

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Two randomized controlled trials (RCTs) recently demonstrated that complete revascularization (CR) in ST-segment elevation myocardial infarction (STEMI) and multivessel disease (MVD) was associated with good clinical outcomes including a favorable tendency toward reducing mortality or myocardial infarction (MI).1)2)3) Thus, the American College of Cardiology/American Heart Association and European Society of Cardiology (ESC) guidelines now state CR as a class IIb recommendation in hemodynamically stable patients with STEMI and MVD.4)5) Sequentially, meta-analyses of larger populations confirmed that CR in STEMI patients with MVD is a safe and effective strategy at the time of primary percutaneous coronary intervention (PCI) or other staged procedure.6)7)8)9)
New-generation drug-eluting stents (DESs) have been associated with lower rates of target lesion revascularization (TLR) and stent thrombosis compared with early-generation DES and bare metal stents (BMSs).10)11)12) The ESC guideline recommends new-generation DES over BMS in non-STEMI patients.5) However, the above studies comparing CR versus culprit-only revascularization in patients with STEMI and MVD used only BMS or early-generation DES. Thus, the purpose of this study is to compare the 1-year outcomes of CR versus culprit-only revascularization for STEMI and MVD in the 2nd generation DES era.
METHODS
Study patient selection
We collected the demographic, clinical, and angiographic findings of STEMI patients who underwent successful primary PCI on the index admission between 2009 and 2014 and completed 1 year of routine follow-up from the INcheon-Bucheon cohorT of patients undERgoing primary percutaneous coronary intervention for acute ST-ELevation myocardiaL infARction (INTERSTELLAR) registry cohort. CR was defined as PCI for a significant lesion to that for non-culprit lesions during the index admission. Non-culprit lesions were defined as lesions ≥50% in coronary arteries and reference vessel size ≥2.0mm. Patients were included if they received a 2nd generation DES at the culprit lesion (everolimus-eluting stent [EES], zotarolimus-eluting stent [ZES], biodegradable polymer DES [BD-DES], and PROMUS Element). The revascularization was performed according to current practice guidelines. The decision to perform whether CR or culprit only PCI were left to the operators. We excluded MVD patients who underwent intended non-infarct-related artery PCI after index admission, use of plain old balloon angioplasty (POBA), BMS, or 1st generation DES. This registry was approved by the Institutional Review Boards of the 4 hospitals (approval number: INHAUH 2016-05-015).
Outcome measures
Major adverse cardiovascular event (MACE) was defined as cardiovascular (CV) mortality, non-fatal MI, and ischemia-driven TLR, and heart failure (HF) during the follow-up period.13)14) HF was defined as re-hospitalization with symptoms for the congestive HF. For patients with multiple CV events, only the first event was used in the analysis. Patient follow-up data were collected using electronic medical record reviews and/or standardized telephone interviews.
Statistical methods
Continuous data are expressed as mean±standard deviation or median (interquartile range). Categorical data are presented as a percentage or absolute number. The analyses were done using unpaired t-tests or Wilcoxon test for continuous data and the χ2 test or Fisher's exact test for categorical data. Cumulative event rates as a function of time were estimated using the Kaplan-Meier method and compared using the log-rank test. Hazard ratio (HR)13) was calculated as an estimate of the risk associated with a particular variable with 95% confidence intervals (CIs) based on binomial distributions. Uni- and multi-variate regression analyses were performed to determine the associations between clinical characteristics and clinical outcomes. All analyses were performed using SPSS version 19.0 (SPSS Inc., Chicago, IL, USA). The p values <0.05 were considered statistically significant.
RESULTS
From 2009 to 2014, 1,537 STEMI patients who underwent primary PCI were suitable for the analysis. Among them, 832 (54%) were excluded for having single-vessel disease or using a BMS or 1st generation DES. Ultimately, 705 (46%) with MVD were included, of whom 286 (41%) underwent culprit-only PCI and 419 (59%) underwent CR during the index admission (Figure 1). The 2nd generation DES included: EES in 259 (37%); ZES in 193 (27%); PROMUS Element in 165 (23%); and BD-DES in 88 (12%).
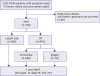 | Figure 1Participant flow chart.BMS = bare metal stent; CR = complete revascularization; CV = cardiovascular; DES = drug eluting stent; HF = heart failure; MACE = major adverse cardiovascular event; MI = myocardial infarction; MVD = multivessel disease; POBA = plain old balloon angioplasty; STEMI = ST-segment elevation myocardial infarction; TLR = target lesion revascularization.
|
Culprit-only PCI vs. CR
The patients' baseline and procedural characteristics are shown in Table 1. The culprit-only PCI group was older (64±13 vs. 62±13 years, p<0.01) and had a higher prevalence of hypertension (58% vs. 49%, p=0.02) and lower use of aspiration thrombectomy (35% vs. 47%, p<0.01) and glycoprotein IIb/IIIa inhibitor (29% vs. 36%, p=0.04). Initial thrombolysis in myocardial infarction (TIMI) flow grade (p<0.01) and type of 2nd DES used differed between the 2 groups (p<0.01).
