

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Coronary artery spasm (CAS) is a form of endothelial dysfunction implicated in acute coronary syndrome (ACS) or vasospastic angina (VSA).123456 Diabetes mellitus (DM) and imimpaired glycemic control are well-known risk factors for cardiovascular disease and are associated with poor clinical outcomes, such as high mortality and poor quality of life.78 Insulin resistance (IR) is the main etiological cause of type 2 DM and is associated with worse clinical outcomes.78 Despite the observed relationships among cardiovascular dysfunction, DM, and IR, associations between CAS and IR in non-diabetic individuals has not been elucidated. The aim of the present study was to evaluate the impact of IR on CAS in patients without DM.
MATERIALS AND METHODS
The present study utilized data from a single-center, prospective, all-comer registry implemented in 2004 that was designed to reflect “real world” practice. The design of this registry has been described previously in detail.91011121314 Data were collected by a trained study-coordinator with a standardized case report form. Standardized definitions of all patient-related variables and clinical diagnoses were used. The participants or their legal guardians were given a thorough, literal, and verbal explanation of the study procedures before granting written consent to participate in the study. The Institutional Review Board (IRB) of Korea University Guro Hospital (KUGH) approved all of the consenting procedures. The authors of this manuscript have certified that the information contained herein is true and correct as reflected in the records of the IRB (#KUGH10045). The KUGH IRB specifically approved this entire study.
A total of 10177 patients with typical or atypical chest pain who received coronary angiography (CAG) at the Cardiovascular Center of KUGH in Seoul, South Korea between November 2004 and May 2014 were enrolled in this study. Among these, 5812 patients with typical or atypical chest pain without significant coronary artery disease (CAD) [defined as having a stenosis diameter of more than 70% on the quantitative coronary angiography (QCA)] underwent intracoronary acetylcholine (Ach) provocation test. Inclusion criteria included both hemoglobin A1c <6.0 % and fasting glucose level <110 mg/dL without diabetes medication or prior diagnosis thereof.8 Fasting glucose, serum insulin, and hemoglobin A1c level of enrolled patients were measured, and homeostasis model assessment of insulin resistance (HOMA-IR) index was calculated before conducting CAG. Patients were excluded if they had any of the following conditions: coronary artery bypass graft, prior percutaneous coronary intervention, prior cerebrovascular disease, advanced heart failure (New York Heart Association class III or IV), serum creatinine ≥2 mg/dL, or myocardial bridge, since these conditions could be major causes for adverse cardiovascular events and could bias the results. A total of 330 eligible patients without DM were divided into quartile groups: 1Q (n=82; HOMA-IR<1.35), 2Q (n=82; 1.35≤HOMA-IR<1.93), 3Q (n=83; 1.93≤HOMA-IR<2.73), and 4Q (n=83; HOMA-IR≥2.73). The incidence of CAS and angiographic and clinical parameters during the Ach provocation test were compared among the different quartile groups.
Study definition
