

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Capitellar fractures account for approximately 1% of all elbow fractures and 6% of distal humerus fractures.1) Bryan and Morrey classification has been widely used to classify capitellar fractures and provide therapeutic guidelines.2) According to their system, type 1 fractures include a coronal shear fragment; type 2 result in a predominantly cartilaginous ‘thin’ fragment; type 3 are comminuted, multi-fragmented; and type 4 describe a shear fracture extended medially to the trochlea. Capitellar impaction fracture is an uncommon type of injury and is not encompassed by commonly used classification systems such as that of Bryan and Morrey.3) Furthermore, to the best of our knowledge, there have been only few cases reporting a capitellar impaction fracture with a radial head fracture.4) Herein, we present a case of capitellar impaction fracture in a 53-year-old female patient.
Case Report
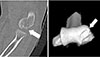
A 53-year-old female came to the emergency department after falling on to her left arm. She presented a painful and mild swollen elbow. On physical examination, her upper extremity was neurologically intact and there was no external wound. She complained of pain on palpation over the radio-capitellar joint of the elbow. It was impossible to apply the stress test to evaluate for any instability of the elbow due to severe pain. The patient's visual analogue scale (VAS) score was 6 out of 10 on the numeric rating scale (NRS)-11 and Mayo elbow performance score was 40. Anteroposterior and lateral radiographs revealed no visible fracture or dislocation (Fig. 1). We took computed tomography (CT) scan to find hidden fractures. The CT scan showed that distal articular cartilage of the capitellum was depressed about 1.7 mm (Fig. 2). There was linear radial head fracture on CT scan.
Under general anesthesia, varus and valgus stress test on the elbow was performed at 30° of elbow flexion; no significant instability was noted. The radio-capitellar joint was exposed through a posterolateral approach. The osteochondral fracture fragment of the capitellum was impacted and there was a step-off on the posterior articular surface. Though anterior one-third of the capitellar articular surface of the radius was peeled, there was no complete fracture on the radial head (Mason type I). Small cartilage fragments from the capitellum were removed (Fig. 3). Impacted osteochondral fragment of capitellum was lifted to make an articular congruence by using small osteotome and the stability was achieved by using rafting a 1.6 mm K-wire inserted parallel & beneath the fracture fragment and advanced into the medial part of the trochlea (Fig. 4, 5).
After four weeks of immobilization, a limited range of active and passive range of motion (ROM) was allowed. The patient received daily physical therapy, and her ROM-both active and passive-gradually increased. At the 4-months follow-up postoperatively, ROM of the elbow joint was 0° to 135°. Removal of ‘raft’ K-wire was performed and the congruence of articular surface of the capitellum was confirmed on follow-up CT scan (Fig. 6).
She feels comfortable using her elbow in daily life (combing hair, performing hygiene) without any complications. The VAS score of the patient was 0 out of 10 on the NRS-11, Mayo elbow performance score was 100 and Disabilities of the Arm, Shoulder, and Hand score was 0 for the disability/symptoms.
Discussion
Impacted fractures of the capitellum are uncommon, and the current body of literature is limited to case series whereby it is difficult to draw firm conclusions on injury mechanism and treatment. Moreover, because of the small size of the fracture fragments as well as overlapping of the radial head and capitellum fracture in plain radiographs, diagnosis is still challenging. To avoid a missed diagnosis and to facilitate precise preoperative planning, in patients with suspected capitellum fractures with a concomitant radial head fractures, CT scan of the affected elbow could be helpful.5)
Although the mechanism of this injury has not been clearly elucidated, the following can be assumed. The capitellum is at risk because of reciprocal impinging on the radial head. A total of 60% of the axial load at the elbow is transmitted through the radiocapitellar joint.46) This axial loading stress may be produced by a fall on the outstretched hand and the capitellum has collapsed by the impact of the radial head. As a consequence, osteochondral fracture and impaction of capitellum may be occurred.
Although this type of injury is not much important to joint stability that relies on both intact articular structures and soft tissue constraints (i.e., lateral collateral ligament, coronoid, and radial head), the bony contribution to radiocapitellar stability is provided by concavity-compressive forces.3) Incongruence of the radio-capitellar joint leads to posttraumatic arthrosis, stiffness and potential ulnohumeral instability.7) For these reasons, recovery of congruence in capitellar articular surface is necessary in our 1.7 mm depression case.
Reduction and internal fixation of the impacted fracture fragment is technically demanding, owing to the small and often comminuted nature of the fragments as well as the circumferential articular cartilage on the capitellum. We obtained the satisfactory clinical results through the ‘lever arm’ reduction of the fracture fragment with a small osteotome and fixation with ‘raft’ K-wire. This case demonstrates that good functional and anatomic results can be realized by open ‘lever arm’ reduction and fixation with ‘raft’ K-wire allowing early mobilization and a good recovery of elbow.
Our observations must be interpreted within the frameworks of the limitations. The clinical outcome of this patient must be compared and contrasted with another patient; however, to the best of our knowledge, there are no comparable clinical reports to date of this injury in the literature.





 XML Download
XML Download