

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cardiothoracic computed tomography (CT) is useful for evaluating congenital heart disease
in children, and electrocardiography (ECG)-synchronized CT data acquisition significantly
reduces cardiac motion artifacts (1234567). However,
respiratory motion artifacts often degrade the image quality of cardiothoracic CT in
free-breathing children. The recently introduced high-pitch dual-source spiral CT imaging
technique can provide excellent coronary artery image quality in adult patients (891011121314151617) and
substantially reduces respiratory motion artifacts in free-breathing patients (14). Two types of scan methods, non-ECG-synchronized and
prospectively ECG-triggered methods, are available for high-pitch dual-source spiral CT
imaging techniques (8). Prospectively ECG-triggered
high-pitch scanning is primarily used for coronary CT angiography because it produces
excellent whole heart image quality in a single cardiac cycle (910121314151617).
High-pitch dual-source spiral CT is highly effective at not only reducing both cardiac and
respiratory motion artifacts in free-breathing children, but also at achieving low radiation
dose (18192021222324). Among previous studies, both
non-ECG-synchronized high-pitch scanning (182324) and
prospectively ECG-triggered high-pitch scanning have been utilized (19202122). However, it has not yet
been determined whether prospective ECG triggering may add additional value to high-pitch
dual-source spiral scanning in free-breathing children, which is particularly crucial in
evaluating congenital heart disease. Therefore, this study aimed to compare image quality
and radiation dose of free-breathing high-pitch dual-source spiral cardiothoracic CT between
non-ECG-synchronized and prospectively ECG triggered data acquisitions in young children
with congenital heart disease.
Go to : 
MATERIALS AND METHODS
This retrospective study was approved by the local Institutional Review Board and informed
consent was waived.
Study Population
Between October 2010 and November 2016, 3127 pediatric cardiothoracic CT examinations
were performed. Among these, 509 CT studies (16.3%) were acquired with high-pitch
dual-source spiral scanning (357 studies using non-ECG synchronized scanning and 152
studies using prospectively ECG-triggered scanning). Exclusion criteria included patients
older than 3 years of age, the use of tube voltages other than 80 kV (n = 14 for 70 kV, n
= 2 for 100 kV in patients younger than 3 years of age), previous history of severe side
effects from iodinated contrast agent, and severe renal failure. Finally, 86 children with
congenital heart disease who underwent free-breathing high-pitch dual-source spiral
cardiothoracic CT at 80 kV were included in the study and divided into two age, sex, and
body size-matched groups (n = 43 for each; group 1 for non-ECG-synchronization and group 2
for prospective ECG triggering) to compare image quality and radiation dose (Table 1).
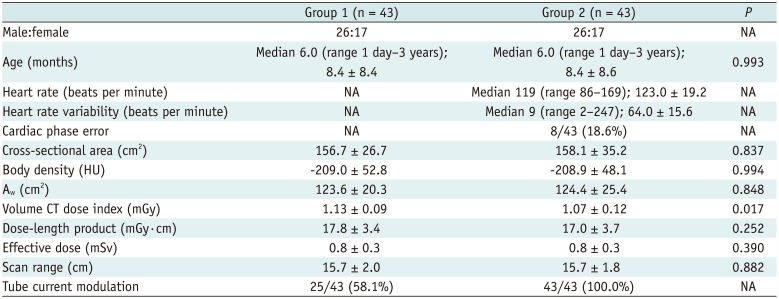
Table 1
Patient Characteristics and Radiation Dose of High-Pitch Dual-Source Pediatric Cardiothoracic CT in Two Groups
![]()
Congenital heart diseases in group 1 were as follows: 17 cases of functional single
ventricle, 11 coarctation of the aorta, three pulmonary atresia with ventricular septal
defect (VSD), two VSD, two double outlet right ventricle, two interrupted aortic arch, two
anomalous pulmonary venous return, two atrial septal defect, one aberrant left subclavian
artery, one truncus arteriosus, and one pulmonary atresia with intact ventricular septum.
