

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
According to the Causes of Death Statistics of Korea, published in 2016, deaths related to cancer accounted for 27.8% of the total mortality rate, which was the highest among the 10 leading causes of death. The number of cancer cases and deaths has been steadily increasing every year, with the cancer death rate increasing by 1.4% in the previous year.1 Pancreatobiliary cancer is one of the 10 most common cancers in Korea, accounting for 2.7% of all cancer cases in 2014. In contrast to the improving survival rates for major cancers, including stomach and breast cancers, the survival rate for pancreatobiliary cancer has shown minimal increases, and the 5-year survival rate remains less than 10%.2
Pancreatobiliary cancer shows poor prognosis, and many patients experience difficulty having a positive outlook toward treatment, which subsequently leads to serious psychological distress. Studies examining the prevalence of depression in cancer patients have shown that pancreatobiliary cancer is most highly associated with depression (33–50%), followed by oropharyngeal cancer (22–57%), lung cancer (11–44%), and breast cancer (1.4–46%), with the subjective quality of life (QoL) of the patients with pancreatobiliary cancer being the lowest.34 Due to such psychological distress, many patients with pancreatobiliary cancer experience anxiety and depression after being diagnosed, and develop a negative outlook on life. These patients are also less willing to undergo treatment and frequently discontinue curative treatment.5 Thus, a multidisciplinary approach that includes psychiatric care in addition to cancer therapy is essential for the treatment of patients with pancreatobiliary cancer.
In recent years, a number of studies have focused on the psychological aspects of patients with advanced cancer and have reported the importance of a patient's sense of meaning in life and spiritual well-being. Accordingly, the need for psychological care through psychiatric intervention is being increasingly acknowledged.67 Due to serious psychological distress, patients with advanced cancer experience a number of psychological symptoms, including depression, anxiety, insomnia, anhedonia, and personal devaluation, and some patients even experience a loss of meaning of life and a desire for hastened death.89 One of the psychotherapeutic interventions for patients with advanced cancer is meaning-centered psychotherapy (MCP). It was first conceptualized by Viktor E. Frankl and has been further developed by a number of other researchers for use in individual or group psychotherapy;1011 MCP has been shown to help patients increase a sense of meaning in one's life during distressing conditions and provide hope to patients with cancer even if they are not cured. Studies have shown that MCP is effective in enhancing QoL and spiritual well-being, as well as reducing depression and desire for death in patients with advanced cancer.1213 The present study aimed to investigate the effectiveness of MCP for patients with pancreatobiliary cancer who reported clinically significant psychological distress.
MATERIALS AND METHODS
Recruitment of study participants and ethics approval
A total of 37 patients with pancreatobiliary cancer were recruited from outpatient clinics at three university general hospitals from December 2015 to October 2017: Gangnam Severance Hospital, Yonsei University College of Medicine; Yeungnam University College of Medicine; and Konyang University College of Medicine. The recruited patients (aged ≥20 years) were scheduled to undergo surgery or receive treatment after being diagnosed with pancreatobiliary cancer. The patients did not exhibit cognitive impairment, understood the purpose of the study, and provided consent to participate in the study. For initial assessment, self-report questionnaires were administered to the patients by registered nurses at each of the three hospitals. Based on the initial assessment, patients who met one of the following criteria were recommended to participate in MCP: 1) a score of 8 or higher on both the anxiety and depression subscales of the Hospital Anxiety and Depression Scale (HADS), 2) a score of 4 or more on the distress thermometer, or 3) a score of 18 or more in the helpless-hopeless subscale of the Mini-Mental Adjustment to Cancer Scale (MAC). MCP was provided to the patients who met the above criteria and wished to participate in this study. Patients who refused to participate in MCP or did not meet the inclusion criteria for MCP group were assigned to the non-MCP group. The questionnaires were administered again 2 months after completing MCP during a follow-up evaluation of the patients' psychological characteristics. Demographic data of the patients were collected during the initial assessment, and electronic medical records were used to examine the patients' medical data, including pancreatobiliary cancer stages. This study was reviewed and approved by the Institutional Review Boards of the Gangnam Severance Hospital (Approval No. 3-2015-0269) including all participating institutions.
