

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
With an increase in the incidence of transnational marriage, Korean society has moved rapidly toward becoming a multicultural society. According to statistics published by Statistics Korea in 2016, the number of female marriage immigrants gradually increased from 127540 in 2012 to 128518 in 2016 (http://index.go.kr/potal/main/EachDtlPageDetail.do?idx_cd=2819).1 The majority of transnational marriages in Korea takes place between Korean men and women from other Asian countries, where, with the exception of Japan, the prevalence of viral hepatitis is similar to or somewhat higher than that of Korea.23456
Hepatitis A virus (HAV) is usually transmitted via polluted water and contaminated food, and seroprevalence is dependent on age and level of hygiene.7 Especially, since one's first exposure to HAV during adulthood can lead to severe and fatal acute hepatitis, it is important to identify susceptible individuals, particularly women of childbearing age, who are likely to be female marriage immigrants.8910 It is possible that the prevalence of hepatitis B virus (HBV) in immigrants reflects infection patterns present in their own countries.1112 Although early and timely vaccinations for those at risk could prevent diseases caused by HAV and HBV, the seroprevalence of hepatitis viruses in multicultural families has not yet been investigated in real-life situations.
HBV strains have been classified into eight well-known genotypes (A–H), and two new genotypes, I and J, have recently been identified.1314 HBV genotypes are related to disease progression, clinical outcome, response to antiviral treatment, and prognosis.15 Therefore, determination of specific genotypes may be important in the clinical management of HBV infection. Geographic distributions of HBV genotypes are distinctive, and genotypes B and C are prevalent in the Asian-Pacific region.15 Genotype C is more common than genotype B in China and Japan, whereas the opposite is true in Taiwan and Vietnam.16 While almost all HBV strains have been identified as genotype C in Korea,1718 there is no available data concerning HBV genotypes in multicultural families.
The total global prevalence of anti-hepatitis C virus (HCV) is estimated to be 1.6%,19 which is higher than the prevalence in Korea (0.78%).20 Even if HCV prevalence may decrease in the near future due to oral antiviral agents, a better knowledge of the prevalence of anti-HCV positivity in female marriage immigrants may help physicians control and prevent HCV infection.
This study aimed to estimate the seroprevalence of hepatitis viruses and investigate HBV genotypic diversity in female marriage immigrants.
Go to : 
MATERIALS AND METHODS
Study population
Free screening program was conducted at support centers for multicultural families in 21 administrative districts in Korea (Gangdong-gu, Gangseo-gu, Geumcheon-gu, Guro-gu, Gwangjin-gu, Seongbuk-gu, and Yeongdeungpo-gu in Seoul; Anyang, Ansan, Icheon, Gunpo, Pyeongtaek, Gimpo, Gwangmyeong in Gyeonggi-do; Jangseong, Gokseong in Jeollanamdo; Bukgu, Sasanggu in Busan; Seosan in Chungcheongnamdo; Tongyeong in Gyeongsangnam-do; and Hongcheon in Gangwon-do). Nine hundred sixty three individuals in transnational marriages participated in the program between July 2011 and January 2017. Blood samples were tested for aminotransferase, IgG anti-HAV, HBsAg, anti-HBs, and anti-HCV. The following data were collected from all subjects: demographic information (e.g., age and sex), and original nationality. To study IgG anti-HAV seroprevalence according to age, patients were stratified into the following two age groups: 20–29 and 30–40 years. The study protocol conformed to ethical guidelines of the 1975 Declaration of Helsinki, and was approved by the Institutional Review Board of Chung-Ang University College of Medicine [IRB No. C2015178 (1636)]. In addition, written informed consent was obtained from each patient.