While those in group 2 comprised: 22 case of functional single ventricle, three double
outlet right ventricle, three anomalous pulmonary venous return, two coarctation of the
aorta, two VSD, two pulmonary atresia with VSD, two pulmonary atresia with intact
ventricular septum, two aberrant left subclavian artery, one tetralogy of Fallot, one
atrioventricular septal defect, one congenitally-corrected transposition of the great
arteries, one patient ductus arteriosus, and one sinus of Valsalva aneurysm. Reasons for
cardiothoracic CT examination in the two groups are summarized in Table 2.
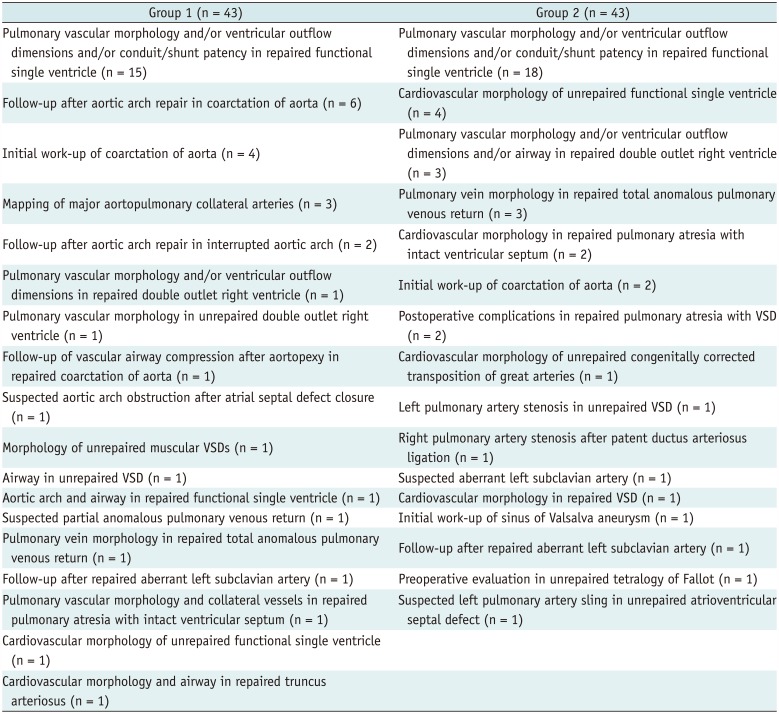
Table 2
Reasons for Cardiothoracic CT Examinations in Two Groups
![]()
High-Pitch Dual-Source Spiral Cardiothoracic CT
High-pitch dual-source spiral cardiothoracic CT was performed using a 128-slice
dual-source scanner (SOMATOM Definition Flash; Siemens Healthineers, Forchheim, Germany)
with 2 × 64 × 0.6 mm slices using the z-flying focal spot technique, a
gantry rotation time of 280 msec, a temporal resolution of 75 msec, a 0.75-mm slice width,
and a 0.4-mm reconstruction interval during free-breathing in all patients. In our
institution, the high-pitch dual-source spiral scan mode is mainly utilized, if the
assessment of coronary artery anatomy or ventricular function is not critical or when a
patient is so clinically unstable they need an ultrafast scanning technique. For patient
sedation, oral choral hydrate (50 mg/kg) was initially administered with additional
intravenous midazolam (0.1 mg/kg) or ketamine (1 mg/kg) as required.
In January 2013, the scan mode of high-pitch dual-source spiral cardiothoracic CT was
changed from non-ECG-synchronized data acquisition to prospectively ECG-triggered data
acquisition, expecting an additional benefit of the latter in free-breathing young
children. Non-ECG-synchronized scanning was obtained with pitch 3.2 in group 1 and
prospectively ECG-triggered scanning was acquired with pitch 3.4 in group 2. In group 1,
caudocranial CT scan direction was used to minimize perivenous streak artifacts resulting
from undiluted contrast agent. In group 2, craniocaudal or caudocranial CT scan direction
was used to adjust the scan range during the end-systolic phase on the ECG in the
conotruncal region of the heart for each patient. Since their heart rates exceeded 75
beats per minutes, the end-systolic cardiac phase rather than mid-diastolic phase was used
in all patients by targeting the second half of the T wave on ECG as previously described
(29). ECG
electrodes were placed in regions far away from the scan range, such as on the shoulder,
arms, and abdomen to avoid streak artifact from the metallic electrodes (Fig. 1). Cardiac phase error was defined to be present
when the R wave on ECG was included in a scan period or the second half of the T wave was
not included in a scan period (Fig. 2). In group 2,
average heart rates during CT examination were recorded and heart rate variability was
calculated by subtracting minimal heart rate from maximal heart rate during CT
examination. However, heart rates were not available in group 1 without ECG records during
CT examination and therefore could not be compared between the two groups.