Meaning-centered psychotherapy
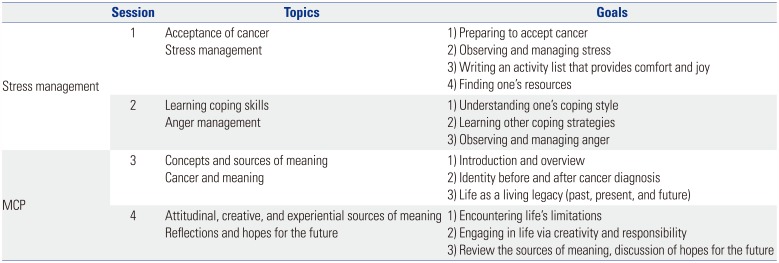
A psychiatrist or a clinical psychologist who had received training in MCP conducted the MCP sessions. The patients in the present study received MCP individually because scheduling for a group intervention was often difficult due to the patients' health conditions and cancer therapy schedules. All patients underwent surgery before the start of MCP and received MCP during chemotherapy, except for one patient who had not received any other treatment after surgery. Most patients received MCP on the day of their outpatient visit, and each patient participated in four sessions of MCP. The content of the sessions was divided into stress management and MCP. The sessions addressed the topics of accepting cancer and stress management, reviewing the concept of meaning of life and rediscovering it despite the limitations related to cancer (Table 1). Each session lasted approximately 1 hour. At the end of each session, the patients were provided related reading material or homework and were instructed to read or try them before the next session.
Assessment scales
The following assessment scales were used in the study: the HADS, for the assessment of depression and anxiety;14 the MAC, for the assessment of psychological and behavioral responses to cancer;15 the European Organization for Research and Treatment of Cancer (EORTC) quality of life questionnaire core 30 (QLQ-C30), for the assessment of global quality of life; the EORTC pancreatic cancer-specific module (QLQ-PAN26), for the assessment of QoL specific to patients with pancreatobiliary cancer;1617 and Social Readjustment Rating Scale (SRRS), for the quantification of psychosocial adjustments to assess personal stress levels from various stressors.18 The National Comprehensive Cancer Network distress thermometer (DS-DT) was included in the initial assessment to evaluate the patients' gross distress levels.19 The MAC used in this study is a minimized version of the widely used Mental Adjustment to Cancer scale. It contains 29 items using a four-point Likert scale, which includes the following five adjustment styles: fighting spirit (FS), helpless-hopeless (HH), anxious preoccupation (AP), fatalism (FA), and cognitive avoidance (CA). According to previous studies on standardization of the Korean version of MAC, FA and FS are associated with positive attitudes, while others are associated with negative attitudes. The QLQ-C30 and QLQ-PAN26 comprise 30 and 26 items, respectively. In the present study, the functional scales [physical function (PF), role function (RF), cognitive function (CF), emotional function (EF), social function (SF)] and QoL scale were assessed using the QLQ-C30. Symptom scales (pancreatic pain, digestive, altered bowel habit, body image, satisfaction with health care, and sexual functioning) were assessed using the QLQ-PAN26. The QoL scale employs a seven-point linear scale, with scores ranging from 1 to 7, and the other items are evaluated on a four-point Likert scale. The raw scores for each item were transformed to scores ranging from 0 to 100 according to the EORTC Scoring guidebook.20 Higher scores in the functional scales and QoL scale indicate better QoL, while lower scores in the symptoms scales indicate better QoL.
Statistical analysis
The sociodemographic characteristics and questionnaire scores for psychiatric assessment of the MCP and non-MCP groups were analyzed. The Kolmogorov-Smirnov test was used to test for normality, and Fisher's exact test and Mann-Whitney U test were used to assess homogeneity between the groups. Paired t-test and Wilcoxon signed rank test were used to compare the questionnaire scores at the initial and follow-up assessments of the MCP and non-MCP groups. Changes in scores were analyzed using independent t-test and Mann-Whitney test. Analysis of covariance (ANCOVA) was conducted to statistically control for differences in initial assessment scores between the MCP and non-MCP groups for more accurate analysis. All statistical tests were two-tailed, and p values less than 0.05 were considered statistically significant. All data were analyzed using SPSS ver. 22.0 (IBM Corp., Armonk, NY, USA).
