

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Elasticity and viscosity of the cornea influence its functional responses and greatly affect vision.12 Many investigators, especially those who specialize in refractive surgery and glaucoma, have attempted to characterize biomechanical properties of the cornea due to its association with the diagnosis and treatment of patients with ocular abnormalities. Corneal biomechanical properties are known to influence the measurements of intraocular pressure (IOP) and central corneal thickness (CCT), and are recognized as important factors in the susceptibility to development of glaucomatous damage.345 In addition, corneal biomechanical properties could be useful for not only the detection of corneal diseases, but also the prediction of refractive outcomes following corneal refractive surgery.67
Until recently, the only instrument that allowed in vivo measurement of ocular biomechanical properties was the ocular response analyzer (ORA, Reichert Ophthalmic Instruments, Depew, NY, USA).8 ORA has been used for the assessment of corneal biomechanical properties according to the dynamic bidirectional applanation process.8 Using ORA, several authors have compared the pre and postoperative corneal biomechanical parameters.910 In addition, a database of normal values for biomechanical properties of the healthy cornea that were measured using ORA has been developed based on the results of previous studies.811
Dynamic Scheimpflug analyzer [corneal visualization Scheimpflug technology (Corvis ST), Oculus, Wetzlar, Germany] has shown to be an appropriate instrument for the evaluation of corneal biomechanical properties.12 With the aid of an ultra-high-speed Scheimpflug camera, dynamic Scheimpflug analyzer enables direct visualization of corneal movement upon application of a rapid air-puff. Consequently, it is now possible to measure several corneal biomechanical parameters during corneal deformation caused by the application of air puff. Dynamic Scheimpflug analyzer provided several corneal biomechanical parameters, including applanation time (AT), applanation length (AL), corneal velocity (CV), deformation amplitude, peak distance, radius, maximal concave power, CCT, and IOP. Recent studies have evaluated the changes in corneal biomechanics following refractive surgeries such as photorefractive keratectomy, laser in situ keratomileusis,13 small-incision lenticule extraction, and corneal cross-linking.1415
Although a few studies have been conducted on the distribution of corneal biomechanical parameters using dynamic Scheimpflug analyzer in healthy eye, no study composed of subjects from a single ethnic group has been introduced yet.161718 Therefore, in the present study, we aimed to investigate biomechanical properties of the cornea using dynamic Scheimpflug analyzer according to age in healthy Korean participants.
Go to : 
MATERIALS AND METHODS
This prospective, cross-sectional, observational study followed the principles of the Declaration of Helsinki. Informed consent was obtained from all of the participants after explaining the purpose and possible consequences of the study. Ethics approval was prospectively obtained by the Institutional Review Board of Yonsei University College of Medicine, Seoul, Korea (4-2015-0943). This study is registered at http://www.clinicaltrials.gov (identification no. NCT02627170).
