

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Radiofrequency ablation (RFA) is currently the most widely used technique for curative treatment of early-stage hepatocellular carcinoma (HCC) (1). The most frequently utilized RFA technique is the monopolar technique using intra-tumor electrode placement (2). However, a major limitation of RFA using the conventional monopolar direct tumor puncture (DTP) technique is the relatively high local tumor progression (LTP) rate, which has been reported to range between 25–53%, owing to the limited volume of tumor necrosis that can be achieved (345). Therefore, overlapping ablation techniques are now more frequently used to create an adequate safety margin around the target tumor (67). However, the conventional tumor penetration technique also poses additional risks of unwanted tumor seeding, which increase when using multiple placements of electrodes within the target tumor, especially in subcapsular locations. Thus, the achievement of a large peritumoral ablation zone while decreasing the risk of procedure-related tumor cell seeding is desirable for improving the therapeutic efficacy of RFA for liver malignancies.
Recently, a no-touch technique using multi-bipolar techniques has been suggested to ensure the maximum ablative area by creating high-density electrical fields between several pairs of independent electrodes (2589). Although there have been sporadic studies that hinted at promising results for the no-touch RFA (NtRFA) technique, only one recent retrospective study (2) directly compared NtRFA with the conventional DTP technique. In addition, a critical issue that has not yet been explored is whether NtRFA can lead to less peritoneal seeding and decreased tumorigenic factor release than conventional monopolar tumor puncture RFA. Even though RFA has proven to be an effective adjunct in treating hepatic tumors as a bridge to liver transplantation (1011) and adverse events are rare, a notable negative outcome is dissemination and implantation of viable tumor cells into the route of applicator entry, i.e., tract seeding (12). If NtRFA in bipolar mode could be shown to reduce tract seeding, it would become an attractive alternative to conventional monopolar RFA using DTP, particularly for peripherally located liver malignancies. As another factor, RFA has recently been recognized to induce cytokines such as interleukin-6 (IL-6), hepatocyte growth factor (HGF) and vascular endothelial growth factor (VEGF), which promote liver regeneration but may also facilitate unwanted tumor recurrence or distant metastasis (1314151617). These cytokines are termed tumorigenic factors and may be produced in the residual incompletely treated tumor at the ablative margin and in the healthy liver surrounding the targeted tumor (1617). However, until now there has been no study clarifying whether contact with the tumor during the procedure influences the release of tumorigenic factors.
Thus, in this proof of concept study, we attempted to compare the NtRFA technique in bipolar mode with conventional DTP-RFA in terms of local tumor control (LTC), peritoneal seeding, and the release of tumorigenic factors, using a rabbit VX2 subcapsular hepatic tumor model.
MATERIALS AND METHODS
This animal study was approved by the Institutional Animal Care and Use Committee at our hospital, Seoul National University Hospital (IACUC No. 16-0109-S1A0). The experimental design of this study is summarized in a flowchart in Figure 1.
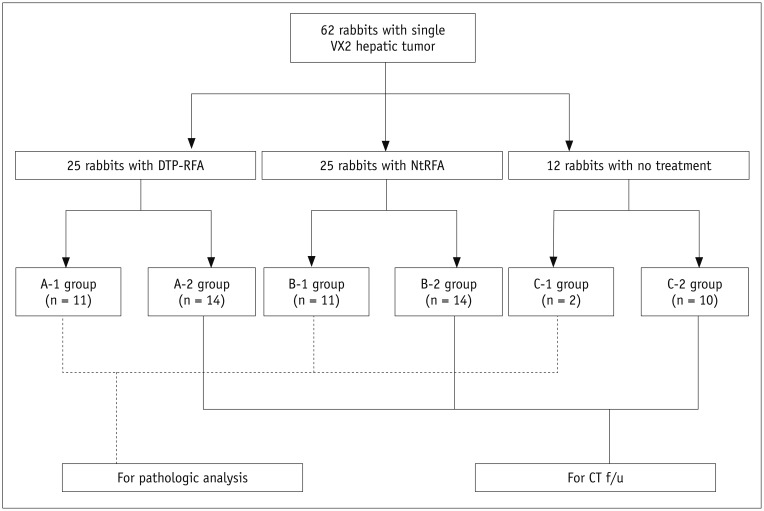
Fig. 1
Study protocol.