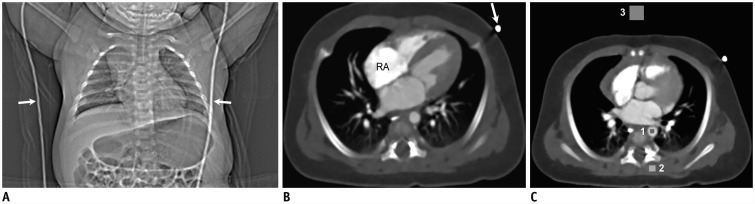 | Fig. 177-day-old boy with coarctation of aorta.
A. CT scout image shows ECG cables (arrows) for prospective ECG triggering.
ECG electrodes placed on both arms are not shown on CT scout image. B. Axial
CT image showing left-side ECG cable (arrow) causing mild streak artifact. Mild streak
artifacts also are shown around RA. As result, degree of streak artifacts was assessed as
grade 3 indicating mildly degraded image quality. C. Axial CT image at level
of aortic sinus shows locations of three rectangular regions of interest for measuring CT
densities in descending aorta (1), paraspinal muscle (2), and air (3). CT = computed
tomography, ECG = electrocardiography, RA = right atrium
|
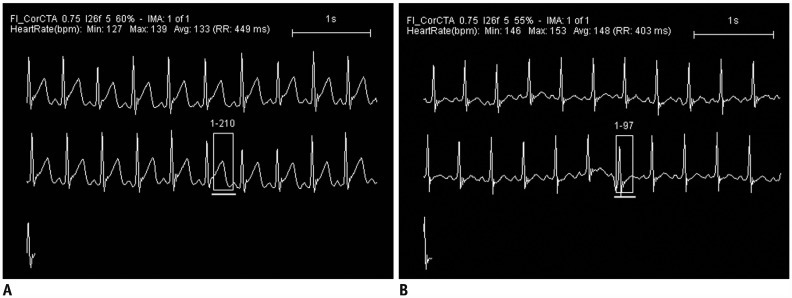 | Fig. 2Scan period positions in prospectively ECG-triggered high-pitch dual-source cardiothoracic CT scanning on ECG.
A. In 77-day-old boy with coarctation of aorta and cervical aortic arch,
scanning period on ECG, indicated by rectangle, is optimally located, starting from T wave
and finishing with P wave peak. B. In contrast, scanning period on ECG,
indicated by rectangle, is poorly positioned, overlapping with R wave in 13-day-old boy
with hypoplastic left heart syndrome.
|
To obtain uniform image noise, a volume CT dose index value based on a 32-cm phantom was
individually determined. This was based on the cross-sectional area and mean body density
measured on an axial CT image obtained approximately 1–2 cm above the dome of the
liver for bolus tracking (25). Patient diameter or
area is often used to reflect patient body size. However, body density should be
incorporated into these indices in order to avoid substantial errors especially in the
thoracic region (26). Consequently,
water-equivalent diameter or area may be used to indicate patient body size with high
fidelity and can be utilized in CT radiation dose optimization. Water-equivalent area
(Aw) was calculated from the measured cross-sectional area (Abody)
and mean body density (Dbody) of each patient by using the following
formula:
An adaptive section collimator was used to reduce additional radiation exposure due to
z-overscanning in both groups as described in previous studies (818). Combined tube current
modulation (CARE Dose 4D; Siemens Healthineers) was not always used because its
dose-saving effect was disputable in the high pitch value (3.2) in group 1; while it was
used in all patients despite the high pitch value (3.4) in group 2 expecting an additional
dose-saving effect (Table 1).
