

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Cerebral microbleeds (CMBs) on T2-weighted gradient echo (GRE) imaging are known to represent hemosiderin deposition in macrophages from previous blood extravasation. They are frequently detected in elderly patients with intracerebral hemorrhage (ICH), ischemic stroke, and incidental ICH.7)9)10)17)24)30) Many studies in the literature have reported that CMBs are prognostic neuroimaging markers for future hemorrhagic or ischemic stroke or hemorrhagic complications of antithrombotic and thrombolytic therapies.7)25)30)40)
Recently, in developing magnetic resonance imaging (MRI) technologies for detection of CMBs, many studies have applied the technologies to population-based elderly samples. In general, CMBs are mainly associated with two types of sporadic small vessel disease: hypertensive arteriopathy and cerebral amyloid angiopathy (CAA).5)15)26) These two types are characterized by different microbleed distribution patterns; CMBs associated with hypertensive vasculopathy tend to occur in the basal ganglia, thalamus, brainstem, and cerebellum, whereas CAA shows a lobar distribution.26)
CAA is diagnosed according to the Boston criteria.26) Several previous studies have demonstrated that the Boston criteria have good sensitivity and specificity in diagnosing pathologically proven CAA; however, there are still limitations in diagnosing pathologically unproven CAA.3)4) Consequently, many studies have attempted to modify the imaging criteria to improve the diagnostic power. Recently, centrum semiovale perivascular spaces (CSO-PVS) have been suggested as additional imaging markers of CAA.4)6)28)31) Several studies have reported that the severity of CSO-PVS, which are distinct pathophysiological processes compared with basal ganglia-PVS, might be related to the impaired interstitial fluid drainage of CAA.
However, in the clinical field, many physicians can easily locate CMBs with lobar distribution on MRI in patients aged < 55 years presenting with ICH. According to the Boston criteria of CAA diagnosis,26) patients who survive after hemorrhage are not suspected of having CAA unless pathological findings are present in those aged < 55 years.
The data on CMBs in younger patients presenting with ICH are lacking. Our goals were to analyze the prevalence of CMBs, characterize the distribution and risk factors in CMB development, and investigate the association between CMBs and other CAA markers in young patients with ICH.
Go to : 
MATERIALS AND METHODS
Study population and data collection
This study was approved by the Ilsan Paik hospital, Inje University, Institutinal Reveiw Board. This retrospective single-center study included patients who presented with spontaneous ICH. Electronic database searches were used to identify consecutive ICH patients who were admitted to our institution from December 2009 to August 2017. We studied a population of 272 consecutive patients aged 18–54 years who were admitted to our emergency department. Among these, we excluded 46 with structural and secondary causes of ICH, including arteriovenous malformations (n = 13), cerebral tumors (n = 5), moyamoya disease (n = 11), cavernous malformations (CM) (n = 3), trauma (n = 9), parasitic lesion (n = 1), and use of aspirin (n = 4). In addition, we excluded patients in whom GRE MRI was not applied and CMBs were not clearly differentiated from vessels.
We assessed many demographic features and vascular risk factors in patients with ICH, including age on admission, sex, hypertension, diabetes mellitus, hyperlipidemia, history of smoking, and history of antithrombotic agent use before and after ICH. Hypertension was defined as history of hypertension, use of an antihypertensive drug, or documented elevated blood pressure (BP) (systolic > 140 or diastolic > 90 mmHg). Diabetes was considered as fasting serum glucose level ≥ 126 mg/dL and hemoglobin A1c ≥ 6.5%, with previous or ongoing use of a hypoglycemic drug or insulin. Hyperlipidemia was defined as a previous diagnosis of hypercholesterolemia or current use of an antihyperlipidemic drug. Subjects who smoked at the time of enrollment were considered current smokers.
ICH was classified based on location as either deep or lobar type. Deep type was defined as ICH located within the basal ganglia, internal capsule, thalamus, brainstem, and cerebellum, and lobar type was defined as that located in the cerebral cortex, subcortex, and underlying white matter.
Most patients received intensive treatment during the acute phase and were subsequently transferred to the rehabilitation department and followed up on an outpatient basis in the neurosurgery department.
