducing acute, subacute, or chronic inflammation (14). The knee joint accounts for the most (50–88%) cases, followed by the wrist (20%), and other areas including the ankle, hip, pubic symphysis, shoulder, and transverse ligaments of the spine (15). In the knee joint, disproportionate patellofemoral degenerative change is characteristic, and chondrocalcinosis involving the fibrocartilage menisci (Fig. 9) and hyaline cartilage is common (1416). In the wrist joint, calcification of the lunotriquetral ligament or the triangular fibrocartilage, associated with a narrowed radiocarpal joint space, is typically demonstrated. In addition, scapholunate advanced collapse is the most common form of wrist arthritis in patients with CPPD arthropathy (14). Additionally, narrowing of the metacarpophalangeal joints, sparing the interphalangeal joints, has been described.
Tuberculous Trochanteric Bursitis
Extrapulmonary manifestations occur in approximately 20% of patients with tuberculous infection (17), and 1% to 3% of those with musculoskeletal system attributes. The most common osseous presentation is tuberculous spondylitis (18). The least commonly involved area is the extraspinal region (19), whereas peripheral arthritis accounts for 60% of cases, followed by osteomyelitis (38%), and tenosynovitis and bursitis (2%) (18). Tuberculous trochanteric bursitis can occur at any location via hematogenous spread; however, it more commonly involves the trochanteric (Fig. 10) and olecranon bursae (20). In the literature, the trochanteric bursae of the hip has the greatest prevalence (2021). Concomitant infection of both affected bursae and adjacent structures, such as bone and tendon, is not unusual. Isolated tuberculous trochanteric bursitis is associated with soft tissue swelling or minute flecks of calcification within the bursae in the early stages, followed by bone destruction (22).
Calcifications in Soft-Tissue-Related Diseases
Synovial Sarcoma
Synovial sarcoma accounts for 2.5% to 10.5% of all primary malignant soft-tissue neoplasms, the majority affecting the extremities (80–95%), especially in the popliteal fossa (23). It is reportedly the most common malignancy of the soft tissues of the foot and ankle in adolescents and young adults (23). Lesions are usually found adjacent to a joint. Histologically, synovial sarcoma is a malignant mesenchymal neoplasm composed of epithelial and spindle cell components (323), and does not originate from the synovium. It is categorized into three subtypes: biphasic, monophasic, and poorly differentiated (23). Synovial sarcoma commonly presents as a multilobulated lesion with cystic change, necrosis, and hemorrhage. Areas of hyalinization within the spindle cell components can form punctate calcifications in as many as 30% of the cases (323). Radiographically, synovial sarcoma manifests as a juxta-articular soft-tissue mass with eccentric calcification (Fig. 11). Nonaggressive bone erosion, osteoporosis, and periosteal reaction have been illustrated, and these can easily be initially misdiagnosed as benign entities (3). On T1-weighted MR images, synovial sarcoma presents as an infiltrative, multilobulated soft-tissue mass with signal iso-intensity or mild hyperintensity compared with muscle. On T2-weighted MR images, a triple sign is apparent because of the intermixture of solid cellular elements (intermediate signal intensity), hemorrhage or necrosis (high signal intensity), and calcifications (low signal intensity) (2324). Marked heterogeneous enhancement after intravenous contrast administration is apparent in synovial sarcomas (Fig. 11).
Myositis Ossificans
Myositis ossificans is defined as a solitary calcified soft-tissue mass with heterotopic bone and cartilage formation, typically presenting in skeletal muscle (325). Large muscles of the extremities account for 80% of cases (26). The mechanism of MO formation remains unclear, and the term “myositis” is a misnomer because there is no inflammatory process. MO usually results from injury, cerebrospinal disorders, or burns (3). These ossifying lesions are commonly surrounded by atrophic skeletal muscles with a distinct zone appearance. The lesion begins with an immature central nonossified cellular focus to the peripheral rim of mature lamellar bone (25). Radiographically, a faint calcification becomes apparent within 2 to 6 weeks of the onset of symptoms and progresses into a distinctive mass lesion with peripheral mature ossification after 6 to 8 weeks (Fig. 12).
Parasitic Infection (Cysticercosis)
Cysticercosis is a common parasitic infection caused by the dissemination of Taenia solium from the intestine to the systemic organs by drinking contaminated water or ingesting uncooked pork. The most commonly affected organs are subcutaneous tissues, skeletal muscles, lungs, brain, eyes, liver and, occasionally, the heart (27). Typical radiographic features are rice-grain calcifications parallel to the long axis of the soft tissue (Fig. 13). These calcifications are dead larval cysts (cysticerci) (28). In addition, intramuscular abscesses, subcutaneous nodules, or pseudohypertrophy of the muscles have been described (29).
Connective Tissue Disease (Scleroderma)
Calcinosis circumscripta manifests as dense, white dermal plaques or subcutaneous nodules usually identified near a joint (Fig. 14) (3). These calcifications are commonly associated with connective tissue diseases including the early stages of polymyositis, dermatomyositis, systemic lupus erythematosus, progressive systemic sclerosis, scleroderma and calcinosis, Raynaud phenomenon, esophageal dysmotility, sclerodactyly, and telangiectasia (CREST) syndrome (3).
Calcifications in Tendon/Ligament-Related Diseases
Degenerative Calcification
The Achilles tendon is composed of the tendons of the soleus and gastrocnemius muscles, and inserts at the posterior calcaneal tuberosity. It is enclosed within a paratendon rather than a synovial sheath (30). Ossification of the Achilles tendon is an uncommon complication of Achilles tendon injury and is usually the result of previous trauma (tendon rupture or repeated micro-trauma) or surgery (31). Based on the anatomical ossification sites on radiographs, the disorder is classified into 3 types. In type 1, ossification is located at the tendinous insertion. In type 2, it is located 1–3 cm from the tendon insertion (Fig. 15). Finally, in type 3, lesions are localized up to 12 cm from tendon insertion. Lesions can further be grouped into those with partial ossification and those with complete ossification of the tendon (3132).