Table 1
Characteristics of patients with culprit-only PCI versus CR

Values are expressed as mean±SD, median (interquartile range), or number (percentage).
ACE = angiotensin-converting enzyme; ARB = angiotensin receptor blocker; BD-DES = biodegradable polymer drug-eluting stent; CKD = chronic kidney disease; CK-MB = creatine kinase-MB; CR = complete revascularization; DTB = door to balloon time; EES = everolimus-eluting stent; IABP = intra-aortic balloon pump; LAD = left anterior descending artery; LVEF = left ventricular ejection fraction; MI = myocardial infarction; PCI = percutaneous coronary intervention; STB = symptom to balloon time; TIMI = thrombolysis in myocardial infarction; ZES = zotarolimus-eluting stent.
![]()
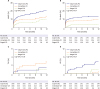
The incidence of MACE was 11.5% in the CR group versus 18.5% in the culprit-only PCI group (HR, 0.56; 95% CI, 0.372–0.869; p<0.01) in the 1-year follow-up period. The CR group revealed significantly lower rates of CV death (7.2% vs. 12.9%; HR, 0.51; 95% CI, 0.313–0.862; p=0.01) and admission for HF (1.0% vs. 4.2%; HR, 0.22; 95% CI, 0.070–0.689; p<0.01). In detail, there were no significant differences on non-fatal MI (1.4% vs. 0.3%, p=0.18) and TLR (1.8% vs. 1.0%, p=0.37). After the adjustment of confounding values, including age, hypertension, aspiration thrombectomy, glycoprotein IIb/IIIa inhibitors, initial TIMI grade, and DES type, the CR group still revealed significantly lower rates of MACE (HR, 0.64; 95% CI, 0.407–0.996; p=0.04), CV death (HR, 0.57; 95% CI, 0.329–0.971; p=0.03), and HF (HR, 0.26; 95% CI, 0.080–0.868; p=0.02, Table 2). The relative effect of CR on MACE and CV death (Figure 2) was consistent across the pre-specified subgroups. Among the patients with CR, those of age >60 or Killip class II–IV were independent predictors of reduced MACE and CV death.
Table 2
One-year outcomes, culprit-only PCI versus CR

Values are number (%).HR adjusted for age, culprit lesion, hypertension, aspiration thrombectomy, glycoprotein IIb/IIIa inhibitor use, pre-thrombolysis in MI, and DES type, proximal culprit lesion, and 3-vessel disease.
CR = complete revascularization; CV = cardiovascular; DES = drug-eluting stent; HF = heart failure; HR = hazard ratio; MACE = major adverse cardiovascular event; MI = myocardial infarction; MVD = multivessel disease; PCI = percutaneous coronary intervention; TLR = target lesion revascularization.
![]()
 | Figure 2Subgroup analyses for MACE & CV death between culprit-only versus CR.BD-DES = biodegradable polymer drug-eluting stent; CI = confidence interval; CKD = chronic kidney disease; CR = complete revascularization; CV = cardiovascular; DM = diabetes mellitus; EES = everolimus-eluting stent; EF = ejection fraction; HR = hazard ratio; LAD = left anterior descending artery; MACE = major adverse cardiovascular event; TIMI = thrombolysis in myocardial infarction; ZES = zotarolimus-eluting stent.
|
Immediate versus staged-CR
In the CR group, 288 (69%) patients underwent CR during the index primary PCI (immediate-CR) and 131 (31%) underwent staged-CR at the index admission (staged-CR). Mean duration of staged PCI was 2.3 days from the index PCI. The immediate-CR group had a lower baseline prevalence of hypertension (45% vs. 58%, p=0.01), left anterior descending artery (LAD) culprit (41% vs. 53%, p=0.02), proximal culprit lesion (41% vs. 53%, p=0.02), 3-vessel disease (39% vs. 60%, p<0.01), and use of aspiration thrombectomy (42% vs. 57%, p<0.01) and glycoprotein IIb/IIIa inhibitor (21% vs. 48%, p<0.01). Initial TIMI grade (p<0.01) and 2nd generation DES type used differed between the 2 groups (p<0.01).