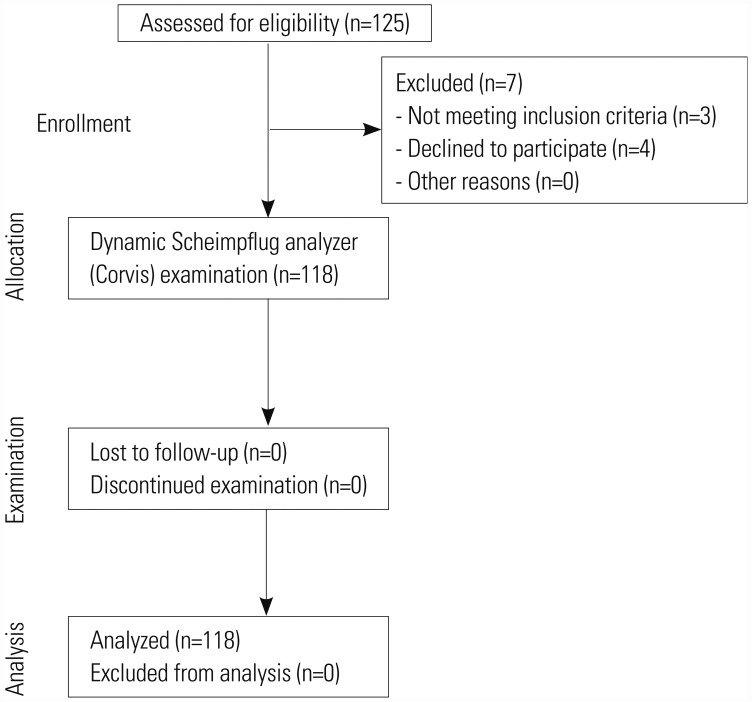
A total of 217 normal eyes of 118 healthy participants were enrolled between December 2, 2015, and March 1, 2016 (Fig. 1). Only participants of ages >20 years were included. The participants underwent thorough ophthalmic investigation, including evaluation of the corrected distance visual acuity and manifest refraction spherical equivalent (MRSE), assessment of the corneal biomechanical properties using dynamic Scheimpflug analyzer, and determination of IOP by non-contact tonometry (NCT; NT-530, Nidek Co., Ltd., Aichi, Japan) and keratometric values by autokeratometry (ARK-530A, Nidek Co., Ltd.). Slit-lamp biomicroscopic evaluation (Haag-Streit, Gartenstadtstrasse, Köniz, Switzerland) of the anterior segment and retina were also conducted.
Exclusion criteria for the study were the presence of abnormal ocular findings except for clinically insignificant senile cataract according to the Lens Opacities Classification System III method,19 history of ocular or intraocular surgery, history of ocular diseases such as glaucoma or age-related macular degeneration, presence of corneal abnormalities such as keratoconus and forme fruste keratoconus, or corneal scarring that would preclude the accurate measurement of ocular characteristics. Signs of keratoconus on Scheimpflug tomography were displacement of the corneal apex, decrease in the thinnest point pachymetry, and asymmetric topographic pattern. Participants with diabetes mellitus were excluded in order to exclude any possible effects of the disease on corneal hysteresis.2021 Participants were confirmed as not using eye drops, especially anti-IOP agents, which can cause variations in the corneal biomechanical properties.22
The principles of dynamic Scheimpflug analyzer have been described in detail elsewhere.23 Briefly, dynamic Scheimpflug analyzer captures the dynamic process of corneal deformation caused by air puff using an ultra-high-speed Scheimpflug camera, which acquires up to 4330 images per second.24 In the present study, AL and CV were automatically calculated by dynamic Scheimpflug analyzer during three distinct phases—first applanation (when the cornea is moving inwards), highest concavity (depression of the cornea to highest concavity), and second applanation (when the cornea moves outwards during recovery from highest concavity).24 AL1 and AL2 were defined as the lengths of flattened cornea (mm) at first and second applanations, respectively. CV1 and CV2 were defined as the maximum corneal velocities during first and second applanation phases. Corneal deformation amplitude, peak distance, radius, maximal concave power, and CCT were also calculated. Deformation amplitude, which reflects corneal stiffness, was defined as the maximum amplitude when the cornea was flattened to its greatest curvature by air puff; thus, thinner corneas tend to exhibit higher deformation amplitudes compared to those of thicker corneas.25 Peak distance was defined as the distance between the two apexes at the time of highest concavity. Radius values were considered to represent the central concave curvature at highest concavity. Maximal concave power value was defined as the inverse radius of curvature at highest concavity. Dynamic Scheimpflug analyzer was also used to evaluate IOP (Corvis-IOP), which was calculated based on the timing of first applanation. All measurements were performed by the same investigator to eliminate possible inter-observer variability, and taken at approximately the same time of day. Each measurement was performed three times, and average value was used in the analysis.