RESULTS
General characteristics and initial assessments
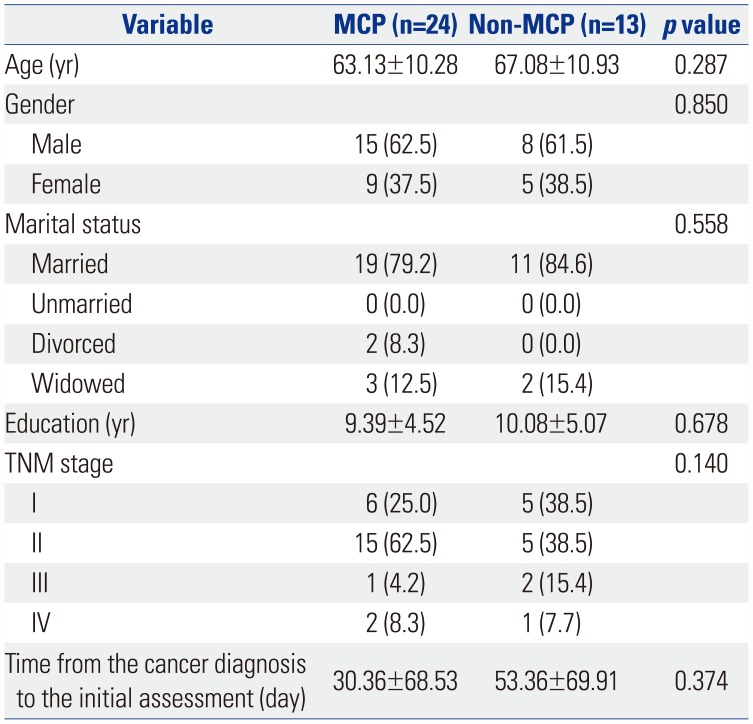
Of the 37 patients who completed the initial assessment, 24 received MCP (Table 2). The mean ages of the MCP (63.13±10.28 years) and non-MCP (67.08±10.93 years) groups were not significantly different (p=0.287). In the MCP group, 15 (62.5%) patients were men and nine (37.5%) were women. The proportion of married individuals was high (79.2%). The mean years of education in the MCP group was 9.39 (±4.52) years. The number of patients with tumor, node, metastasis (TNM) stages I and II was higher than the number of patients with TNM stages III and IV for both groups. The time from the cancer diagnosis to the initial assessment was 30.36 (±68.53) days in the MCP group and 53.36 (±69.91) days in the non-MCP group, which were not significantly different (p=0.374). Among the patients, two in the non-MCP group were receiving psychiatric medication, SSRI and mood stabilizer with antipsychotics, respectively.
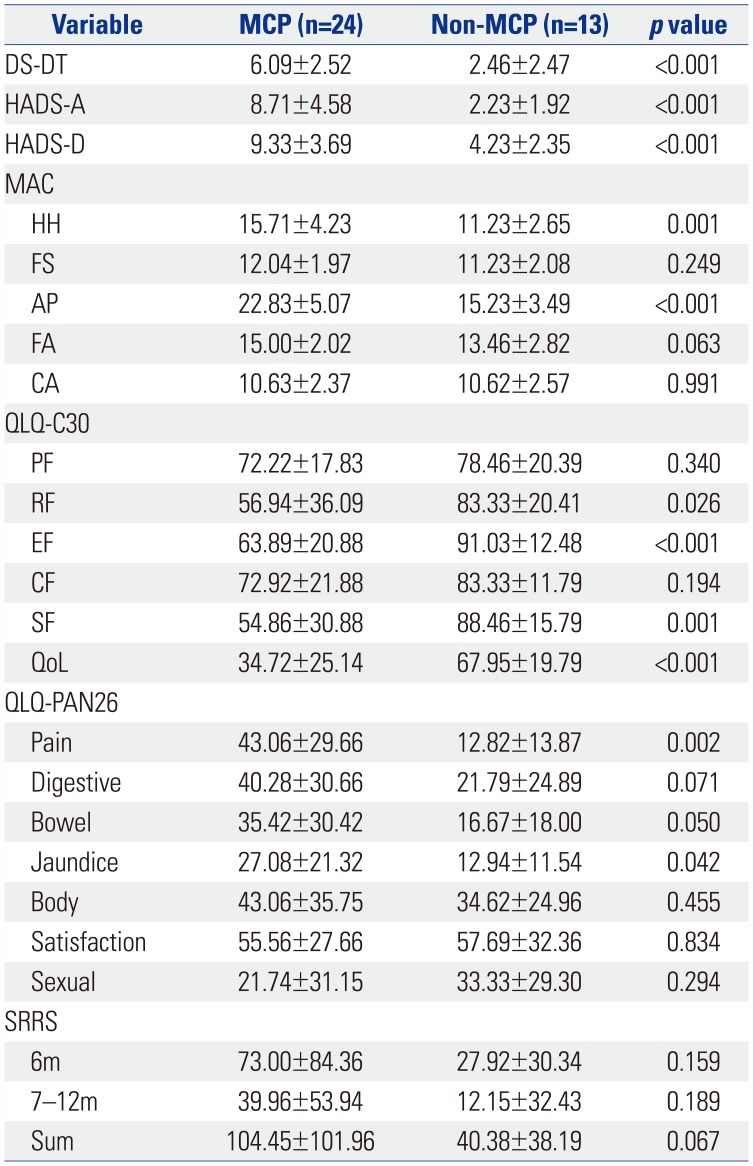
In the initial assessment, the patients in the MCP group showed significantly higher levels of distress (DS-DT, p<0.001), anxiety (HAD-A, p<0.001), and depression (HAD-D, p<0.001) than those in the non-MCP group. The scores of helpless-hopeless (MAC-HH, p=0.001) and anxious preoccupation (MAC-AP, p<0.001) items of the MAC scale were also significantly higher in the MCP group than in the non-MCP group. Moreover, the patients in the MCP group, in general, scored lower on the social and emotional functional scales of the QLQ-C30, and the overall QoL scale scores were significantly different between the two groups (p<0.001) (Table 3).