Calcific Tendinitis
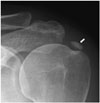
Calcific tendinitis is defined as deposition of calcium hydroxyapatite crystals within the tendons. It most commonly occurs in individuals between 30 and 60 years of age, and women are slightly predominant among those diagnosed (33). It primarily affects the shoulder and hip joints. In the shoulder joint, the supraspinatus tendon (Fig. 16) is involved in 80% of cases, followed by the infraspinatus, which accounts for 15%, and the subscapularis tendons, which account for 5% (34). Radiographically, calcification, which is restricted to the tendon without evidence of degenerative joint disease, is diagnostic (35). During the calcification phase, the deposit appears to be homogeneously dense and well-defined, whereas in the resorptive phase, it can manifest as fluffy and ill-defined (3335).
Pellegrini-Stieda Lesion/Syndrome
Pellegrini-Stieda syndrome is characterized by ossification of the femoral attachment of the medial collateral ligament, and develops adjacent to the medial femoral epicondyle 3 or 4 weeks following injury (36). Clinical presentations include medial swelling of the knee with pain; however, sometimes the patient is asymptomatic. On radiographs, a linear vertical ossification is depicted adjacent to medial femoral condyle (Fig. 17). However, this ossification can also involve the adductor magnus tendon.
Iatrogenic Calcifications (Injection Granulomas)
Injection granulomas result from repeated injections into the subcutaneous fat (37). They are usually found in the upper outer quadrant of the gluteal regions but can occur at any injection site. Tissue reactions depend on the site, number of injections, and the composition of the injected material (38). On radiographs, injection granulomas are characterized by well-circumscribed calcified nodules (Fig. 18) (39).
Metastatic Calcifications
Causes of metastatic calcifications include chronic renal failure, hyperparathyroidism, pseudohypoparathyroidism, sarcoidosis, and tophaceous gout.
Chronic Renal Failure
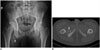
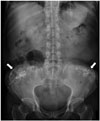
Biochemical disturbances resulting from chronic renal failure can give rise to vascular and soft-tissue metastatic calcifications (40). Clinically, these patients exhibit hyperparathyroidism secondary to chronic renal failure and hemodialysis (Figs. 19, 20, 21). These calcified lesions, however, cannot be distinguished from primary tumoral calcinosis based on imaging findings or histology (341).
Primary Hyperparathyroidism
When parathyroid hormone is autonomously secreted, primary hyperparathyroidism can result in bone resorption when this secretion is not suppressed by elevated serum levels of calcium (42). It is most commonly encountered in individuals > 50 years of age, and in women more than men, by a factor of three- to fourthfold (43). In approximately 90% of cases, they are caused by parathyroid adenomas and, in approximately 10%, they result from multi-gland hyperplasia. In extremely rare cases, primary hyperparathyroidism results from parathyroid carcinomas (44). Skeletal manifestations of hyperparathyroidism include subperiosteal bone resorption, a “salt-and-pepper” appearance of skull demineralization, distal clavicle tapering, and brown tumors (43). Subperiosteal bone resorption usually begins at the radial aspects of the middle phalanges of the middle and index fingers, and at the distal phalangeal tufts as acro-osteolysis (Fig. 22) (42).
Pseudohypoparathyroidism
Pseudohypoparathyroidism is a heterogeneous group of disorders characterized by end-organ resistance to parathyroid hormone. It is subclassified into types Ia, Ib, Ic, and II (45). Albright's hereditary osteodystrophy is a clinical entity described together with pseudohypoparathyroidism, presenting as brachydactyly, rounded face, short stature, central obesity, subcutaneous ossifications, and varying degrees of intellectual disability (46). Brachydactyly typically manifests as a shortening of the third, fourth, and fifth metacarpals, and the first distal phalanx (Fig. 23).
Sarcoidosis
Sarcoidosis is a systemic granulomatous disease characterized by noncaseating granulomas in soft tissues without definite cause. The disease most commonly affects the lungs, lymph nodes, skin, and eyes (47). However, it can also involve the musculoskeletal system, in which 1% to 13% (estimated average, 5%) of sarcoidosis cases have been reported (48). Approximately 90% of the osseous lesions found in sarcoidosis are small bone lesions, especially in the distal and the middle phalanges of the second and third digits (49). Classically, they present with a “lacy” lytic appearance (47), or with extensive bone erosion and pathological fractures, sparing the articular surfaces (50). In addition, the infiltrated soft tissues will also demonstrate “sausage finger” or “radish” deformities (49). A single bone can exhibit up to 3 types of small bone lesions (49): type 1, large bone geodes or bullous lesions; type 2, multiple well demarcated, rounded, and occasionally confluent geodes located in the heads of the phalanges; and type 3, a “lace-like” pattern with thickened bone sheets and a thin cortex (Fig. 24).
Tophaceous Gout
Gouty arthritis is caused by deposition of monosodium urate monohydrate crystals and subsequently forms periarticular tophus masses that can induce both acute and chronic inflammation (3). Adjacent soft tissue swelling due to gouty tophus deposition is virtually diagnostic on radiographs. Gouty arthritis typically exhibits juxta-articular, marginal erosion with an overhanging edge and extends perpendicularly from underlying bone. The first metatarsophalangeal joint of the foot is the most commonly affected (Fig. 25).


















 XML Download
XML Download