In total, 62 New Zealand white rabbits with VX2 tumors confirmed by CT on day 9 (range, 7–12) were randomized into three groups (DTP-RFA group, NtRFA group, and control group). Each group was further divided into two subgroups for pathologic analysis (A-1, B-1, C-1) and for 6 weeks of CT follow-up (A-2, B-2, C-2). CT = computed tomography, DTP-RFA = direct tumor puncture radiofrequency ablation, NtRFA = no-touch RFA
![]()
Animal Care and VX2 Liver Implantation
A total of 62 adult New Zealand white rabbits weighing 2.5–3 kg were used. The VX2 tumor used in this study is a virus-induced anaplastic squamous cell carcinoma characterized by hypervascularity with rapid growth (1819). The rabbit VX2 tumor model has been employed in numerous RFA-based studies for the treatment of HCC (20212223). After preparation of 4 mm3 tumor chips from donor rabbits, midline subxiphoid laparotomy was performed in all 62 rabbits for liver tumor implantation into the subcapsular parenchyma in the left medial lobe of the liver. All rabbits were given appropriate postoperative care, including analgesics and antibiotics.
In Vivo RFA Procedure
Dual RFA electrodes with a 1-cm active tip (STARmed, Goyang, Korea) were placed percutaneously under ultrasonography (US) guidance. For the DTP-RFA group (n = 25), one of two electrodes directly penetrated the tumor, while the other electrode was inserted at the periphery of the tumor. For the NtRFA group (n = 25), both electrodes were inserted at the periphery of the tumor, but not penetrating it. The only difference between the two groups regarding the RFA procedure was whether any of the electrodes penetrated the tumor. After the RFA procedure, cauterization of the electrode tracks was performed in both groups. An illustration of the in vivo RFA procedure used in this study is shown in Figure 2. For the control group (n = 12), observation was performed without any treatment after tumor implantation.
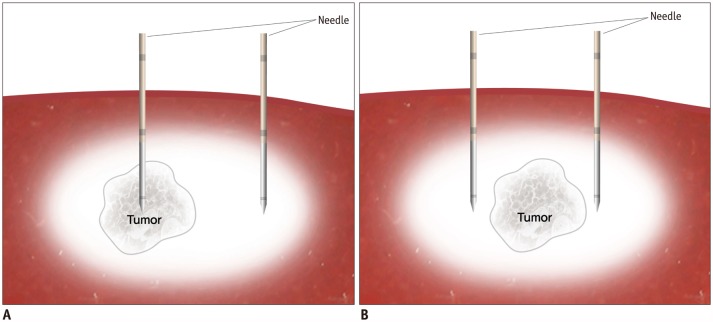
Fig. 2
Illustration of DTP-RFA and NtRFA.
A. DTP-RFA technique. One of dual electrodes is inserted directly into tumor, penetrating tumor capsule. This technique initiates ablation within tumor. B. NtRFA technique. Dual bipolar needles are inserted into periphery of tumor, not penetrating tumor capsule. This technique induces ablation starting from healthy tissues surrounding tumor, then extending centripetally into tumor.
![]()
Radiological Study
All computed tomography (CT) examinations were performed on a multi-detector CT scanner (Discovery CT 750 HD; GE Healthcare, Pewaukee, WI, USA) with 2 mL/kg of nonionic contrast medium (Ultravist 370, Bayer, Wayne, NJ, USA) injected through an auricular vein in the supine position. CT scans included pre, arterial (15 seconds) and portal (30 seconds) phases after a contrast injection rate of 1 mL/sec with a 1 mm slice thickness from the head to upper thigh, with the following CT parameters: 150 mA, 140 kVp, 1.0 pitch, and 214 × 214 mm2 field of view. All 62 rabbits with VX2 tumor implantations underwent CT scans prior to RFA (median, nine days after implantation [range, 7–12 days]). In the subgroups for CT follow-up (14 rabbits each from the DTP-RFA and NtRFA groups, and ten rabbits from the control group), CT scans were performed every week until the 6th week after RFA. Semiautomated measurements of the ablation volume for each animal were done in an axial, coronal, or sagittal view for follow-up CT scans acquired 3 days after RFA using the three-dimensional functionality of a picture archiving and communication system (PACS; INFINITT Healthcare Co., Ltd., Seoul, Korea). The ablation area was distinguished as a nonenhancing area of low attenuation in the liver on CT (24). LTP was defined by the appearance of nodular, mass-like, or thick irregular tissue with enhancement adjacent to the previously RFA-treated site (24). Peritoneal and skin seeding was determined as the appearance of enhancing nodular or thick irregular-shaped lesions with interval increments attached to the peritoneum or subcutaneous layer and skin (25). Euthanasia and autopsy were also performed in all rabbits with CT follow-up, to correlate the CT data and pathology after completion of the 6-week follow-up.