In addition to thin-section axial CT images, 2- or 3 mm-thick axial, coronal, sagittal,
and oblique reformatted CT images were reconstructed. For image reconstruction, the
sinogram-affirmed iterative reconstruction (SAFIRE; Siemens Healthineers) strength 5 with
a medium smooth kernel (I26f) was used. Iodinated contrast agent (Iomeron [iomeprol] 400,
400 mg I/mL; Bracco Imaging SpA, Milan, Italy; 1.5–2.0 mL/kg) was intravenously
administered at an injection rate of 0.2–1.0 mL/s using a dual-head power injector
and a tri-phasic injection protocol, in which undiluted contrast agent was followed by 50%
diluted contrast agent and then by 5% diluted contrast agent. This was performed to
achieve uniform cardiovascular enhancement and minimal perivenous streak artifacts from
undiluted contrast agent. More specifically, the first, second, and third parts of the
tri-phasic protocol contribute to optimal systemic arterial and left heart, pulmonary
vascular and right heart, and systemic venous enhancements, respectively. The scan delay
time was determined by a bolus tracking technique with a trigger threshold of 150
Hounsfield units (HU) in the left ventricular cavity.
Comparison of CT Radiation Dose
The volume CT dose index and dose-length product values based on a 32-cm phantom of
cardiothoracic CT displayed on the patient protocol were recorded. Effective dose values
of cardiothoracic CT were calculated by multiplying the dose-length product with patient
age and gender, and tube voltage-specific conversion factors for chest CT (27).
Quantitative Evaluation of CT Image Quality
On axial CT images at the level of the aortic valve sinus, CT density was measured in the
descending aorta, paraspinal muscle, and air by placing rectangular regions of interest in
the areas showing homogeneous attenuation (Fig. 1C).
In particular, a lung window setting was used to avoid the interference of patient clothes
and blanket in the measurement of air density. Although the same tube voltage (80 kVp) was
used in all cardiothoracic CT scans, standard deviations of aortic and muscular densities
might be affected by a different level of contrast enhancement. Therefore, the standard
deviation of air density was used for image noise on the CT images. Since a 2- or 3-mm
slice thickness (S) was used to reconstruct thick-section axial CT images, the image noise
(σ) was normalized to a slice thickness of 3 mm using the following formula:
From aortic density (Daorta) and slice thickness-normalized image noise from
air density (σair), signal-to-noise ratio (SNR) was calculated using the
following formula:
From mean aortic density (Daorta), muscle density (Dmuscle), and
slice thickness-normalized image noise from air density (σair),
contrast-to-noise ratio (CNR) was calculated using the following formula:
Subjective Evaluation of CT Image Quality
Subjective CT image quality was assessed by a pediatric radiologist with 17 years of
experience in pediatric cardiothoracic CT. Motion artifact grade on axial, coronal,
sagittal, and oblique reformatted CT images was evaluated for the cardiac structures,
coronary arteries, ascending aorta, pulmonary trunk, lung markings, diaphragm, and chest
wall using a 4-point scale (grade 1, severely degraded; grade 2, moderately degraded;
grade 3, mildly degraded; and grade 4, excellent, no artifact). In addition, the grade of
streak artifacts, including those resulting from ECG electrodes on axial, coronal, and
sagittal CT images was assessed using the same 4-point scale. Motion artifacts in the lung
markings were evaluated using the lung window setting while others were evaluated using
the mediastinal window setting. To evaluate intra-observer variability in subjective image
quality grading, the second session of the evaluation was repeated 6 months after the
first session and these two values then were averaged. The overall grade was subsequently
calculated as the average of these eight grades for each patient.
Statistical Analysis
For statistical analysis, the statistical software SPSS (version 24.0; IBM Corp., Armonk,
NY, USA) was used. Continuous or ordinal variables are presented as mean ± standard
deviation or median with range, and categorical variables are expressed as frequency with
percentage. Unpaired t test and Mann-Whitney U test were used to compare the difference
between two means of continuous and ordinal variables, respectively, between the two
groups. In group 2, subjective image quality was compared between two subgroups, with and
without cardiac phase error. Intra-observer agreement on subjective image quality of
high-pitch dual-source spiral cardiothoracic CT was evaluated using Cohen's kappa
statistics. A p value of less than 0.05 was considered to be
statistically significant.