Statistical analysis
Kolmogorov-Smirnov test was used to assess the normality of distribution of corneal biomechanical parameters. Piecewise regression models were used to determine the relationship between each corneal biomechanical parameter and ocular/systemic variables (participant's age, MRSE, IOP, and mean keratometric values).2627 Spearman correlation analysis and stepwise multiple regression analysis were performed to investigate the association between corneal biomechanical parameters and variables. Reference intervals (RI) were calculated by bootstrap method, in order to establish the normal ranges of various biomechanical parameters. This is known to be a good method for the representation of estimated distributions of reference data acquired from healthy populations.2829 The process for establishing RIs includes identifying and eliminating outliers, determining whether the distribution of reference data is Gaussian or non-Gaussian, and, then, establishing the confidence interval (CI) based on sample size and distribution of data. Values exceeding the interquartile (IQ) boundaries set at Q1 (first quartile of the distribution) – 1.5×interquartile range (IQR) and Q3 (third quartile of the distribution) + 1.5×IQR were rejected. IQR represents the range of data from first (Q1; 25th percentile) to third (Q3; 75th percentile) quartiles of distribution (IQR=Q3–Q1). Nonparametric methods of evaluation of CI, such as bootstrap method, were used since not all biomechanical parameters exhibited Gaussian data distribution. Statistical analysis was performed using R statistical software version 3.1.2 (R Foundation for Statistical Computing, Vienna, Austria) and Statistical Analysis System (SAS) software (version 9.2; SAS Institute, Inc, Cary, NC, USA). Differences were considered statistically significant when p values were less than 0.05.
Go to :
RESULTS
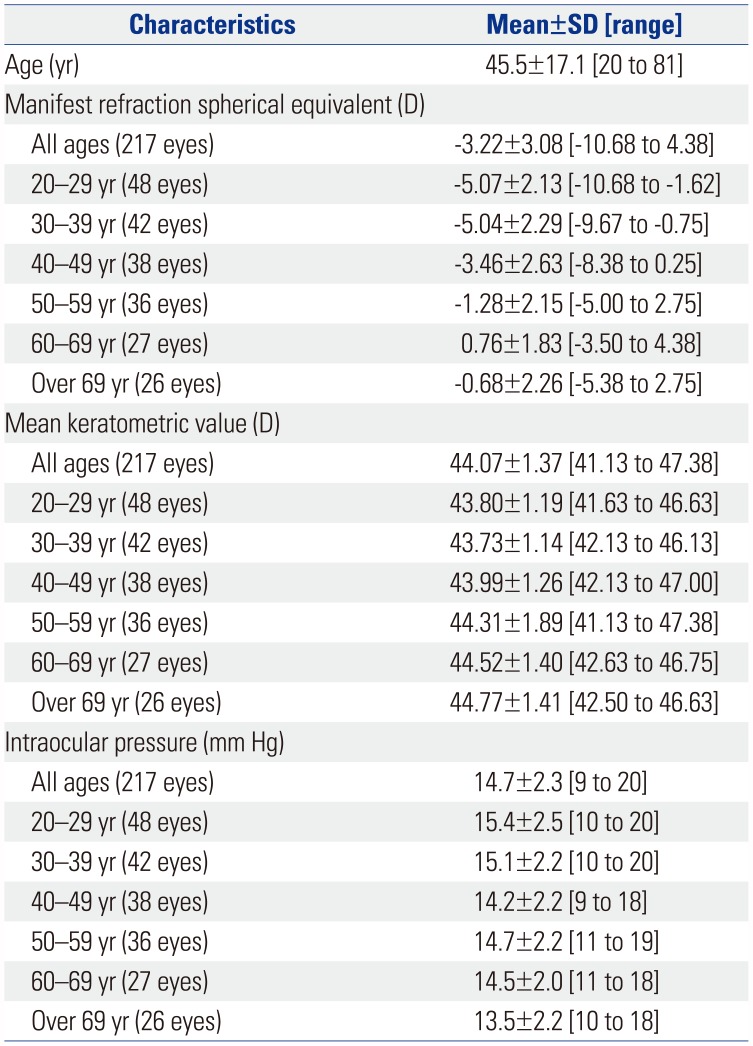
Table 1 presents the characteristics of study participants. According to the results of piecewise linear regression analysis, estimated breakpoint between Corvis-CCT and age was 45 years of age, as evident from the locally weighted scatterplot smoothing plot (Fig. 2A) and PROC NLIN module (FFig. 2B). Slopes of linear fit to reference data below and above the estimated breakpoint were −0.760 and 0.624, respectively. According to subgroup analysis, there were significant differences in AL1, CV1, Corvis-CCT, and deformation amplitude between the age groups of 20–44 years and above 44 years (p<0.001 for AL1, CV1, and deformation amplitude and p=0.041 for Corvis-CCT).