Pathologic Analysis
Euthanasia was performed for pathologic examination three days after RFA. The liver was then harvested, and multiple slices of 1 cm thickness were cut perpendicularly to the RFA needle insertion direction. The sliced tissues were embedded in an optimal cutting temperature compound (Tissue Tek; Sakura Finetek, Tokyo, Japan), quenched in isopentane, and frozen in liquid nitrogen prior to storage at −80℃ for nicotinamide adenine dinucleotide (NADH) diaphorase activity evaluation, which reflects the viability of the tumor (26). The remnant specimen was fixed in 10% neutral buffered formalin, embedded in paraffin, and sliced into 5-µm sections for hematoxylin & eosin (H&E) staining for histologic structural evaluation. Pathologic analyses were performed on the main tumor nodule and peri-nodular satellite nodules. Complete local necrosis was defined as complete involvement of the main tumor and all peri-nodular satellite nodules within the ablative zone on H&E staining with no NADH staining (26). To assess the tumorigenic effect, immunohistochemistry was performed to quantify activated Ki-67 positive hepatocytes using anti-Ki-67 (Ab155580; Abcam, Cambridge, MA, USA) in the ablated lobe with high-power (× 40) microscopy (14).
Local tumor control was defined as either complete local necrosis on histopathologic examination or absence of LTP on follow-up CT and autopsy.
Biochemical Analysis of the Tumorigenic Factor
Serum levels of IL-6, HGF and VEGF before and 24, 48, and 72 hours after RFA were measured via enzyme-linked immunosorbent assay (ELISA) using a rabbit kit (Elabscience Biotechnology Co., Wuhan, China). Untreated rabbits served as controls. A total of 14 rabbits (6 rabbits each for the NtRFA and DTP-RFA groups, and two rabbits from the control group) were used for the analysis. ELISA were performed according to the manufacturer's instructions.
Statistical Analysis
Data are reported as mean ± standard deviation (SD), median (range) or number (percentage, %) as appropriate. Comparisons between DTP-RFA and NtRFA were performed using Fisher's exact test or the chi-squared test for categorical variables and the unpaired Student's t test or Mann-Whitney U test for continuous variables. For continuous variable comparison among the three groups (DTP-RFA, NtRFA, and control), analysis of variance (ANOVA) was performed. All statistical analyses were performed using commercially available statistical software (SPSS for Windows, version 21.0; IBM Corp., Armonk, NY, USA). P values of < 0.05 were considered to indicate a statistically significant difference.
RESULTS
VX2 Carcinoma and in vivo RFA Procedure
The intrahepatic VX2 tumors were grown for a mean of 9.7 days and 10.2 days for the DTP-RFA and NtRFA groups, respectively, reaching mean sizes of 7.9 mm and 8.3 mm in the axial longest diameter on pre-RFA CT. All 62 rabbits were confirmed to have successful VX2 tumor implantation in the left medial lobe subscapular area, with no iatrogenic tumor seeding on pre-RFA CT.
We initially conducted ex vivo testing for RFA optimization, adapting the results of previous studies (2728) (Supplementary Table 1 in the online-only Data Supplement), and applied the results of the ex vivo test to the in vivo RFA procedure using the following specifications: power, 50 watts; distance between the two RFA needles, 10–13 mm; energy, 0.51 kcal (SD, ± 0.06) in DTP-RFA, 0.50 Kcal (SD, ± 0.12) in NtRFA ; ablation time, 297.6 seconds (SD, ± 75.8) in DTP-RFA, 327.4 seconds (SD, ± 109.6) in NtRFA. The number of punctures per procedure differed between the two groups, with the NtRFA group requiring more punctures (DTP-RFA: 2 [median] [range, 2–3]; NtRFA: 3 [2–5], p < 0.001). Table 1 summarizes the tumor characteristics and in vivo RFA specifications for the DTP-RFA and NtRFA groups, which showed no significant differences.