Hypertension was diagnosed according to a history of hypertension and treatment with medication, diet, and/or exercise. Dyslipidemia was defined as having a total cholesterol level ≥200 mg/dL or undergoing current treatment with lipid-lowering drugs for controlling increased blood lipid level. Current cigarette smoking was defined as active smoking within the past 12 months. Significant CAS was defined as having greater than 70% luminal narrowing of the artery during the Ach provocation test regardless of ischemic ECG changes or presence of chest pain. Myocardial bridge was defined as phasic systolic compression of the coronary artery with a decrease of more than 30% in diameter on an angiogram after intracoronary nitroglycerin infusion, mostly in the anterior-posterior cranial or right anterior oblique cranial projection. Multi-vessel spasm was defined as significant CAS occurring at more than two major epicardial arteries. Diffuse spasm was defined as significant CAS with site length measuring more than 20 mm. Apontaneous spasm was defined as focal or diffuse narrowing greater than 30% at baseline CAG, compared to the reference vessel diameter after nitroglycerin administration via an intracoronary route. The HOMA-IR index was calculated as follows: [fasting plasma insulin (µU/mL)×fasting glucose (mg/dL)]/405.15
Acetylcholine provocation test
The design of the Ach provocation test has been described before.910111213 Initial investigation for CAG included clinical history taking and non-invasive stress tests, such as treadmill test, stress echocardiography, and radionuclide study. Then, CAG was performed to confirm the presence of significant CAD. CAG was performed immediately without functional studies in case of typical resting ischemic chest pain to confirm VSA. Vasodilators or vasoconstrictors, such as nitrates, calcium channel blockers, beta blockers, nicorandil, and molsidomine, were discontinued at least 72 hours before CAG. CAS induction was tested by intracoronary injection of Ach immediately after diagnostic angiography by either a trans-radial or trans-femoral approach. Ach was injected by incremental doses of 20 (A1), 50 (A2), and 100 (A3) µg/min into the left coronary artery on a 1-minute period with 5-minute intervals up to the maximal tolerated dose under continuous monitoring by electrocardiogram and measuring of blood pressure. Provocation of the right coronary artery was not done routinely due to safety issues, as the insertion of a temporary pacemaker is required to prevent advanced atrioventricular block during Ach infusion. Angiography was repeated after each Ach dose until a significant focal or diffuse narrowing greater than 70% was observed. If significant focal or diffuse vasoconstriction (>70%) of coronary arteries was induced at any dose, Ach infusion was stopped. An intracoronary injection of 0.2 mg of nitroglycerine was administered after completing the Ach provocation test, followed by CAG 2 minutes later. End-systolic images for each segment of the left coronary artery were chosen according to the corresponding points on the electrocardiographic trace (QRS onset or end of T wave) and analyzed using a proper QCA system in the catheterization laboratory (FD-20, Phillips, Amsterdam, the Netherlands). Coronary artery diameters were measured with QCA before and after administration of Ach at the site that showed the greatest changes following drug administration. Reference vessel diameters were measured at proximal and distal portions of each artery. The mean reference vessel diameter was used to assess diameter narrowing by QCA.