Definitions and laboratory tests
Anti-HAV seropositivity was established if serum IgG anti-HAV was positive, HBV infection was diagnosed if HBsAg was positive, and anti-HCV seropositivity was defined if serum anti-HCV was positive in a second-generation enzyme immunoassay. Commercially available enzyme immunoassay kits were used to detect serum IgG anti-HAV (bioMérieux SA, Marcy-l'Etoile, France) and anti-HCV (Roche, Mannheim, Germany). HBV serologic markers (HBsAg, anti-HBs) were tested via radioimmunoassay or enzyme-linked immunoassay, using commercial assays (Abbott Laboratories, Sligo, Ireland). HBeAg and anti-HBe were tested via radioimmunoassay or enzyme-linked immunoassay, using commercial assays (Abbott Laboratories).
Determination of HBV DNA titer and genotypes
Among 52 subjects who were HBsAg-positive, written informed consent on HBV DNA genotyping, HBeAg, and anti-HBe was obtained from 28 subjects. Among these 28 subjects, 22 subjects showed detectable HBV DNA levels and six subjects showed undetectable HBV DNA level. Serum HBV DNA concentration was determined by a commercially available quantitative assay (Lightcycler 2.0; Roche Diagnostics, Branchburg, NJ, USA). The lower limit of sensitivity of assay was 116 copies/mL. With respect to genotyping, a phylogenetic analysis based on entire sequences of the entire HBs region was performed for subjects with detectable HBV DNA (n=22). Nucleotide sequences of HBV strains were compared to those of reference strains representing genotypes B and C obtained from GenBank (Accession numbers AB010290.B1, AB073830. B2, AB73823.B2, M54923.B3, AY033072.B4, AB073835.B4, AB219429.B5, AY123041.C1, AY217371.C1, AB205124.C2, X756 56.C3, X75666.C3). A maximum likelihood phylogenetic tree was constructed using MEGA (version 5).