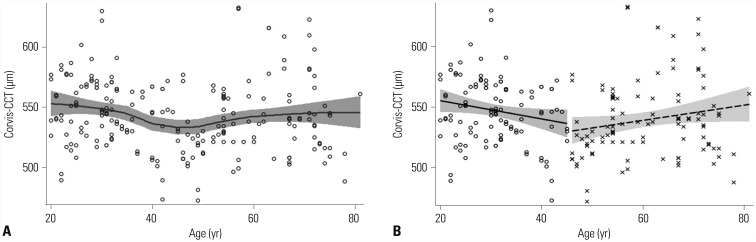 | Fig. 2Piecewise linear regression of Corvis-central corneal thickness (CCT) with participant's age. (A) Locally weighted scatterplot smoothing fit between Corvis-CCT and age. Estimated breakpoint between Corvis-CCT and age is 45 years of age. (B) Fitting of the model. Colored range: 95% confidence limits.
|
Table 1
Characteristics of Eyes in the Present Study
![]()
Table 2 summarizes the results of Spearman's correlation analysis after considering the cut-off value of age (45 years). AL1, CV1, AL2, deformation amplitude, Corvis-CCT, and Corvis-IOP of all age group exhibited significant correlations with participant's age. CV1, deformation amplitude, and Corvis-IOP of the age group of 20–44 years, as well as deformation amplitude and Corvis-CCT of the age group of over 44 years exhibited correlations with participant's age. AL1, AL2, CV2, deformation amplitude, Corvis-CCT, and Corvis-IOP of all age group exhibited correlations with MRSE. CV1, CV2, deformation amplitude, peak distance, radius, maximal concave power, Corvis-CCT, and Corvis-IOP of all age group exhibited significant correlations with IOP. CV1, AL2, CV2, deformation amplitude, peak distance, radius, maximal concave power, Corvis-CCT, and Corvis-IOP of the age group of 20–44 years, as well as CV1, CV2, deformation amplitude, radius, maximal concave power, Corvis-CCT, and Corvis-IOP of the age group of over 44 years were correlated with IOP. AL1, CV2, and deformation amplitude of all age group exhibited significant correlations with the mean keratometric values. According to the results of stepwise multivariate regression analysis, deformation amplitude was the most relevant variable (Table 3). With larger deformation amplitude, age became significantly increased while IOP decreased.