Table 1
Tumor Characteristics and in Vivo RFA Specifications
![]()
LTC
Table 2 summarizes the results for LTC in DTP-RFA and NtRFA, based on both pathologic analysis and 6-week post-RFA CT follow-up. There was a tendency toward better results with NtRFA than with DTP-RFA (DTP-RFA 56% [14/25] vs. NtRFA 80% [20/25], p = 0.069). Regarding complete local necrosis (including the main tumor and satellite nodules) on pathologic assessment, DTP-RFA achieved it in 54.5% (6 out of 11) of rabbits, whereas NtRFA achieved it in 90.9% (10 out of 11) of rabbits (p = 0.148). Furthermore, in three of the five rabbits in the DTP-RFA group with viable satellite nodules, the viable satellite nodules were located more than 5 mm from the main tumor (Fig. 3B, Supplementary Table 2, Supplementary Fig. 1 in the online-only Data Supplement) whereas all of the satellite nodules in the NtRFA (n = 1) and control group (n = 2) were within 2 mm of the main tumor. In addition, intravascular tumor emboli were noted in one of the rabbits in the DTP-RFA group with a satellite nodule (Supplementary Fig. 1 in the online-only Data Supplement). On CT follow-up and autopsy, the DTP-RFA group showed LTP in 42.8% (6 out of 14) of rabbits, while the NtRFA group showed LTP in 28.6% (4 out of 14) of rabbits (p = 0.694). Representative histopathologic figures of DTP-RFA, NtRFA and control are shown in Figure 3.
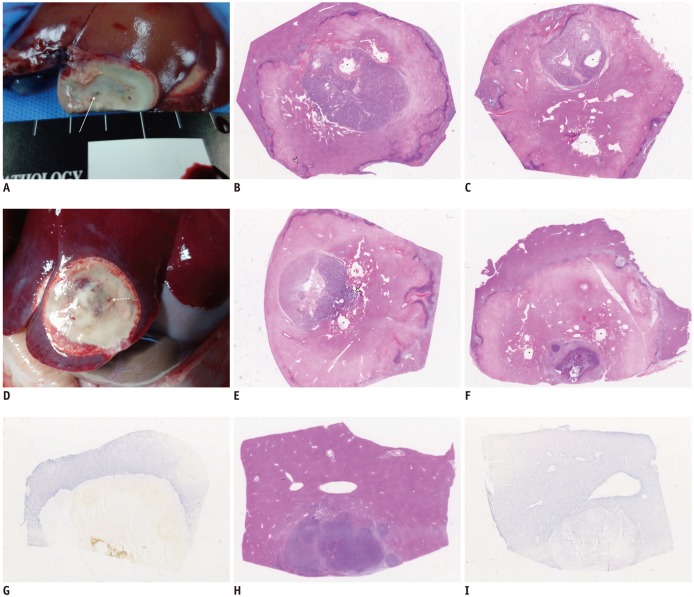
Fig. 3
Histopathology in DTP-RFA, NtRFA, and control.