Go to :
RESULTS
Patient Characteristics
Patient characteristics in the two groups are described in Table 1. No significant differences in age (8.4 ± 8.4 months vs.
8.4 ± 8.6 months, p = 0.993), cross-sectional area (156.7 ±
26.7 cm2 vs. 158.1 ± 35.2 cm2, p = 0.837),
body density (−209.0 ± 52.8 HU vs. −208.9 ± 48.1 HU,
p = 0.994), and Aw (123.6 ± 20.3 cm2 vs.
124.4 ± 25.4 cm2, p = 0.848) were found between group 1
and group 2, respectively (Table 1). In group 2,
average heart rate and heart rate variability during CT examination were 123.0 ±
19.2 beats per minute and 17 ± 38 beats per minute, respectively. Erroneous
selection of cardiac phases in prospective ECG triggering occurred in eight out of 43
patients (18.6%) in group 2.
CT Radiation Dose
CT radiation dose parameters in the two groups are summarized in Table 1. No significant differences in dose-length product (17.8
± 3.4 mGy·cm vs. 17.0 ± 3.7 mGy·cm, p =
0.252), effective dose (0.8 ± 0.3 mSv vs. 0.8 ± 0.3 mSv, p
= 0.390), and scan range (15.7 ± 2.0 cm vs. 15.7 ± 1.8 cm,
p = 0.882) were found between group 1 and group 2, respectively (Table 1). In contrast, volume CT dose index values of
group 1 (1.13 ± 0.09 mGy) were significantly higher than those of group 2 (1.07
± 0.12 mGy, p = 0.017) (Table
1). Combined tube current modulation was used in 25 out of 43 patients (58.1%) in
group 1 and in all patients in group 2 (Table
1).
Quantitative Image Quality
Quantitative image quality parameters in the two groups are described in Table 3. There were no significant differences in the
measured CT densities in the descending aorta (398.2 ± 117.3 HU vs. 429.6 ±
126.3 HU, p = 0.240), paraspinal muscle (76.8 ± 11.6 HU vs. 76.5
± 12.0 HU, p = 0.910), or air (−984.0 ± 27.6 HU vs.
−987.6 ± 23.4 HU, p = 0.650) between group 1 and group 2,
respectively (Table 3). In contrast, significantly
higher image noise (3.8 ± 0.7 HU vs. 3.3 ± 0.6 HU, p
< 0.001), and significantly lower SNR (105.0 ± 28.9 vs. 134.1 ± 44.4,
p = 0.001) and contrast noise-to-ratio (84.5 ± 27.2 vs. 110.1
± 43.2, p = 0.002) were found in group 1 compared with group 2
(Table 3).

Table 3
Quantitative Image Quality Evaluation of High-Pitch Dual-Source Pediatric Cardiothoracic CT in Two Groups
![]()
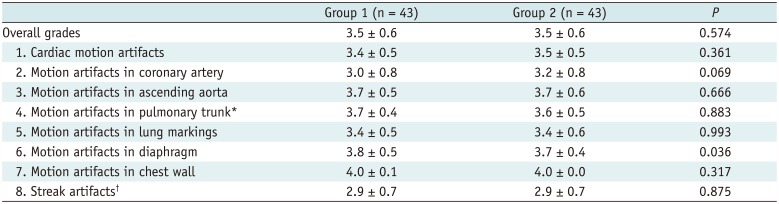
Subjective Image Quality
Subjective image quality parameters in the two groups are summarized in Table 4. There were no significant differences in
overall grades (3.5 ± 0.6 vs. 3.5 ± 0.6, p = 0.574),
cardiac motion grades (3.4 ± 0.5 vs. 3.5 ± 0.5, p = 0.361),
coronary artery motion grades (3.0 ± 0.8 vs. 3.2 ± 0.8, p =
0.069) (Fig. 3), ascending aorta motion grades (3.7
± 0.5 vs. 3.7 ± 0.6, p = 0.666), pulmonary trunk motion
grades (3.7 ± 0.4 vs. 3.6 ± 0.5, p = 0.883), motion grades
in lung markings (3.4 ± 0.5 vs. 3.4 ± 0.6, p = 0.993)
(Fig. 4), chest wall motion grades (4.0 ±
0.1 vs. 4.0 ± 0.0, p = 0.317), or grades of streak artifacts (2.9
± 0.7 vs. 2.9 ± 0.7, p = 0.875) between group 1 and group
2, respectively (Table 4). In contrast, diaphragm
motion was significantly less in group 1 (3.8 ± 0.5) than in group 2 (3.7 ±
0.4, p = 0.036) (Table 4, Fig. 4). In group 2, streak artifacts from the ECG
electrodes for prospective ECG triggering was shown in only one patient (2.3%, 1/43). In
contrast, the ECG electrodes placed on the patient's back in admission wards infrequently
caused streak artifacts in both groups. Cohen's kappa coefficient was 0.63
(p < 0.001) indicating a good intra-observer agreement.