Statistics
Seroprevalence of hepatitis viruses was expressed as number of positive/number of tested subjects (percentage), according to country or region. In particular, seropositivity of IgG HAV was stratified according to age group, country, or region.
Go to :
RESULTS
Patient characteristics
Baseline characteristics of the subjects are shown in Table 1. A total of 963 female marriage immigrants were included in this study. They participated in the free hepatitis screening program conducted by Chung-Ang University Hospital between July 2011 and January 2017. Subjects' median age was 33 years (20–40), consisting of women from nine countries including Vietnam (n=422, 43.8%), China (n=311, 32.3%), the Philippines (n=85, 8.8%), Cambodia (n=58, 6.0%), Japan (n=39, 4.0%), Uzbekistan (n=18, 1.9%), Mongolia (n=13, 1.3%), Thailand (n=10, 1.0%), and Kazakhstan (n=7, 0.7%).
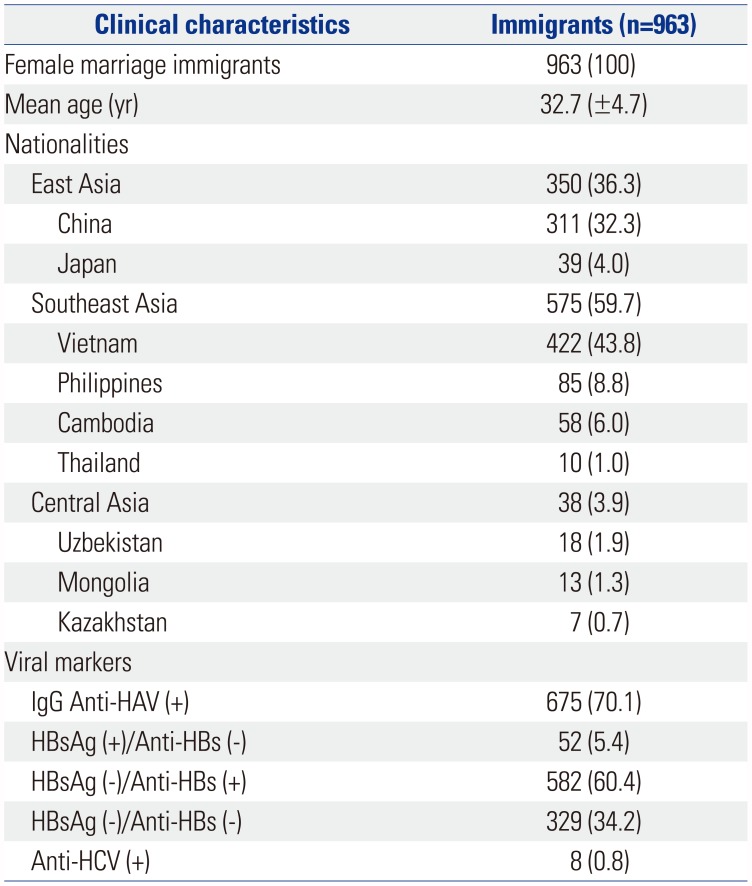
Table 1
Baseline Demographic and Clinical Characteristics
![]()
Seroprevalence of IgG anti-HAV according to age group
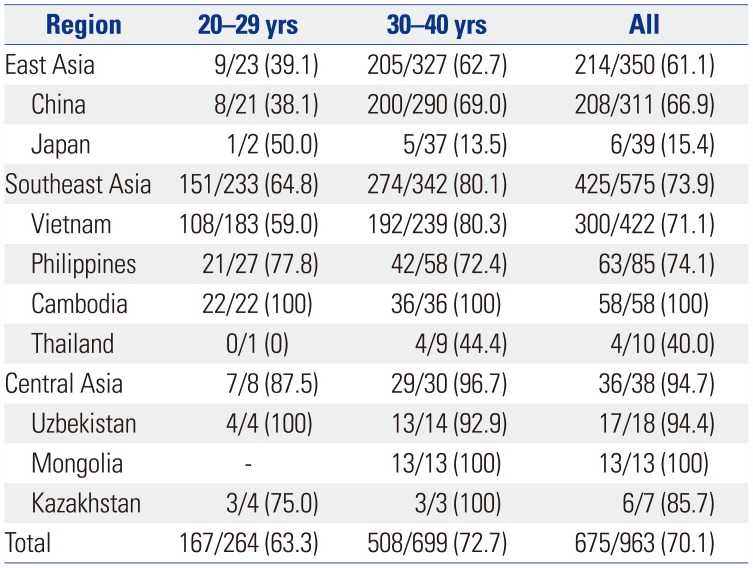
Of 963 subjects, 675 (70.1%) were positive for IgG anti-HAV and 288 (29.9%) required HAV vaccination. Seroprevalence of IgG anti-HAV according to country, region, and age is presented in Table 2. All 71 subjects from Cambodia and Mongolia were shown to be positive for IgG anti-HAV, and IgG anti-HAV was highly prevalent in subjects from Uzbekistan, Kazakhstan, the Philippines, Vietnam, and China. In contrast, only 15.4% (6 of 39) subjects from Japan showed positive for IgG anti-HAV. Seroprevalence of IgG anti-HAV increased with age. In subregions of Asia, IgG anti-HAV seroprevalence was high in members of multicultural families from Central, Southeast, and East Asia, except Japan (Fig. 1).