Statistical analysis
All statistical analyses were performed using SPSS 20 (IBM Corp., Armonk, NY, USA). For continuous variables, differences among three groups were evaluated by ANOVA or Joncheere-Terpstra, and post-hoc analysis between two groups was evaluated by Hochberg or Dunnett-T3 test. Data are expressed as a mean±standard deviation. For discrete variables, differences among the three groups are expressed as counts and percentages, and were analyzed with χ2 or Fisher's exact test as appropriate. Multivariable Cox-hazards regression that included baseline confounding factors was used for assessing independent impact factors. We tested all available variables that could be of potential relevance: age, sex and cardiovascular risk factors (hypertension, dyslipidemia, current smokers and current alcohol drinkers, and insignificant coronary stenosis). A two-tailed p value of <0.05 was considered statistically significant.
RESULTS
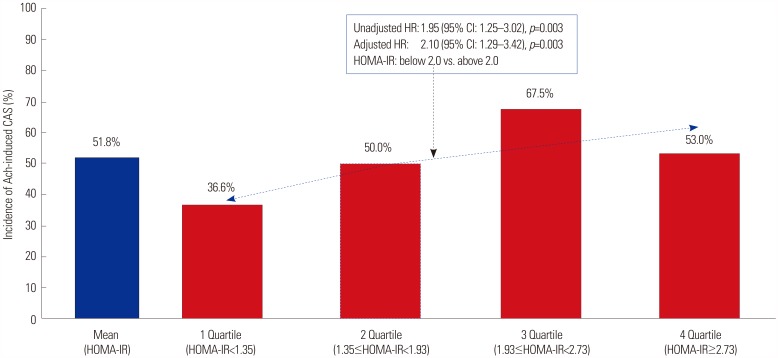
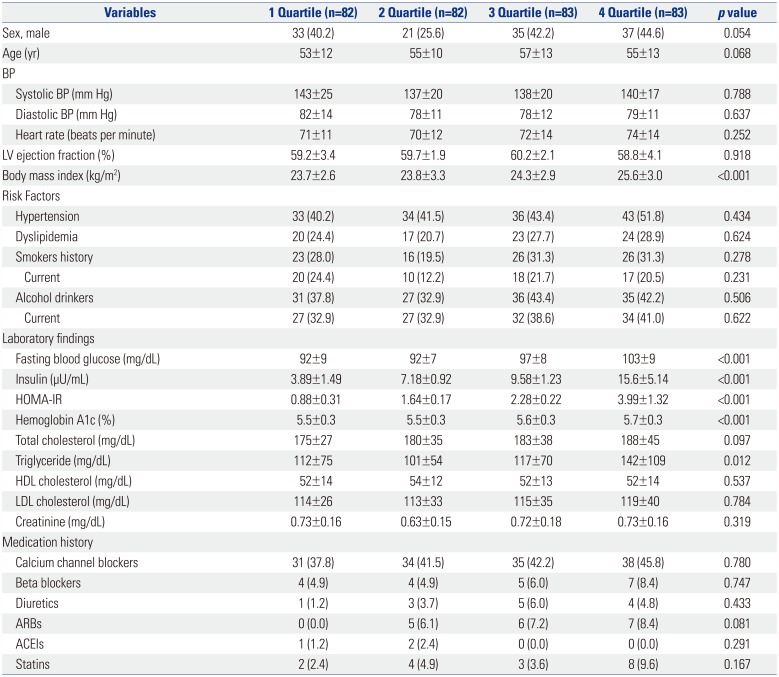
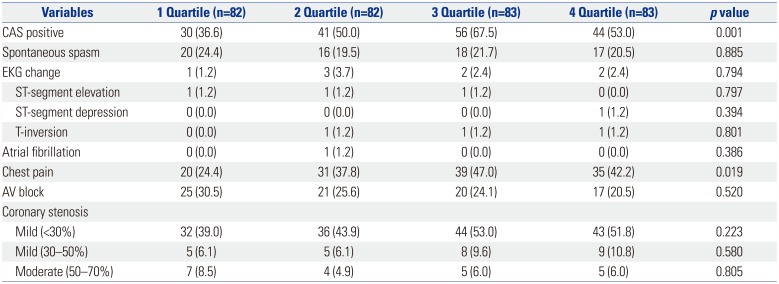
To assess the association between HOMA-IR and Ach-induced CAS, patients were divided into quartile groups according to HOMA-IR levels: 1Q (n=82; HOMA-IR<1.35), 2Q (n=82; 1.35≤HOMA-IR<1.93), 3Q (n=83; 1.93≤HOMA-IR<2.73), and 4Q (n=83; HOMA-IR≥2.73). There were considerable differences in baseline characteristics, such as age, sex (male), body mass index, glycemic control (hemoglobin A1c) and levels of lipid profile (total cholesterol, triglyceride), among the quartile groups (Table 1). The higher HOMA-IR groups (3Q and 4Q) were older; had higher body mass index, fasting blood glucose, serum insulin, hemoglobin A1c, total cholesterol, and triglyceride levels; and received more angiotensin receptor blockers and statin treatments than the lower HOMA-IR group (1Q). As shown in Table 2, there were significant differences in angiographic and clinical parameters among the quartile groups during Ach provocation test. The higher HOMA-IR groups (3Q and 4Q) had more CAS and chest pain than the lower HOMA-IR group (Q1) (Fig. 1, Table 2). As shown in Table 3, HOMA-IR was positively correlated with CAS regardless of adjusting for baseline confounders in Cox regression analysis.
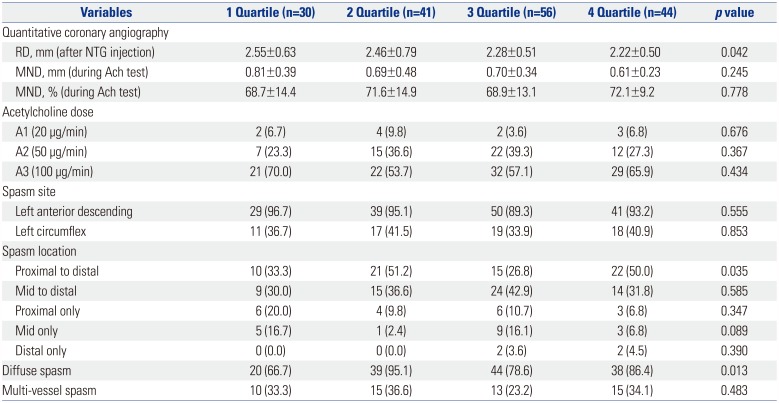
The higher HOMA-IR groups (3Q and 4Q) had higher CAS risk than the lower HOMA-IR group (Q1). Taking HOMA-IR above 2.0 as a cut off, mostly including Q3 and Q4, the hazard ratios (HRs) for CAS were 1.95 (95% CI: 1.25–3.02), and 2.10 (95% CI: 1.29–3.42) in un-adjusted or adjusted Cox regression analysis, respectively. In CAS patients, HOMA-IR was significantly negatively correlated with reference diameter measured after nitroglycerin and significantly positively correlated with diffuse spasm (Table 4).
DISCUSSION
In the present study, which analyzed non-diabetic subjects, the main findings were as follows: 1) IR is considerably linked to age, sex, body mass index, and high levels of triglyceride. Also, 2) HOMA-IR is positively correlated with CAS incidence during Ach provocation test.