A–C. DTP-RFA technique. A. Gross anatomic picture showing one of bipolar needles (arrow) penetrating tumor. B. H&E staining of ablation zone reveals needle insertion site (asterisks) in main mass within ablation zone. Note that incomplete ablation was performed for satellite tumor nodule (arrowhead). Satellite nodule is located 6 mm from main tumor. C. Another H&E stain of ablation zone reveals needle insertion site (asterisks) within tumor. Note that lateral border of main tumor abutted ablation margin. D–G. NtRFA. D. Gross anatomic picture showing dual bipolar needles (dotted arrows) penetrating periphery of tumor. E, F. H&E staining of ablation zone in two different rabbits reveals needle insertion site (asterisks) with both main tumor and satellite nodules (arrowhead) completely ablated. G. NADH staining of ablation zone. Contrary to normal viable cells with NADH staining outside of ablation zone, there is no viability within ablation zone. H, I. Control group. H. H&E staining reveals main tumor with multinodular satellite tumors. Note that all satellite nodules are located within 2 mm from main tumor (I) NADH staining shows both viable hepatocytes and main tumor. H&E = hematoxylin & eosin, NADH = nicotinamide adenine dinucleotide
![]()
Table 2
LTC between DTP-RFA and NtRFA
Data are presented as number with percentage in parentheses. *Defined as total involvement of both main tumor and all peri-nodular satellite nodules within ablative zone on hematoxylin & eosin staining with no nicotinamide adenine dinucleotide staining, †Determined by either achievement of complete local necrosis on histopathologic examination or absence of LTP on follow-up CT. LTC = local tumor control, LTP = local tumor progression
![]()
CT Follow-Up for Peritoneal Seeding
Table 3 summarizes the results of 6-week post-RFA CT follow-up in the DTP-RFA, NtRFA, and control groups. Regarding peritoneal seeding, the DTP-RFA group showed a significantly higher incidence than that of the NtRFA group (71.4% vs. 21.4%, p = 0.021). The control group showed no evidence of peritoneal seeding or skin seeding. Lymph node metastasis and lung metastasis varied among the three groups without statistical significance. All peritoneal seeding and lymph node metastases detected on CT were confirmed on pathologic analysis. Representative cases are presented in Figures 4 and 5.
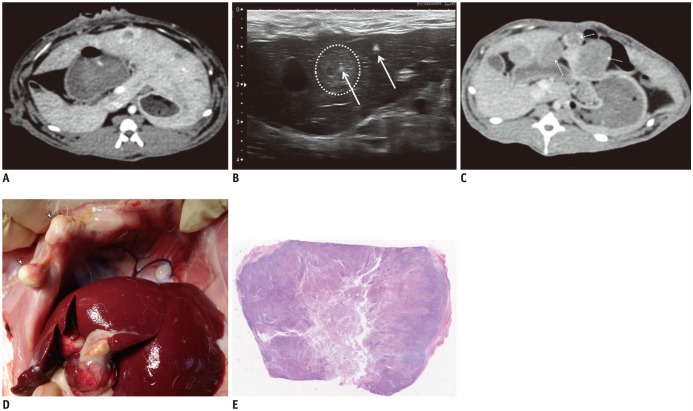
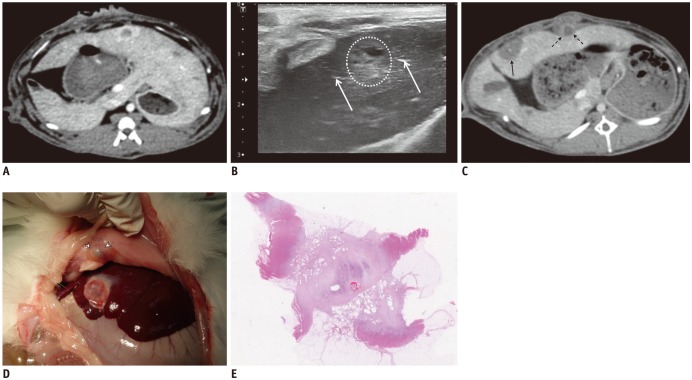

Fig. 4
DTP-RFA.
A. Pre-RFA CT showing 0.8 cm peripheral enhancing tumor in left medial lobe subcapsular area. B. US-guided RFA was performed, and one of two dual bipolar needles (arrows) accurately penetrated tumor (dotted circle). C. 6-week post-RFA CT reveals multiple peritoneal seeding nodules (dotted arrows) and local recurrence (double lined arrow) at inferior aspect of previous tumor. D. Gross anatomic picture showing peritoneal seeding nodules (arrowheads) and local recurrence. Lung metastasis (asterisk) also appears. E. H&E staining of peritoneal seeding nodules confirmed VX2 carcinoma. US = ultrasonography
![]()
Fig. 5
NtRFA.