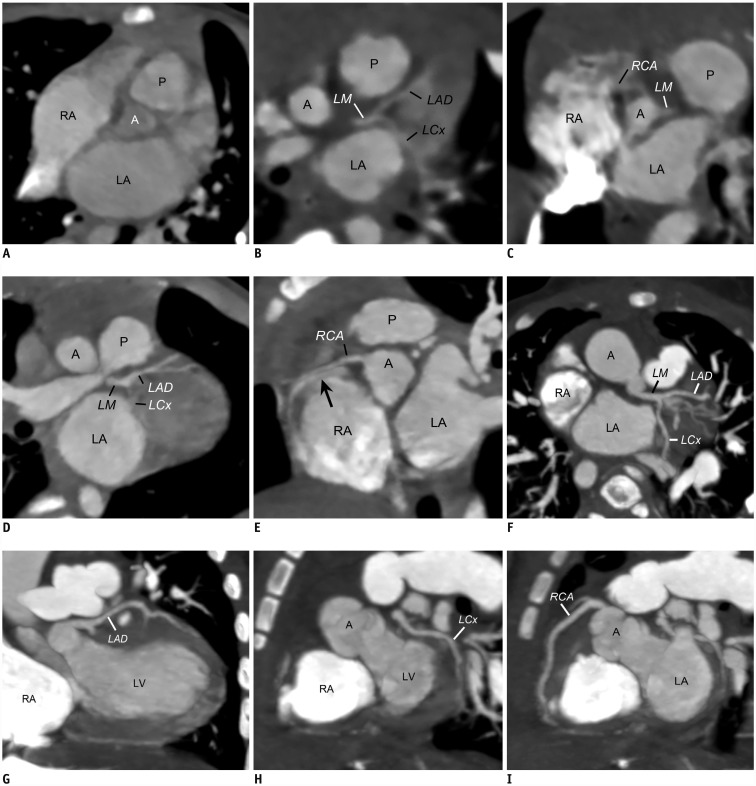 | Fig. 3Coronary artery motion artifact grading of high-pitch dual-source cardiothoracic CT.