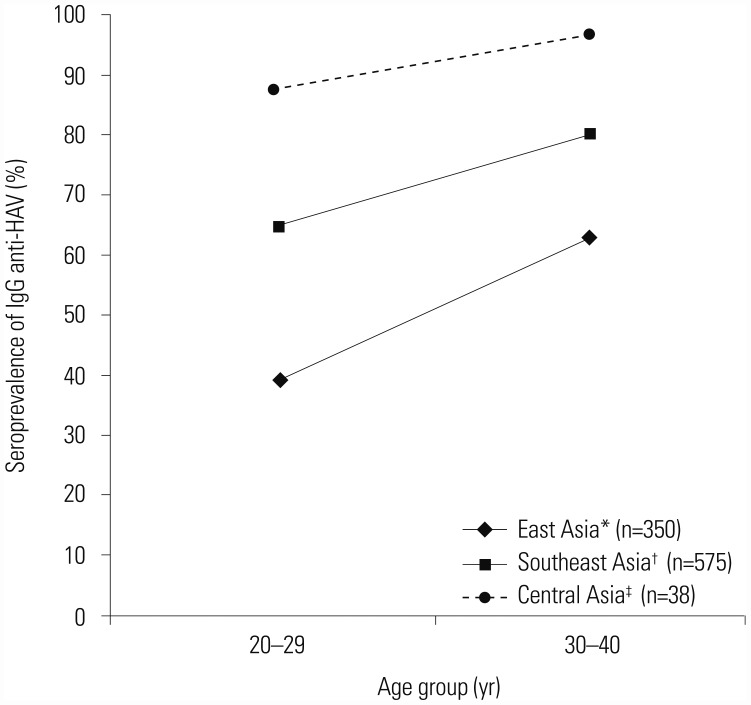 | Fig. 1Seroprevalence of IgG anti-HAV in female marriage immigrants according to subregion of Asia. Female marriage immigrants from Central Asia, Southeast Asia, and East Asia showed high seroprevalence of IgG anti-HAV. Seroprevalence of IgG anti-HAV increased with age. *East Asia: China (n=311) and Japan (n=39), †Southeast Asia: Vietnam (n=422), Philippines (n=85), Cambodia (n=58), and Thailand (n=10), ‡Central Asia: Uzbekistan (n=18), Kazakhstan (n=7), and Mongolia (n=13). HAV, hepatitis A virus.
|
Table 2
Seroprevalence of IgG Anti-HAV in Female Marriage Immigrants
![]()
Seroprevalence of hepatitis B virus
Overall, 52 (5.4%) subjects were positive for HBsAg. Rates of positive HBsAg were the highest in subjects from Vietnam (7.6%, n=32), followed by those from Cambodia (6.9%, n=4) and China (4.2%, n=13), among countries with more than 50 subjects (Table 3). Five hundred eighty-two (60.4%) subjects were positive for anti-HBs. In addition, 329 (34.2%) subjects who required HBV vaccination presented negative for anti-HBs and HBsAg.
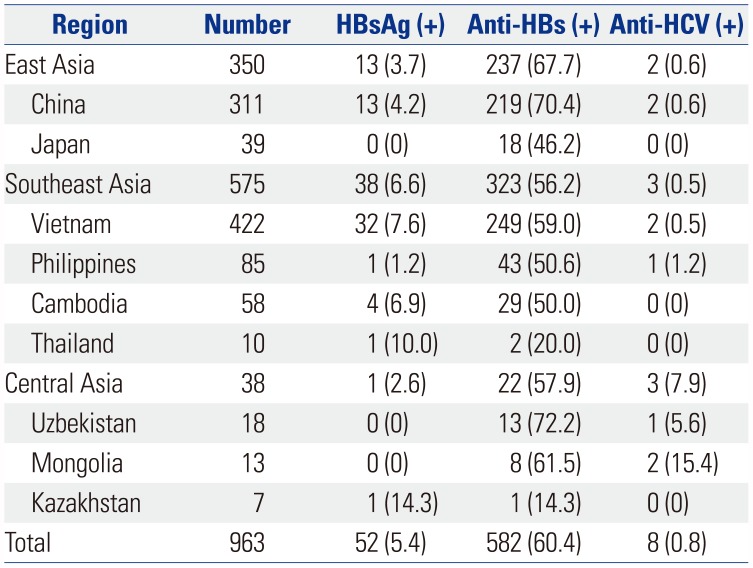
Table 3
Seroprevalence of HBV and HCV in Female Marriage Immigrants
![]()
HBV DNA levels and genotypes
Among the 52 HBV-infected subjects, blood samples were available for 28 subjects.
Nine subjects were positive for HBeAg; their mean age was 30 years (range: 25–36 years), and mean HBV DNA level was 636958527 copies/mL (120680–3472000000 copies/mL). Four subjects were categorized into immune tolerant phase [high HBV DNA levels (7560000–3472000000 copies/mL) and normal ALT (<40 IU/L)]. Five subjects were categorized into immune active phase [high HBV DNA levels (120680–752000000 copies/mL) and high ALT (>80 IU/L)], and required antiviral therapy.