Effectiveness of MCP
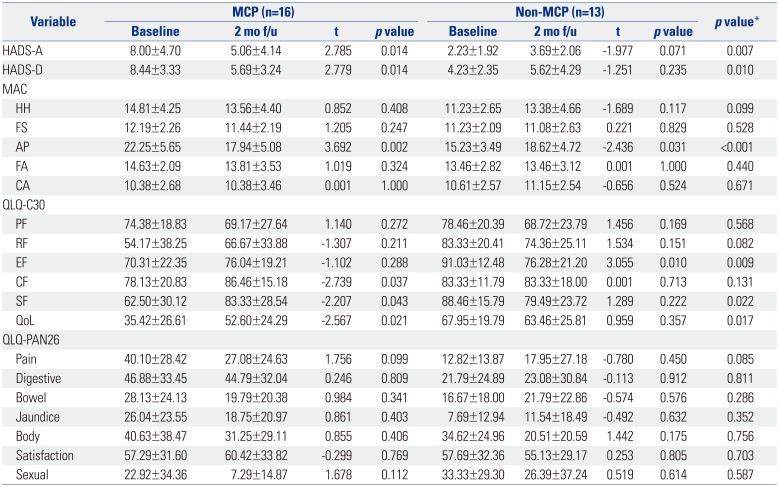
Of the 24 patients who received MCP, 16 completed the questionnaire during the follow-up 2 months after the completion of MCP. Thirteen patients in the non-MCP group completed the questionnaire again 2 months after the initial assessment (Table 4). The patients in the MCP group showed significant improvements in the HADS-A (p=0.014), HADS-D (p=0.014), and MAC-AP (p=0.002) scores at the final assessment. In addition, cognitive function (QLQ-C30-CF, p=0.037), social function (QLQ-C30-SF, p=0.043), and global QoL (QLQ-C30-QoL, p=0.021) for patients in the MCP group were also significantly improved at the final assessment. Although there were no clinically significant changes in the scores between the initial and final assessments for the non-MCP group, a trend of increasing distress was observed, based on the MAC-AP (p=0.031) and emotional function (QLQ-C30-EF, p=0.010) scores.
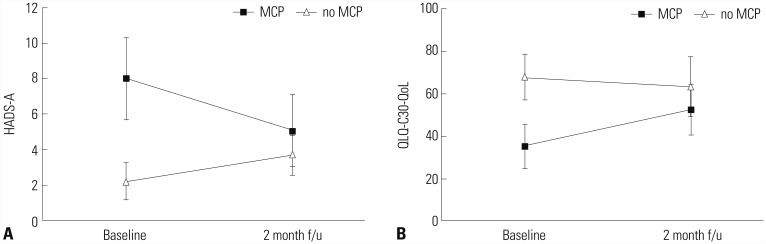
Changes in HADS-A (p=0.007) and HADS-D (p=0.010) scores between the initial and final assessments were significantly different between the MCP and non-MCP groups. Changes in MAC-AP score were also significantly different between the two groups (p<0.001). Moreover, the two groups showed significantly different changes in the scores for EF (p=0.009), SF (p=0.022), and global QoL (p=0.017) subscales of the QLQ-C30 (Fig. 1).