A. Pre-RFA CT showing 0.7 cm peripheral enhancing tumor in left medial lobe subcapsular area. B. US-guided RFA was performed, and dual bipolar needles (arrows) accurately penetrated periphery of tumor (dotted circle). C. 6-week post-RFA CT reveals complete ablation of tumor (double line arrow) with small amount of localized fluid collection within soft tissue anterior to left lobe of liver (dotted arrows). D. Gross anatomic picture showing complete necrosis of tumor (asterisk) and localized peritoneal fluid collection (arrowheads). E. H&E staining of peritoneal fluid collection confirmed reactive fibrosis with few lymphocytes and no tumor.
![]()
Table 3
Results of 6-Week Post-RFA CT Follow-Up in DTP-RFA, NtRFA, and Control Group
![]()
Tumorigenic Factor
Serum levels of HGF, VEGF, and Il-6 were too low to detect in all three groups (DTP-RFA, NtRFA, and control). Additionally, measurements of the Ki-67 proliferation marker in the ablated lobe (three days after ablation) did not differ among the three groups (per high-power microscopy frame: DTP-RFA, 7.5 ± 3.0; NtRFA, 8.1 ± 4.1; control, 3.0 ± 1.6; p = 0.494) (Supplementary Table 3 in the online-only Data Supplement).
DISCUSSION
In the current study, our results demonstrated that NtRFA led to the development of less peritoneal tumor seeding than DTP-RFA in subcapsular VX2 liver tumors implanted in rabbits. In addition, NtRFA showed a tendency toward better LTC than DTP-RFA (DTP-RFA 56% [14/25] vs. NtRFA 80% [20/25], p = 0.069) based on both pathologic assessment and a combination of contrast-enhanced CT and autopsy findings. However, no difference was found in tumorigenic factor elevation between DTP-RFA and NtRFA. On the basis of these results, NtRFA may provide a better clinical outcome for subcapsular HCCs than DTP-RFA and could be a better choice of technique when RFA is used as a bridge therapy to liver transplantation.
Peritoneal tumor seeding is one of the most unfavorable complications after RFA for liver malignancies such as HCC or colorectal liver metastases. Many previous studies have reported the incidence of tumor seeding after RFA for HCC ranging from less than 1.5% (29303132) to 4.0% (33), although a higher rate of 12.5% was reported by one center (34). Most of the previous studies, however, dealt with the DTP-RFA technique and suggested various risk factors such as subcapsular location (3334), prior biopsy (3032), poorly differentiated tumors (34), and lack of cauterization of the electrode track (3132). Possible mechanisms for peritoneal tumor seeding after DTP-RFA include facilitation of viable cancer cell dissemination by increased intratumoral pressure (2529), direct tumor implantation through a needle (31), or direct migration of tumor cells via bleeding into the peritoneal cavity (2931). Therefore, RFA is generally not a preferred procedure for subcapsular tumors, and it has been widely accepted that direct insertion of the electrode into the tumor should be avoided (353637). As NtRFA alternatively places the probes in the liver parenchyma surrounding the tumor margin, there is reduced risk of direct tumor implantation through the needle or via bleeding from the tumor. In addition, NtRFA can induce vessel coagulation around the tumors, and therefore produces relatively less intratumoral pressure than DTP-RFA (2), which in turn would lead to lower peritoneal seeding. Accordingly, recent clinical studies dealing with NtRFA have reported no peritoneal seeding (2538), although most of them have been retrospective studies with small sample sizes.
No-touch radiofrequency ablation is known to improve the rate of complete necrosis, as a result of a larger ablation volume with ablation developing in the centripetal direction, creating a margin of safety. Seror et al. (8) reported enhanced completeness of necrosis with NtRFA (26 out of 29, 89.6%) in comparison to DTP-RFA (14 out of 30, 46.6%) in patients with HCC. In our experiment, we found a similar trend for NtRFA to produce better LTC than DTP-RFA, but it failed to reach statistical significance (p = 0.069). This can probably be attributed to the biological features of VX2 tumors, which develop multiple tiny satellite nodules around the main implanted tumor when they reach more than 2 cm in diameter. On follow-up CT and autopsy, despite complete necrosis of the target tumor, LTP was found to develop around satellite nodules, which may be related to the aggressiveness of infiltrative growth of VX2 tumors. At the same time, it is interesting to note that in three rabbits with viable satellite nodules in the DTP-RFA group, the satellite nodules were located more than 5 mm from the main tumor, and one of the rabbits developed intravascular tumor emboli. Conversely, the NtRFA group and the control group only showed satellite nodules within 2 mm of the main tumor. This may reflect facilitated local dissemination and a subsequent trend toward poor local control rate with DTP-RFA, resulting from intratumoral placement of electrodes, intratumoral pressure increases, and the centrifugal direction of ablation with late vascular perfusion blockage during the ablation, recapitulating previous observations that manipulation of the tumor during surgery may aggravate postoperative recurrence and distant metastasis (394041) and that early vascular flow control prior to manipulation of tumors may improve the survival outcome (42).