Nineteen subjects presented negative for HBeAg; their mean age was 35 (range: 27–40), and mean HBV DNA level was 16323 copies/mL (<116–52432 copies/mL). Five subjects were categorized into immune escape phase [elevated HBV DNA levels (11832–52432 copies/mL) and high ALT (>40 IU/L)], and required antiviral therapy. Eight subjects had serum HBV DNA levels ranging from 116 copies/mL to 10000 copies/mL, and ALT was normal. Six subjects had undetectable HBV DNA level (lower limit of HBV DNA: <116 copies/mL) and normal ALT. These 14 subjects were categorized into immune control phase.
HBV genotypes were available in 22 subjects with detectable HBV DNA. Their phylogenic tree is shown in Fig. 2. Genotypes B and C were found in 54.6% (n=12) and 45.4% (n=10) of the subjects, respectively. As mentioned previously, genotype C was more common in China (n=8, 80%), and genotype B was more common in Vietnam (n=7, 58.3%) and Cambodia (n=3, 25%).
 | Fig. 2Phylogenetic maximum likelihood tree for 22 subjects with positive HBV DNA. Sequences from China, Vietnam, and Cambodia are represented by closed circles, squares, and triangles, respectively. Reference sequences obtained from GenBank are marked with open circles. HBV genotypes B and C are also shown. Genotypes B and C obtained from GenBank (Accession numbers AB010290.B1, AB073830.B2, AB73823.B2, M54923.B3, AY033072.B4, AB073835.B4, AB219429.B5, AY123041.C1, AY217371.C1, AB205124.C2, X75656.C3, X75665.C3). HBV, hepatitis B virus; CHN, China; VIE, Vietnam; CAM, Cambodia.
|
Seroprevalence of hepatitis C virus
Eight (0.8%) subjects were positive for anti-HCV. Seroprevalence of anti-HCV was high in subjects from Central Asia (n=3, 7.9%) (Table 3). None of the subjects presented positive for HBV and HCV coinfection.
Go to :
DISCUSSION
For the first time, this study investigated the seroepidemiology of hepatitis viruses and hepatitis B genotypes in female marriage immigrants in Korea. Of a total of 963 subjects, 52 (5.4%) was positive for HBsAg, and eight (0.8%) was positive for anti-HCV. HAV and HBV vaccinations were required for 288 (29.9%) and 329 (34.2%) subjects, respectively. In particular, HBV genotypes were available in 22 HBsAg-positive subjects. Genotype B (n=12, 54.6%) was found in a slightly higher number of female marriage immigrants compared to genotype C (n=10, 45.4%).
Prior to 1990, majority of Koreans had acquired natural immunity to HAV by their 20s.21 With improvements in socioeconomic status, opportunities for exposure have decreased; consequently, rates of childhood HAV infection have reduced remarkably, and severe symptomatic hepatitis A infection in adolescents and adults has increased over the last 10 years.2223 In 2015, recent data indicated that the seropositive rate of IgG anti-HAV in 15–29 age group was still low (15–19 years, 22.7%; 20–24 years, 18.4%; 25–29 years, 16.3%; 30–34 years, 26%; 35–39 years, 54.8%).24 Especially, seropositive rate of IgG anti-HAV in 20–29 age group was reported to be only 18%, and 71.3–84% of acute hepatitis A occur in this age group.21 Therefore, Korean adults younger than 30 years of age should be vaccinated without antibody testing, and those of age 30 years or older should be vaccinated in cases involving negative serologic tests.25
In contrast, seroprevalence of IgG anti-HAV was significantly higher in female marriage immigrants from Asian countries (20–29 years, 63.3%; 30–40 years, 72.7%). Interestingly, in female marriage immigrants from Japan, only six subjects (15.4%) were immune to HAV in the age group under 40 years. This variance may reflect differences in HAV seroepidemiology in the subjects' own countries.26 Several studies have suggested that differences in seroprevalence can be attributed to geological, environmental, and socioeconomic conditions rather than ethnicity.27 Fortunately, safe and efficacious vaccine is available, providing an opportunity to lower disease burden and potentially eliminate infection. Considering the estimated prevalence of hepatitis in each country, we recommend that most immigrants, with the exception of those from Japan, should be tested for HAV immunity before vaccination. However, immigrants from Japan might be vaccinated without antibody testing in the age group under 40 years, as in Korean adults younger than 30 years of age.