A. Oblique coronal CT image acquired with prospective ECG triggering in
35-day-old boy with coarctation of aorta demonstrates severe motion artifacts on coronary
arteries that corresponded to grade 1. Oblique CT images (B, C) acquired
without ECG synchronization in 1-day-old girl with coarctation of aorta illustrate
moderate motion artifacts on coronary arteries, especially right coronary artery, which
correspond to grade 2. Oblique CT images (D, E) acquired without ECG
synchronization in an 11-month-old boy with surgically closed atrial septal defect reveal
mild motion artifacts (grade 3), especially on right coronary artery, including doubling
artifact (arrow) at proximal segment. Oblique CT images (F–I) acquired
without ECG synchronization in 6-month-old boy with double-outlet right ventricle show no
motion artifacts on coronary arteries including left main artery, left anterior descending
artery, left circumflex artery, and right coronary artery that corresponded to grade 4. A
= ascending aorta, LA = left atrium, LAD = left anterior descending artery, LCx = left
circumflex artery, LM = left main artery, LV = left ventricle, P = pulmonary trunk, RCA =
right coronary artery
|
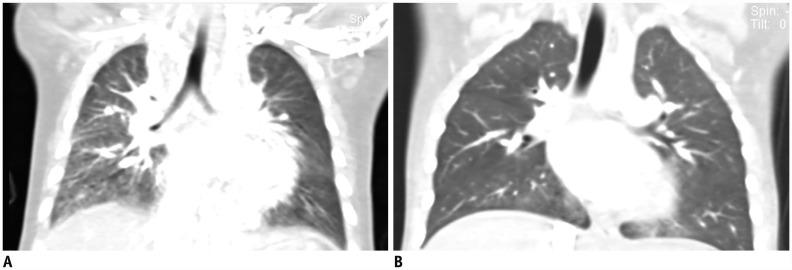 | Fig. 4Lung window setting CT images illustrating motion artifacts in lung markings and diaphragms.
A. Coronal CT image acquired without ECG synchronization in 6-month-old boy
with functional single ventricle shows moderate degrees of motion artifacts (grade 2) in
lung markings as well as in diaphragm. B. Coronal CT image acquired without
ECG synchronization in 3-year-old boy with repaired coarctation of aorta displays no
motion artifacts (grade 4) in lung markings as well as diaphragm.
|
Table 4
Subjective Image Quality Evaluation of High-Pitch Dual-Source Pediatric Cardiothoracic CT in Two Groups
![]()
In the subgroup analysis of group 2, cardiac phase error significant degraded not only
overall image quality, but also the image quality of the cardiac structures, coronary
arteries, and ascending aorta (Table 5).
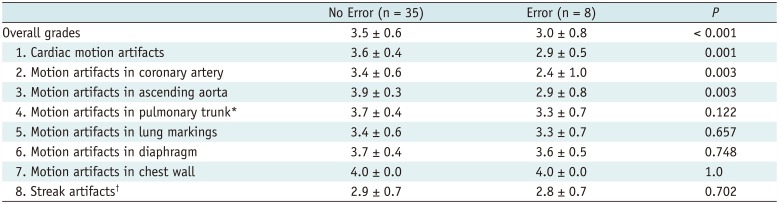
Table 5
Effect of Cardiac Phase Error on Subjective Image Quality in Group 2
![]()
Go to :
DISCUSSION
This study demonstrated that image quality and radiation dose of free-breathing high-pitch
dual-source spiral pediatric cardiothoracic CT were comparable between non-ECG synchronized
scans and prospectively ECG-triggered scans. This finding is in accordance with previous
studies comparing between non-ECG-synchronized and prospectively ECG-triggered scan modes of
high-pitch dual-source spiral CT of the aorta in adults (2829). The two scan modes showed comparable
subjective and objective image quality of the aorta, including the aortic root and coronary
arteries, as well as radiation dose (2829). Consequently, prospective ECG triggering does not
add a substantial diagnostic gain to free-breathing high-pitch dual-source spiral
cardiothoracic CT in children with congenital heart disease and an additional workflow
required for ECG electrode placement may therefore be omitted.
The finding of equivalent dose-length product and effective dose between the two scan modes
appears to be reliable because patient-related parameters, such as age, sex,
Abody, Dbody, and Aw, potentially influencing CT
radiation dose, were strictly matched between the two groups. In contrast, volume CT dose
index values in group 1 were significantly higher than those in group 2, probably due to
less frequent use of tube current modulation. Unless tube current modulation was not
utilized in both groups, radiation dose may be equal between the two. Despite significantly
lower volume CT dose index values in group 2, σ was significantly lower in group 2
than in group 1. The result clearly highlights the usefulness of tube current modulation in
radiation dose optimization. The combination of slightly higher aortic enhancement and
significantly lower σ in group 2 led to significantly higher SNR and CNR in group 2
than in group 1.