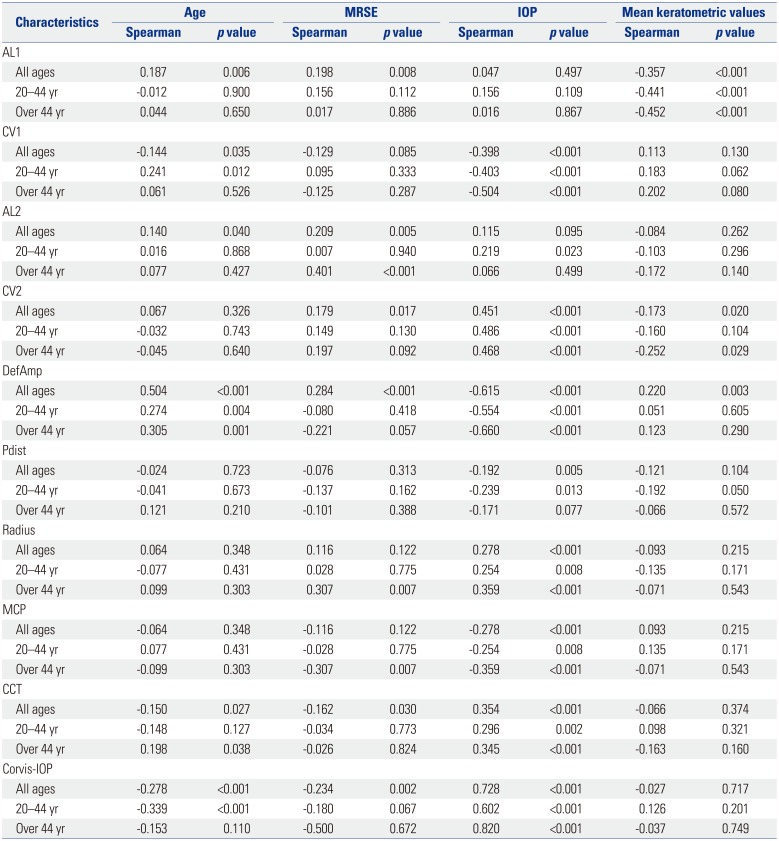
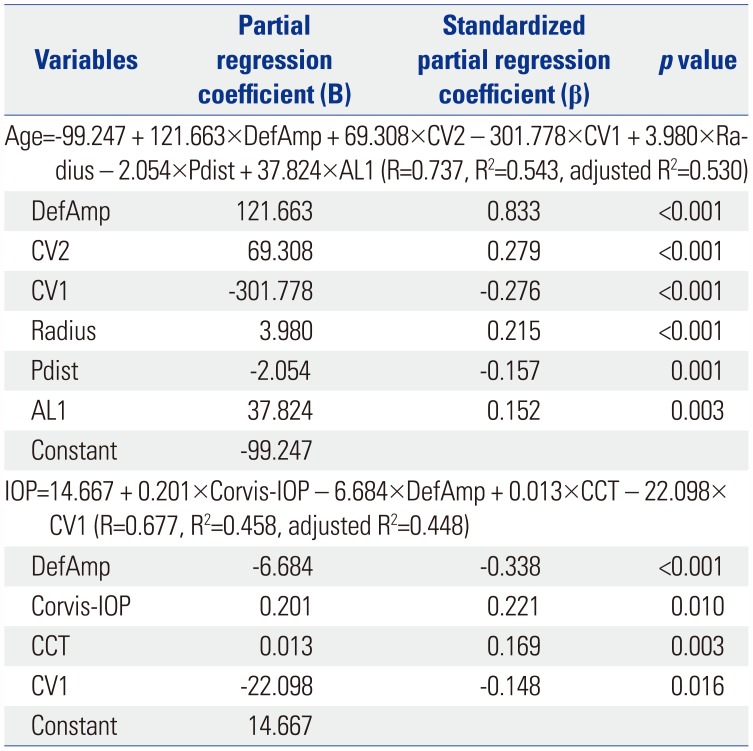
Table 2
Determination of Correlations between Corneal Biomechanical Parameters and Each of the Ocular/Systemic Variables (Participant's Age, MRSE, IOP, and Mean Keratometric Values) in Three Separate Age Groups by Spearman's Correlation Analysis
![]()
Table 3
Results of Stepwise Multiple Regression Analysis between Corneal Biomechanical Parameters and Participant's Age, and IOP
DefAmp, deformation amplitude; CV, corneal velocity; Pdist, peak distance; AL, applanation length; IOP, intraocular pressure; CCT, central corneal thickness.
Variables in the table are ordered according to the strength of contribution, which was based on standardized partial regression coefficient (β).
![]()
Table 4 presents the results of determination of CI using bootstrap method in three separate age groups—all ages, 20–44 years, and over 44 years. Table 5 presents the summary of reference data of corneal biomechanical parameters that were obtained after elimination of outliers from the data.