Obstructive CAS, which is implicated in endothelial dysfunction, induces ACS and VSA.123456 Meanwhile, IR subjects are at a greatly increased risk of developing type 2 DM and is associated with obesity, hypertension, dyslipidemia, and metabolic syndromes.781617 Many studies have shown associations among IR and its effects on vasculature and endocrine system.21819 However, associations between CAS and IR in non-diabetic individuals has not been studied. A few studies have reported that IR is closely linked to endothelial dysfunction and causes endothelial dysfunction in peripheral circulation; however, whether it impairs endothelial function in coronary circulation has not been proven.2021 This is the first report on the associations between IR and CAS in non-DM subjects.
In the present study, poor IR was strongly associated with CAS in patients without DM. Compared with Q1, the HRs for Q3 and Q4 were 3.55 (95% CI: 1.79–7.03, p<0.001) and 2.12 (95% CI: 1.07–4.21, p=0.031), respectively, after adjustment of baseline risk confounders. Also, diffuse spasm and accompanying chest pain during Ach provocation test were more strongly associated with IR patients with CAS (Tables 3 and 4). In our previous study, which assessed 986 patients who underwent Ach provocation test, we found no relationships among DM, blood sugar control status, and CAS.9 However, in the present study on non-DM subjects, IR showed a strong, positive association with CAS. These findings suggest that there may be different mechanisms at play between prognostic CAS and IR according to DM status. Lee, et al.22 reported the optimal cut off of HOMA-IR for type 2 DM is 1.97 (AUC=0.807; 95% CI=0.777–0.886; sensitivity=65.5%, specificity=82.9%). In the present study on non-DM subjects, the HOMA-IR of higher IR groups, such as Q3 (1.93≤HOMA-IR<2.73) and Q4 (HOMA-IR≥ 2.73), was similar to the HOMA-IR of DM patients. As shown in Fig. 1, CAS incidence was highest in Q3 and decreased in Q4, supporting our hypothesis.
At the cellular level, insulin works via two pathways. The phosphatidylinositol 3-kinase (PI3K)-dependent signaling pathway is involved in nitric oxide (NO) production and vasodilation in vascular endothelium.2324 Another signaling pathway is the mitogen activated protein kinase (MAPK)-dependent insulin-signaling pathway that regulates the secretion of vasoconstrictor endothelin-1 (ET-1) and intracellular adhesion molecules 1, as well as vascular cell adhesion molecule 1 expression in vascular endothelium.2324 However, such signaling pathways seem to be impaired in an IR state. Glucotoxicity, lipotoxicity, and inflammation are often present in an IR state.25 Various cytokines produced in inflammation inhibit NO production and vascular endothelial vasodilation by down-regulating the PI3K signaling pathway. Moreover, endothelial IR is generally characterized by selective impairment in PI3K-NO signaling but an intact MAPK-dependent pathway.2324 This causes reduced expression of endothelial NO synthase protein and NO and increased release of vasoconstrictor ET-1, collectively resulting in endothelial vasoconstriction.2 Such endothelial dysfunction mechanisms support our results of a positive correlation between IR patients and a greater risk of having CAS.
Our study showed that insulin-resistant groups (Q3 and Q4) had higher blood insulin levels that fall under hyperinsulinemia. As previously mentioned, these patients also had more frequent CAS. Nakagomi, et al.26 demonstrated that IR associated with compensatory hyperinsulinemia increases the risk of other cardiac events in VSA. Also, another study reported that compensatory hyperinsulinemia in IR patients causes endothelial dysfunction.23 Hence, in a hyperinsulinemia state, the insulin-induced vasodilatory effect is impaired. Also, at baseline, the IR groups showed higher prevalences of old age, male gender, and high body mass index and triglyceride levels (Table 1). These factors are well-known risk factors for type 2 DM and IR.8
There were several limitations in the present study. First, IR was calculated by the HOMA-IR index, which is not a direct method. Other well-designed prospective studies are necessary to derive a definite conclusion. Second, medication history is important to furthering detailed analyses. However, in this study, medication sub-type and duration were not demonstrated clearly due to retrospective analysis design. Third, the present study was analyzed retrospectively, and multivariable Cox-proportional regression analysis was performed to minimize confounding factors that might have influenced the results. Also, the registry was designed with an all-comer prospective registry from 2004. We could not adjust for all limiting factors not included in the medical records or collected through telephone contact.
To summarize our study, IR was positively associated with CAS on non-DM subjects. Recent studies have shown that improving lifestyle and medication interventions not only improve the symptoms and prevent complications of diabetes but also prevent the onset of type 2 DM.272829 Therefore, medication interventions along with an improving lifestyle should be suggested for these patients.

 XML Download
XML Download