Substantial reductions in respiratory motion artifacts on high-pitch dual-source spiral CT
have been already reported in both clinical and phantom studies (1830). In this study, motion
artifacts other than the diaphragm showed no significant difference between the two scan
modes. It remains unclear why a small but significant difference in diaphragm motion
artifacts was observed between the two groups. It is noteworthy that cardiac phases along
the z-axis are different in high-pitch dual-source spiral CT (8). Therefore, scan mode cannot be used for ventricular function assessment (3132). In
addition, image quality of the coronary arteries tends to be suboptimal at high heart rates
(8), which are common in children with congenital
heart disease. As a result, the sequential CT scan mode with combined respiratory and ECG
triggering is used for pediatric cardiothoracic CT in our institution, when the evaluation
of ventricular function and coronary artery anatomy is essential (33).
A previous study reported that streak artifacts resulting from ECG electrodes deteriorate
image quality of prospectively ECG-triggered high-pitch dual-source spiral CT (24). In this study, streak artifacts resulting from ECG
electrodes could be avoided in almost all patients by placing ECG electrodes outside the
longitudinal scan range. As a result, no significant difference in streak artifacts was
found between the two scan modes. In contrast, mild streak artifacts from undiluted contrast
agent were observed in both groups despite the utilization of the tri-phasic intravenous
injection protocol in this study. In high-pitch dual-source spiral CT, the scan delay for
optimal contrast enhancement should be adjusted so that its duration is sufficient to
compensate for an exceedingly short scan time (34).
In high-pitch dual-source spiral scanning, the use of low tube voltage may result in high
image noise due to tube current saturation (8). In
fact, this technical limitation often precludes the use of 70 kV for high-pitch dual-source
spiral scanning even in small children. To obtain the full advantages of 70 kV in high-pitch
dual-source spiral pediatric cardiothoracic CT, a higher radiation dose efficiency is
required using improved detector technology and iterative reconstruction algorithm, as well
as a stronger X-ray tube. For the same reason, automatic tube voltage selection software
leads to higher radiation dose in non-ECG-synchronized high-pitch dual-source spiral CT of
the aorta by escalating tube voltage from 100 kV to 120 kV in 80% of patients; this
contradicts previous results of automatic tube voltage selection software using
standard-pitch single-source scan (35).
This study has several limitations. First, two groups of 43 different patients with
different utilized CT scan modes were compared rather than paired examinations in the same
patients due to the retrospective nature of this study. However, patient age, sex, and body
size of the two groups were matched to increase the significance of the unpaired comparison.
Second, the use of tube current modulation during CT scanning was not completely equal
between the two groups. This is because its dose-saving effect during high-pitch dual-source
spiral scanning was questionable at that time. Nonetheless, an additional dose-saving effect
of tube current modulation was proven for high-pitch dual-source spiral scanning even with a
relatively short scan range, approximately 16 cm. Third, the degree of respiratory motion,
such as respiratory rate or respiratory excursion, between the two groups could not be
controlled in this retrospective study, and there were unexpectedly less diaphragm motion
artifacts in group 1 compared with group 2. Nonetheless, the results may at least suggest
non-inferiority of the non-ECG-synchronized scan mode in reducing respiratory motion
artifacts, compared with the prospectively ECG-triggered scan mode. Fourth, the pitches of
the two scans were slightly different: 3.2 for non-ECG-synchronized high-pitch dual-source
spiral scanning and 3.4 for prospectively ECG-triggered high-pitch dual-source spiral
scanning. These values were selected because they are the maximal values for each scan and
were expected to show the most beneficial effects in reducing motion artifacts. They were
different due to the retrospective nature of this study. However, a 0.2 difference in pitch
might not substantially affect the results of this study. Fifth, inter-observer agreement
was not evaluated in this study. However, intra-observer agreement was evaluated as in a
previous study (29). Sixth, diagnostic accuracy was
not compared because it was beyond the scope of the study.
In conclusion, additional ECG triggering does not substantially reduce motion artifacts on
high-pitch dual-source spiral pediatric cardiothoracic CT in young children with congenital
heart disease. In high-pitch dual-source spiral cardiothoracic CT, the use of tube current
modulation appears to reduce radiation dose.
Go to :
 XML Download
XML Download