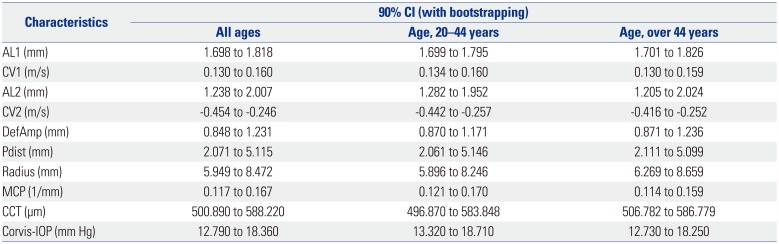
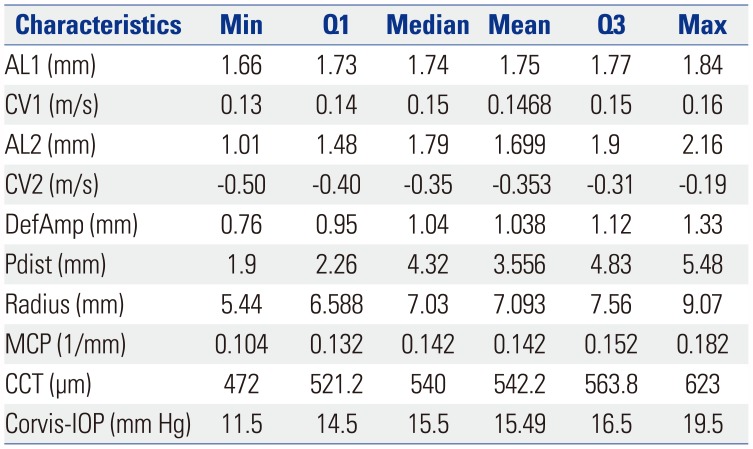
Table 4
Determination of CIs from the Reference Interval Data in Three Separate Age Groups Using Bootstrap Method
![]()
Table 5
Summary of Reference Data of Corneal Biomechanical Parameters
![]()
Go to :
DISCUSSION
In the present study, we investigated the biomechanical properties of the cornea using dynamic Scheimpflug analyzer in healthy adults according to age, and demonstrated the distribution of corneal biomechanical parameters after categorizing the data based on the cut-off value of age (45 years).
A recent study investigating the corneal biomechanical properties in 90 healthy Brazilian participants between the ages of 21.1 to 78.8 years, using dynamic Scheimpflug analyzer, reported the normal values of biomechanical parameters; the study also reported an association between CCT measured using Pentacam (Oculus) and the biomechanical parameters measured, using dynamic Scheimpflug analyzer.30 Upon comparison with the results of the present study, it was observed that the mean values of AL1, CV1, AL2, and radius reported in healthy Brazilian participants did not fall within the corresponding 90% CIs determined in our study. Other studies have reported the results of evaluation of corneal biomechanical properties in control groups comprising healthy participants; while one of these studies included 18 eyes of 10 young Chinese patients with myopia, another included 52 eyes of 26 young Hungarian patients with myopia and hyperopia.1424 The mean values of all corneal biomechanical parameters evaluated in those two studies were noted to fall within the corresponding 90% CIs for participants between the ages of 20 and 44 years in the present study. In another study including the corneal biomechanical properties of 32 young, healthy Danish participants, mean values of AL1, peak distance, and IOP did not fall within the corresponding 90% CIs for participants between the ages of 20 and 44 years in the present study.31 The discrepancies in results observed between the Brazilian and Danish studies could be related to small sample size, or ethnicity or age-related variations in corneal biomechanical properties.