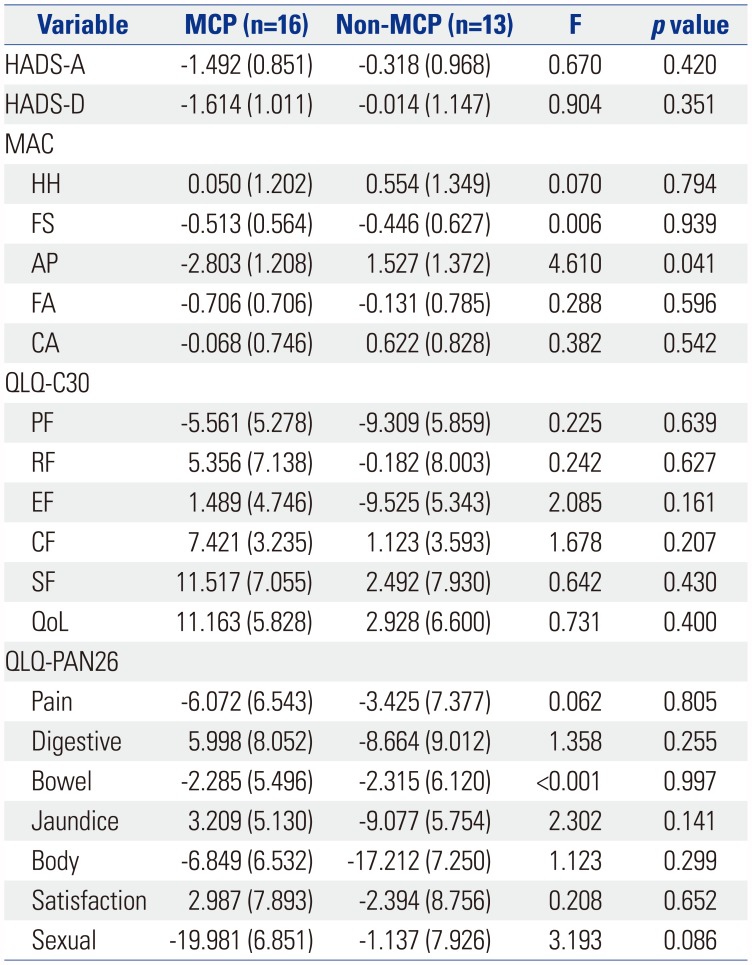
As the patients who received MCP scored significantly higher on several items assessing emotional distress and lower QoL at the initial assessment, the effects of these differences in the initial assessment were considered to affect the analysis of the therapeutic effect of MCP. In order to control for this, ANCOVA was conducted with initial assessment scores of each scale showing a difference at baseline (e.g., HADS-A, HADS-D, HH, AP, RF, EF, SF, QoL, Pain, Jaundice) as the covariate of each scale to analyze changes in scores between the initial and follow-up assessments of the two groups (Table 5). FS, FA of MAC and all items of QLQ-C30 suggest improvement when showing positive changes, whereas HADS-A, HADS-D, HH, AP, CA of MAC, and all items of QLQ-PAN26 reflect improvement when showing negative changes. This analysis showed that change in the anxious preoccupation (MAC-AP, p=0.041) subscale of MAC alone was significantly different between the MCP and non-MCP groups. In other words, the anxious preoccupation tendency in the MCP group showed significant positive changes, compared with the non-MCP group, when the differences at the initial assessment were controlled.
DISCUSSION
Patients with cancer experience a number of psychiatric symptoms, including depression, anxiety, and insomnia, in addition to physical symptoms.21 Pancreatobiliary cancer is one of the malignancies with the worst prognosis, so there is an even greater need for a psychiatric approach for these patients.3 One of the psychotherapeutic intervention that helps patients cope with the distress is MCP. There have been no reports of MCP being conducted in patients with advanced cancer in Korea. Thus, the present study aimed to evaluate the effectiveness and applicability of MCP in patients with pancreatobiliary cancer.
We examined emotional distress and QoL before MCP and 2 months after its completion. The MCP group showed significant improvements in depression, anxiety, and anxious preoccupation related to mental adjustment to cancer, global QoL, cognitive function, and social function, although the group had scored relatively poorly for emotional distress and QoL at the initial assessment. In contrast, no clinically significant changes in emotional distress and QoL were found between the initial and follow-up assessments in the non-MCP group. Although not statistically significant, a trend of increasing distress, based on the MAC-AP and QLQ-C30-EF scores, was observed in the non-MCP group. These results suggest that patients with advanced cancer, who experience clinically significant emotional distress and decreasing QoL, need an appropriate psychosocial intervention. In addition, the MCP group showed significantly higher scores in the initial assessment of QLQ-PAN26 pain, jaundice. Higher anxiety and distress scores in the MCP group may be induced by severe physical symptoms. In addition, although not statistically significant, it is possible that MCP was assessed in severe physical symptoms because the time from cancer diagnosis to initial assessment was shorter than non-MCP. The important finding is that QLQ-PAN26, an evaluation item related to physical symptoms, did not show any significant improvement in any, while there was improvement in EF score. The results suggest that the therapeutic effects of MCP may primarily involve relieving psychological symptoms, which can change the cognitive approach process and improve emotional state even if actual physical symptoms are similar.