It is also interesting that in our study, the number of total punctures per RFA procedure differed significantly between the two techniques (DTP-RFA; 2 [median] [range: 2–3], NtRFA; 3 [2–5], p < 0.001). Furthermore, all three cases with peritoneal seeding in the NtRFA group in our study required more than four punctures due to the repositioning of unsatisfactory initial electrode insertions without intervening RF heating (43). We assume that during the repositioning, peri-nodular satellite tumor nodules may have been perturbed, resulting in facilitation of tumor seeding. Indeed, NtRFA is a more demanding technique that requires a longer learning curve than DTP-RFA (2). Despite the technical and experimental difficulty, it is noteworthy that a statistical difference was still found between NtRFA and DTP-RFA. Nonetheless, considering that radiologists are accustomed to placing electrodes in the central portion of a tumor for ultrasound-guided biopsy or ablation procedures, it can be expected that there would be a longer learning curve for NtRFA, which requires placing electrodes in the peritumoral zone with appropriate geometry.
Finally, there has recently been increasing experimental evidence that hepatic RFA may contribute to the release of tumorigenic factors that stimulate tumor development, growth, or more aggressive biology, either at separate sites within the same organ or in a distant tumor. However, in our study, we found no increase in tumorigenic factors such as IL-6, HGF and VEGF, and no difference in the Ki-67 proliferation index in among the RFA groups (NtRFA and DTP-RFA) and the control group. We attribute this contrary result to differences in our study design, as we used a rabbit model while previous studies have been conducted on smaller animal models (mice (1617) and rats (1415)).
There are several limitations in our study that need to be acknowledged. First, there was a technical challenge in performing US-guided RFA of VX2 tumors in rabbit livers due to the anatomy of the rabbit liver, which has five lobes of the racemose type, and due to the small size of the tumors. Nevertheless, we attempted to mimic real clinical practice, and found a statistical difference between DTP-RFA and NtRFA regarding the development of peritoneal seeding. Second, another limitation is the relatively small sample size. Additional study with an expanded number of subjects and clinical scenarios is warranted to obtain greater statistical significance. Third, we also found that the incidence of peritoneal seeding was higher in our study (71.4% in DTP-RFA, 21.4% in NtRFA) than in previous studies dealing with humans (1.5–12.5%). We believe that this might be attributable to the subcapsular location of the tumors and the virulence of the VX2 carcinoma. Given the innate differences in tumor characteristics of VX2 carcinoma in the rabbit model and those of HCC in humans, caution is warranted when generalizing the incidence of peritoneal seeding between studies on rabbits and humans. Fourth, considering the low detection rate of small peritoneal seeding and lymph node metastasis on CT, there may have been undiagnosed pathologic peritoneal seeding or lymph node metastasis that was not detected on prior CT. Further evaluation with thorough pathologic analyses should be conducted to compare the results of pathologic and imaging examinations. Finally, as noted earlier, using a small animal model with VX2 tumors may be a limitation in extrapolating our data to the clinical setting, as the biological behavior of VX2 tumors may differ from that of human HCC. Nevertheless, we believe this study presents reasonable preclinical proof of improved safety and treatment efficacy of NtRFA in subcapsular hepatic tumors.
In conclusion, we demonstrated that NtRFA produces a lower peritoneal seeding rate and a tendency toward better LTC than DTP-RFA, which may contribute to better treatment in subcapsular hepatic tumors and serve as an attractive bridge therapy to liver transplantation.
 XML Download
XML Download