Results of the present study are in agreement with those of recent studies, which reported that IOP is a fundamental property in the evaluation of corneal deformation response.3233 In our study, CV1, CV2, deformation amplitude, radius, maximal concave power, Corvis-CCT, and Corvis-IOP exhibited significant correlations with IOP, regardless age (all p<0.01). While IOP was positively correlated with CV2, radius, CCT, and Corvis-IOP, it exhibited negative correlations with CV1, deformation amplitude, and maximal concave power. With smaller deformation amplitude and CV1 and higher Corvis-IOP, and thicker cornea, IOP became significantly increased. Considering that stretching of the cornea under conditions of high IOP might result in corneal stiffness, higher IOP might be associated with increased radius and decreased deformation amplitude or maximal concave power. In addition, considering that thinner corneas are associated with higher deformation amplitudes when compared to thicker corneas, there could be close relationships among thicker cornea, higher IOP, and more strengthened or stiff cornea. Interestingly, IOP was negatively correlated with CV1 (negative coefficient) and positively correlated with CV2 (positive coefficient). This implies that, although IOP level does not affect the length of first (inward) and second (outward) applanations, inward applanation is slower at high IOP, while outward applanation is quicker. We can speculate that the more stiff cornea, the faster recovery of cornea into pre-applanation state. Results of the present study are in accordance with those reported by Asaoka, et al.33 In a study on the evaluation of corneal biomechanical parameters using ORA, Narayanaswamy, et al.11 suggested that the disruption of equilibrium in the relationship among CH, CRF, and IOP might play a role in the increased susceptibility of an individual to glaucoma. Further research using dynamic Scheimpflug analyzer is required for establishing the significance of correlations among IOP, radius, deformation amplitude, and maximal concave power in order to identify the risk factors for development of glaucoma.
Participant's age exhibited significant correlations with several corneal biomechanical parameters. Specifically, in the present study, participant's age exhibited a significant positive correlation with deformation amplitude, regardless of age group (all p<0.01). Therefore, we suggest that corneal stiffness would be lower in old-aged participants compared to young-aged participants. In case of Corvis-CCT, participant's age exhibited negative correlations with Corvis-CCT. However, Corvis-CCT of the age group of over 44 years exhibited positive correlations with participant's age. Also, there were significant differences in Corvis-CCT between the age groups of 20–44 years and above 44 years (p=0.041). We confirmed these differences by piecewise regression analysis between Corvis-CCT and participant's age, the results of which demonstrated the estimated breakpoint between CCT and participant's age to be 45 years of age. Additionally, slopes of linear fit to reference data below and above 45 years of age were −0.760 vs. 0.624, showing different directionality.
According to results of stepwise multiple regression analysis, age increased with larger deformation amplitude, CV2, radius, and AL1, as well as with smaller CV1 and peak distance. Therefore, when determining age-related effects on corneal biomechanical parameters using dynamic Scheimpflug analyzer, analysis based on multiple corneal biomechanical parameters is mandatory. Several studies have reported a decrease in CH and CRF, measured using ORA, with an increase in age.1134 Results of experimental ex vivo studies have demonstrated an increase in corneal stromal collagen cross-linking with age, which, consequently, results in a decrease in corneal viscosity and an increase in corneal stiffness.353637 On the other hand, one previous study reported no significant association between patient's age and CRF.38
Results of the present study also demonstrated that mean keratometric values were correlated with AL1 regardless of age (all p<0.001). According to previous studies, the associations between corneal radius of curvature and corneal biomechanical parameters measured by ORA were unclear.113940
Finally, we determined the CIs for reference data on the basis of RIs. Considering that this is a good method for representing the estimated distributions of reference data from healthy populations, our results of determination of CI from the data of RI could be valuable for further study on biomechanical properties of the cornea in healthy eyes.
The strength of our study lies in the fact that our study sample was composed of subjects from a single ethnic group, without ocular pathologies or history of ocular surgery. However, the cross-sectional nature of our study limits our ability to arrive at causal conclusions. Further large population-based studies investigating the correlation of corneal biomechanical properties with various ocular/systemic variables are required. In addition, definite cut-off values should be calculated by piecewise linear regression analysis between corneal biomechanical properties and multiple variables in specific corneal diseases, such as keratoconus and corneal ectasia.
In conclusion, we have investigated biomechanical properties of the cornea in healthy adults according to age using dynamic Scheimpflug analyzer. Our results have demonstrated that corneal biomechanical parameters are significantly influenced by IOP. Therefore, when interpreting corneal biomechanical parameters obtained from dynamic Scheimpflug analyzer, clinicians should consider age-related and IOP-related effects on values for corneal biomechanical parameters.
Go to :
 XML Download
XML Download