MCP is a psychotherapeutic intervention that helps patients cope with distress by enhancing meaning of life and spiritual well-being. So far, few psychological interventions have been developed, with psychological care more often being focused on providing psychoeducational or supportive interventions.13 These interventions have rarely considered meaning of life and spiritual well-being an important issue. MCP is based on the writings of Viktor Frankl, a psychiatrist and holocaust survivor, and he suggested that people desire to find meaning in their existence even as they approach the end of life.112223 This difference in the perspective of psychological care for cancer patients may cause MCP to be effective in patients with advanced cancer experiencing anxiety and pain related to the issue of “impending death.”1213
The result of ANCOVA for assessing MCP effectiveness showed that only MAC-AP was significantly improved in patients after receiving MCP. MAC-AP is characterized by constant preoccupation with cancer and feelings of anxiety, fear, and devastation.24 Previous studies have shown that a higher score on AP domain was associated with both anxiety and depression, and has a negative impact on well-being, irrespective of phase of illness.2526 In this study, we attempted not only to get a meaning of life from different perspectives through MCP, but also to understand the causes of anxiety and to learn how to control anxiety effectively through stress management. These attempts seem to have worked together to improve cancer-related anxiety. Other variables, except MAC-AP, did not show a significant difference in ANCOVA. This may be attributed to the fact that only the patients who reported clinically significant distress in the initial assessment were selected for the MCP group.
Approximately 66% of the participants completed all sessions of MCP, which is much higher than the completion rate of the grouped format of MCP reported by previous studies.13 Generally, MCP is provided in a group format. In the present study, however, patients missed or were unable to complete their sessions due to difficulties of scheduling or illness-related problems. This suggests the need for a more flexible and personalized therapy for patients with advanced cancer. In our study, MCP was provided individually, and in many cases, patients were able to receive MCP after their outpatient visit to the surgery department. It is expected that this form of therapy will have positive effects on treatment compliance in clinical practice. A previous study on MCP, however, showed that patients who received the individual format of MCP no longer showed improvement 2 months after its completion, whereas patients who received the grouped format showed continued improvement when they were followed up after more than 2 months.12 Our study demonstrated the effectiveness of MCP up to 2 months after its completion, and further investigation in a long-term follow-up study may provide a better understanding of the patterns of MCP effectiveness.
This study has several limitations. Firstly, the subjects were limited to patients with pancreatobiliary cancer, and the results may not be generalizable to all patients with cancer. Moreover, the small sample size of the MCP group lowers the statistical power. As mentioned above, ANCOVA showed significant therapeutic effect in terms of MAC-AP scores alone, whereas the t-test showed otherwise. More statistically significant results may be expected when larger sample sizes of MCP and control groups with clinically significant emotional distress are compared to assess therapeutic effects. In addition, although the patients of this study were recruited from three hospitals, the number of patients that the psychologists at each hospital were assigned to was not equal because different numbers of patients were recruited at each hospital. The therapist may influence the therapeutic effect and patient satisfaction. To minimize the effect related with differences between therapists, we initiated this study after each therapist had had sufficient time to discuss the MCP program during the study preparation step. The MCP group was reassessed two months after the completion of the MCP, while the non-MCP group was reassessed two months after the baseline. Therefore, there is a difference in the evaluation interval for each group, and these factors may have affected the outcome. Lastly, the MCP was only recommended to the patients who showed clinically significant levels of depression, anxiety, and distress in this study, and the results of the current study do not provide evidence for the effectiveness of MCP in patients without clinically significant psychiatric symptoms.
Despite these limitations, our study showed that MCP helps patients with advanced cancer regain their sense of meaning in life and may reduce emotional distress, including depression and anxiety, and increase QoL. Our study is the first to attempt MCP intervention in patients with pancreatobiliary cancer in Korea. The need to treat the psychiatric symptoms of patients with cancer is clear, and further studies and clinical trials may establish MCP as an important therapeutic tool for treating patients with advanced cancer.
 XML Download
XML Download