Overall, 5.4% (n=52) of female marriage immigrants were positive for HBsAg, and anti-HBs was found in 60.4% (n=582). Sixty-two percent of countries in East, Southeast, and Central Asia have implemented universal HBV vaccination since 1990. These countries have achieved more than 70% coverage of completed HBV vaccination (China, 99%; Thailand, 99%; Cambodia, 97%; Vietnam, 95%; the Philippines, 79%; Uzbekistan, 82%, Mongolia, 76%).28293031 Therefore, the prevalence of anti-HBs gradually increased in East, Southeast, and Central Asia after implementation of universal HBV vaccination program.
As in the case of HAV infection, no subject with HBsAg was found in immigrants from Japan; however, seroprevalence of HBsAg positive was 5% higher compared to those from Vietnam and Cambodia. Likewise, in systematic review and pooled analysis, Vietnam (10.8%) and Mongolia (9.1%) showed the highest endemicity (HBsAg prevalence ≥8%). Uzbekistan (7%), Thailand (6.4%), Kazakhstan (6.1%), and China (5.5%) were of higher-intermediate endemicity (HBsAg prevalence 5–7.99%). The Philippines (4.6%), Korea (4.4%), and Cambodia (4.1%) were of lower-intermediate endemicity (HBsAg prevalence 2–4.99%). Japan (1%) had the lowest level of endemicity (HBsAg prevalence <2%).32
We assumed that most HBsAg-positive individuals were infected in their own countries, but we did not know the mode or time of infection. Fewer than 10% of immunocompetent adults, who were infected with HBV, developed chronic infection; however, 80–90% of perinatal transmission of HBV infection remains chronic.33 In this study, 50% (n=14) of HBsAg-positive subjects with written informed consent about HBV DNA genotyping (n=28) showed elevated HBV DNA levels higher than 10000 copies/mL. Especially, 35.7% (n=10) of HBsAg-positive subjects required antiviral therapy. This is highlighted by the fact that HBV-infected female marriage immigrants with immune active phase or immune escape phase were sexually active women of childbearing age, who were highly likely to become pregnant.
In Korean National Health and Nutritional Examination Survey 2014, HBsAg-positive rates were 1.7% in female subjects 20–29 years and 3.2% in female subjects 30–39 years.34 In this study, HBsAg-positive rates in female marriage immigrants were 4.5% in 20–29 years and 5.7% in 30–40 years. Rate of HBsAg carriage was higher in female migrants than in Korean women. Moreover, 168853 children from multicultural families were identified by the Ministry of Security and Public Administration. A considerable number of children could have been exposed via mother-to-infant transmission. As mentioned, the number of female marriage immigrants was gradually increased.1 More than 80% of the immigrants came from HBV endemic areas, such as China (45301, 35.2%), Vietnam (40479, 31.5%), the Philippines (11272, 8.8%), Cambodia (4412, 3.4%), and Thailand (3105, 2.4%). Therefore, early detection of HBV infection, through mass screening of HBV seromarkers, will induce timely and optimal antiviral therapy and finally prevent liver-related morbidity and mortality. In addition, appropriate immunization in spouse is needed to prevent horizontal infection. Perinatal care and health education on the prevention of vertical transmission should be covered by well-organized health programs.
Furthermore, neither HBsAg nor anti-HBs were found in 329 (34.2%) subjects who required HBV vaccination in our study. In previous reports about health exams supported by the Ministry of Health and Welfare in 2008, about 40% to 60% of immigrants wives were susceptible to HBV infection.35 However, available resources for HBV prevention targeting female marriage migrants offer little access to health services.34 As with hepatitis A infection, efficacious and cheap vaccine is available for HBV infection. Therefore, financial support and health service for HBV vaccination should be provided to unimmunized immigrants.