Computed tomography (CT) and brain MRI acquisition and analysis
CT scans on admission and brain MRIs were reviewed by two study investigators. ICH volume was calculated using the formula A × B × C / 2, where A is the greatest hemorrhage diameter on CT, B is the diameter 90° to A, and C is the approximate number of CT slices containing hemorrhage multiplied by the slice thickness. All subjects had an axial T2-weighted fast spin-echo sequence (repetition time (TR)/echo time (TE), 4,850/98 ms; flip angle 90°; FOV, 220 mm; slice thickness, 5 mm; slice gap, 6 mm) and a T2*-weighted gradient echo sequence (TR/TE, 800/26 ms; flip angle, 20°; field of view (FOV), 230 mm; slice thickness, 5 mm; slice gap, 6 mm) based on data obtained using a 1.5-Tesla MRI scanner.
Strictly lobar CMBs (size, 2–10 mm) were assessed on T2-GRE images using the Microbleed Anatomical Rating Scale (MARS).5)19) The MARS study classified microbleeds into “definite” and “possible” categories to improve reliability. However, we counted and enrolled only “definite” lesions on GRE MRI. Definite microbleeds were defined as small, rounded or circular, well-defined hypointense lesions within brain parenchyma with clear margins ranging from 2 to 10 mm in size on GRE T2-weighted imaging (WI).19) The location of CMBs was classified as either deep or lobar, similar to the abovementioned ICH classification. CMB mimics included cavernous malformation, calcium and iron deposits, flow void, partial volume artifact from bone, metastatic melanoma, and diffuse axonal injury. CMB mimics have morphology and signal characteristics similar to CMBs.18) Cavernomas are distinguishable from typical primary CMBs based on appearance on both T1- and T2-WI of stagnant blood in the sinusoidal lumen, extravasated blood at varying stages of degradation, and characteristic hemosiderin rim.1)5)18)
CSO-PVS were assessed and rated on axial T2-WI according to recent consensus criteria.39) After reading all relevant slices for the anatomical area being assessed, the side of the slice with the highest number of CSO-PVS was recorded. To confirm our hypothesis, severity was categorized into low- (n ≤ 20) and high-degree (n > 20) groups. CSO-PVS severity was interpreted by an independent board-certified neurosurgeon and an independent board-certified neuroradiologist. In cases of disagreement, we sought consensus between the two observers and a third interpreter.
White matter hyperintensity (WMH) was defined as a hyperintense lesion on T2-WI that remained bright on fluid-attenuated inversion recovery and was graded according to the modified Fazekas visual rating scale.14)34) WMH was assessed with the four-step simplified scale from 0 to 3 (0 = no lesions, 1 = focal lesions, 2 = early confluent, and 3 = confluent). Moderate-to severe WMH was assessed with a 2- or 3-step scale.
Statistical analysis
Statistical analysis was performed using IBM SPSS statistics version 21.0 (IBM, Armonk, NY, USA). Categorical variables were compared using Pearson chi-squared test or Fisher's exact test, whereas continuous variables were compared using the two-sample t-test or the Mann-Whitney U test. Multivariate logistic regression analysis was used to determine the independent clinical and radiologic characteristics associated with CMBs in ICH patients. The Kruskal- Wallis test was used to compare the age-related prevalence of CMBs. A p-value of <0.05 was considered statistically significant. Cohen's kappa statistic was used to test inter-rater reliability of CMB evaluation on MRI.
Go to :
RESULTS
We identified a total of 226 subjects with spontaneous ICH. Among these, we excluded those for whom MRI (n = 120) or GRE T2-WI (n = 38) was not performed and those for whom MRI or GRE did not show good reading quality (n = 2). The final cohort comprised 66 patients with a mean age of 45.3 years and 76% males. All patients presented with symptomatic ICH, including 21 with altered mental change, 44 with hemiplegia or hemiparesis, one with seizure combined with > 1 symptom, 29 with headache and dizziness, 38 with dysarthria, and three with blurred vision. Table 1 shows the demographic features according to ICH location in the 66 enrolled patients. Of ICH locations, 59 (89.4%) were of the deep type and 7 (10.6%) of the lobar type.
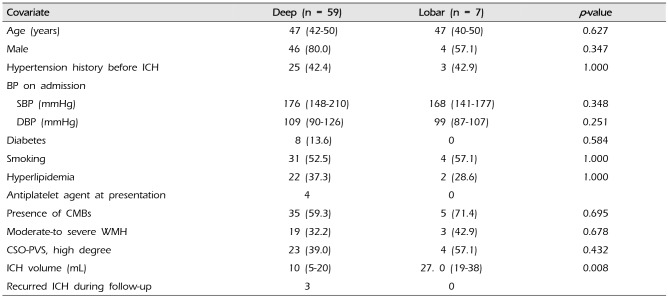
Table 1
Demographic characteristics, vascular risk factors for patients according to the ICH location (n = 66)
![]()
All enrolled patients were divided into two groups that were CMB+ or CMB− on GRE MRI. Among 66 spontaneous ICH patients, CMBs were detected in 40 (61%), with 29 (73%) being of the multifocal type; location of these CMBs was deep in 23 cases, lobar in one case, and both deep and lobar in 16 cases. Kappa coefficients for inter-rater agreements for MRI lesions of interest were 0.83 for CMBs, 0.90 for WMH, and 0.84 for CSO-PVS severity. In comparison with baseline characteristics according to CMB, a history of hypertension was more common in the CMB+ group than in the CMB− group (p = 0.040). In addition, high-degree CSO-PVS were more frequent in the CMB+ group. A total of 219 CMBs were counted on GRE MRI. Overall, 150 CMBs were of the deep type (68.5%) and 69 of the lobar type (31.5%) (Table 2).
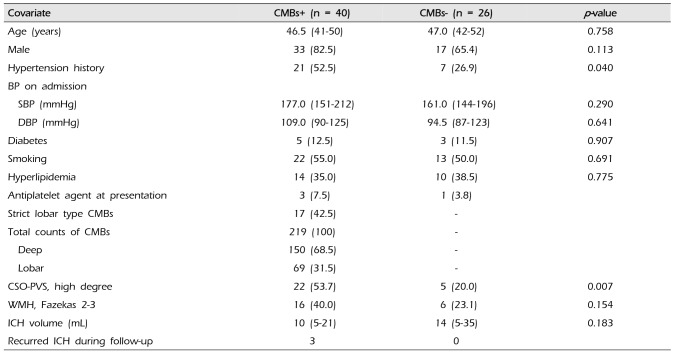
Table 2
Comparison of baseline characteristics according to CMBs presence
![]()
Variables for multivariate logistic regression analysis included age, sex, moderate-to-severe WMH, hypertension history, diabetes mellitus, hyperlipidemia, and smoking. In multivariate logistic regression analysis, hypertension history (adjusted odds ratio [aOR], 4.048; 95% confidence interval [CI], 1.14–14.32; p = 0.030) and male sex (aOR, 4.233; 95% CI, 1.09-16.48; p = 0.037) were independently associated with CMBs. Moderate-to-severe WMH (aOR, 3.876; 95% CI, 0.92–16.41; p = 0.066) tended to be associated with CMBs, although this association was not statistically significant (Table 3).
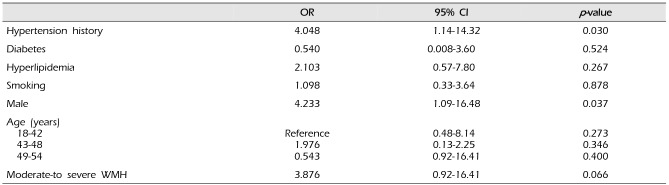
Table 3
Logistic regression analysis of risk factors for development of cerebral microbleeds in ICH patients
![]()
Among the 66 enrolled patients, 40 were treated continuously on an outpatient basis (median follow-up, 20.0 months; range, 1–87 months). When investigating recurrent episodes among the 40 patients, three (7.5%) had recurrent ICH events and were included in the GRE+ group (Table 2). However, the relationship between recurrent ICH and CMBs was not confirmed because GRE MRI was not performed at the time of first hemorrhage in three patients.
Go to :
DISCUSSION
The primary findings from our study are that a history of hypertension and male sex were independently associated with CMBs. In addition, moderate- to-severe WMH tended to be associated with CMB development.