Genotypes B and C are prevalent in Asian Pacific regions, and the prevailing HBV genotype in Korea is C.1718 When HBV infections were compared, with respect to genotypes B and C, infection via genotype C showed higher incidence of progression to cirrhosis and hepatocellular carcinoma, less favorable HBeAg seroconversion response to standard or pegylated interferon, and lower incidence of HBsAg seroclearance.15163637 In our study, 22 strains were available in the analysis of HBV genotypes. Their phylogenic tree only showed genotypes B (54.6%, n=12) and C (45.4%, n=10). Genotype C was found in eight out of 10 subjects from China, and genotype B was found in seven out of nine subjects from Vietnam. Such finding is consistent with those of previous reports.16 Geographic differences have not affected the distribution of HBV genotype in Korea,1718 while an epidemiological study conducted in China showed that genotypes B was primarily distributed in the south and genotype C in the north of the country.38 With the increase in incidence of transnational marriage, infection with genotype B could increase if we do not implement certain measures, such as screening and appropriate vaccination. HBV genotype is an important determinant in management. Therefore, medical expenses might increase to discriminate genotype for an individualized approach.
Estimated prevalence of anti-HCV positive rate in China was 1–1.9%. In a recent report using an estimated 2009 population of Korea, the age, sex, and area-adjusted anti-HCV positive rate was 0.78%.20 Age-related prevalence of anti-HCV positive was 0.34% in subjects aged 20 to 29 years, and 0.41% in subjects aged 30 to 39 years.20 Our study showed that eight (0.8%) out of 963 subjects were positive for anti-HCV. Rates of anti-HCV positive in female marriage immigrants were 0.8% in 20–29 year-olds and 0.9% in 30–40 year-olds. Rate of anti-HCV positive was also higher in female migrants than in Korean women.
A systematic study showed that the estimated prevalence of HCV in the entire Asian continent was 2.8% (Japan, 1.5%; the Philippines, 0.8%; Cambodia, 2.5%; Thailand, 2.7%; Uzbekistan, 11.3%; Mongolia, 8.5%; Kazakhstan, 2.9%).39 Although the prevalence of HCV was lower than that of HBV, most countries showed higher prevalence rate compared to Korea.
The present study had several limitations. First, it is impossible to know the mode and time of infection, since serologic tests were not conducted at the time of immigration or marriage, and subjects did not have reliable immunization records. However, we can assume that most hepatitis infections were acquired in the subjects' own countries, based on our results concerning seroprevalence and distribution of genotypes. Second, although many immigrants in transnational marriages reside in urban areas, other rural areas may show different patterns of seroepidemiology depending on subjects' home countries. However, authors tried to include urban and rural immigrants in the same proportion. Third, despite a considerable number of subjects participating in the screening program, numerous countries were represented by multicultural families, and analysis according to each country was infeasible in most cases. Therefore, it was difficult to ensure representative character. Fourth, a better knowledge based on gross national product and ethnicity may be critical for a complete understanding of the seroprevalence of hepatitis viruses. In addition, female marriage migrants also face financial difficulties in Korea. More than half of them fall below poverty levels (www.korea.kr/common/download.do?tblKey=EDN&fileId=211426).40 Furthermore, female marriage immigrants have limited access to healthcare services and support, due to linguistic barrier and economic difficulties.35 Finally, greater investment will be needed in public health research to evaluate the prevalence of seromarkers of hepatitis E virus in immigrants from high endemic areas, as well as the prevalence of HBV and hepatitis D virus coinfection in North Korean immigrants.
This survey is the first seroepidemiological analysis of hepatitis viruses and HBV genotypes in female marriage immigrants in Korea. Testing for hepatitis viral marker (HAV IgG and HBsAg/anti-HBs) is needed for female marriage immigrants. Especially, HBV genotype B is different from genotype C of Koreans. As the number of transnational marriages increases, interest and attention to vaccination program for female marriage immigrants is required for both clinicians and public health institutes.
Go to :
 XML Download
XML Download