In general, CMB development increases with age, possibly due to the strong association of advanced age with CMB risk factors such as leukoaraiosis, CAA, and hypertension.27) In a study on prevalence analysis of CMBs by Koennecke,27) the cohorts were grouped into three categories: without cerebrovascular disease, with ICH, and with ischemic cerebrovascular disease. Total CMBs were prevalent in 4.7% (range, 3.7–8.5) of elderly patients without cerebrovascular disease, 68% (range, 47–80) with spontaneous ICH, and 40% (range, 18–78) with ischemic disease.27) CMBs in our cohort were prevalent in 61% of patients, which is consistent with that reported in an elderly population with spontaneous ICH. Most of the CMB-relevant studies included elderly patients aged > 60 years; however, it was difficult to find comparable data in PubMed for characterization of CMBs in young patients presenting with spontaneous ICH.23)27)38)
CMBs of the lobar type have been known to reflect age-related progression of CAA in elderly patients.35)42) Koennecke insisted that the CMBs located in the lobar area in elderly patients may represent in vivo indicators of CAA.27) Although approximately 11% of our patients were admitted with ICH of the lobar type, there was a high proportion of CMBs (42.5%); 31.5% of these were of the lobar type despite the young age of the patients. In a study on young stroke patients conducted by Shoamanesh, 33% of the sample strictly had CMBs of the lobar type, which probably resulted more often from underlying CAA.37) Several studies have attempted to pathologically confirm CAA in patients aged < 55 years presenting with lobar ICH.33)41)
In studies on risk factors of CMBs in elderly patients with hemorrhagic or ischemic stroke, CMBs were associated with advanced age, male sex, hypertensive BP, diabetes mellitus, statin use, moderate-to-severe WMH, silent lacunar infarcts, global cortical atrophy, and hypoxemia.9)10)13)35)36)38) However, young people have fewer risk factors for cerebrovascular disease and degenerative markers on brain MRI, including moderate-to-severe WMH, lacunar infarcts, and cortical atrophy. Shoamanesh published the only study we could find in PubMed on CMB risk factors in young people.37) He reported that CMBs in young patients were independently associated with male sex, hypertension, moderate-to-severe WMH, and ICH.37) In our study, a history of hypertension and male sex were crucial risk factors for CMBs. Our study included only younger patients with spontaneous ICH but with risk factors were similar to those in the study by Shoamanesh.37)
Few papers have reported on how often CM cause ICH in young patients. Recent hemorrhage may completely or partially obscure the CM on MRI, which is why follow-up MRI is important for the diagnosis of a CM underlying an intraparenchymal hemorrhage.1) We identified three cases of hemorrhage from CM in our study according to Al-Shahi Salman's definition of CM hemorrhage.1)
Sufficient evidence suggests a causal link between CAA and WMH, but the significance of WMH for development of CMB is not well known.12)20)21) Recently, Charidimou et al.2) suggested that different patterns of subcortical white matter damage can provide insight into the dominant type of underlying arteriopathy with the potential mechanisms: multiple punctate FLAIR hyperintensities correlate with CAA and CAA-related imaging markers, whereas peri-basal ganglia WMH patterns are strongly correlated with hypertensive arteriopathy. In our study, we could not divide patients based on WMH patterns due to the small number of CMB patients. However, it is necessary to analyze whether meaningful results can be obtained for younger patients with ICH.
Recurrence after a first ICH episode has been considered a rare event in the past.11)16) However, recent studies have shown that the incidence of recurrent ICH ranged from 2.7% to 8.7%;8)22)29)32) our study had a recurrence rate of 7.5%. We will further assess whether there is a correlation between CMBs and ICH recurrence in patients requiring antithrombotic agents, and for this, a long-term follow-up of such patients is warranted.
This study has several limitations. First, there was selection bias because we included only spontaneous ICH patients who underwent GRE MRI. Second, the small number of subjects with spontaneous ICH led to weak statistical power for evaluating the prevalence and risk factors of CMBs. Third, this was a retrospective study that investigated the association and risk of CMBs in a group of patients with ICH. All patients were not treated surgically, and among patients with hematoma evacuation, pathologic biopsy was not performed for the purpose of CAA diagnosis. According to Boston CAA criteria, patients were classified on the basis of patients older than 55 years, and there were limitations in applying to young patients. To overcome these limitations, a prospective study or randomized controlled trial would provide further evidence to guide clinical practice.
Go to :
CONCLUSION
For young patients presenting with spontaneous ICH, CMBs are highly prevalent in 61% and strongly associated with history of hypertension and high-degree CSO-PVS. CAA may also be suspected in young patients when considering the variables associated with CMB development. Further study regarding the relationship between CMBs and ICH recurrence in patients requiring antithrombotic agents is needed.
Go to :
 XML Download
XML Download