The incidence of MACE was 9.2% in the staged-CR group versus 12.5% in the immediate-CR group (HR, 0.70; 95% CI, 0.355–1.406; p=0.32) in the 1-year follow-up. The staged-CR group revealed significantly lower CV death (3.1% vs. 9.0%; HR, 0.31; 95% CI, 0.108–0.929; p=0.03). After the adjustment for baseline differences in patent and angiographic variables, the staged-CR group maintained its lower rates of MACE (HR, 0.53; 95% CI, 0.257–1.127; p=0.10) and CV death (HR, 0.23; 95% CI, 0.078–0.732; p=0.01, Table 3). Regardless of CR strategy, the immediate-CR and staged-CR groups were associated with better overall outcomes of MACE and CV death (Figure 3) than the culprit-only PCI group.
Table 3
One-year outcomes, immediate CR versus staged-CR

Values are number (%).HR adjusted for age, culprit lesion, hypertension, aspiration thrombectomy, glycoprotein IIb/IIIa inhibitor use, pre-thrombolysis in MI, and DES type, proximal culprit lesion, and 3-vessel disease.
CR = complete revascularization; CV = cardiovascular; DES = drug-eluting stent; HF = heart failure; HR = hazard ratio; MACE = major adverse cardiovascular event; MI = myocardial infarction; TLR = target lesion revascularization.
![]()
DISCUSSION
The data from the INTERSTELLAR registry for patients with STEMI and MVD indicated that CR was associated with better outcomes, including reduced MACE and CV death at 1-year follow-up compared with culprit-only PCI in the 2nd generation DES era. Regarding CR strategy, the staged-CR group was correlated with a trend toward better outcomes compared with the immediate-CR group.
Early reports of late and very late stent thrombosis were associated with 1st generation DES, including sirolimus-eluting stents and paclitaxel-eluting stents, especially in cases of dual-antiplatelet therapy cessation.15)16) Thus, newer-generation DES has been developed with the intent of improving the overall safety of earlier DES while maintaining anti-restenotic efficacy. As a result, new-generation DES, with more biocompatible polymers, have been shown to provide benefits in stent thrombosis at early and mid-term follow up in the STEMI setting.17)-19) In addition, recent studies revealed that, compared with early-generation DES, new-generation DES were associated with a lower MACE rate in STEMI patients compared with early-generation DES.20)21) Finally, the latest ESC guideline recommended that new-generation DES should be used in patients with acute coronary syndrome.5) In cases of patients with STEMI and MVD, more DES would be used to treat both culprit and non-culprit unstable lesions; thus, DES efficacy and safety could be crucial prognostic determinants in the early and long-term period.
There have been three large RCTs to date that demonstrated that CR use in STEMI and multi-vessel MVD was associated with better clinical outcomes.1)-3) The Preventive Angioplasty in Acute Myocardial Infarction (PRAMI) trial enrolled 465 STEMI and MVD patients between 2008 and 2013. The use of DES at the culprit lesion occurred in approximately 60% of enrolled patients, but there were no data for DES type, and BMS was used in approximately 40% of enrolled patients for culprit lesion intervention. CR was associated with a 65% reduction in death from cardiac causes, non-fatal MI, or refractory angina compared with culprit-only PCI (HR, 0.35; 95% CI, 0.21–0.58; p<0.001). CV death as the composite endpoint was numerically reduced (HR, 0.36; 95% CI, 0.11–1.08; p=0.17).2) Next, the Complete versus Lesion-only Primary PCI Trial (CvLPRIT) enrolled 296 STEMI and MVD patients between 2011 and 2013. Compared with the PRAMI trial, use of DES at the culprit lesion was significantly increased to up to 93% of enrolled patients, but there were no data for DES type. The CR was associated with a 55% reduction in MACE including death, recurrent MI, HF, and repeat revascularization compared with culprit-only PCI (HR, 0.45; 95% CI, 0.24–0.84; p=0.001). The CV death rate was also lower; however, the difference was not statistically significant (HR, 0.32; 95% CI, 0.06–1.60; p=0.14).2) Finally, the PRIMULTI trial enrolled 627 STEMI and MVD patients. The use of DES (especially EES) was preferred for additional PCI procedures in the CR group. Although DES type was not clear, DES was used in >90% of patients in both groups. The CR significantly reduced the composite of all-cause death, non-fatal MI, and ischemia-driven revascularization (HR, 0.56; 95% CI, 0.38–0.83; p=0.004). However, CV death (HR, 0.56; 95% CI, 0.19–1.70; p=0.29) or all-cause mortality (HR, 1.40; 95% CI, 0.63–3.00; p=0.43) rates did not differ between the 2 groups.3) Similarly, previous small sized RCTs did not show mortality benefit from CR strategy.22)23)
The findings from our study were consistent with those seen in previous RCTs. Overall, the CR was associated with a better composite of CV death, non-fatal MI, TLR, and HF (adjusted HR, 0.64; 95% CI, 0.407–0.996; p=0.04). In addition, although the previous three RCTs revealed a lack of reduction in CV death using the CR strategy, our study demonstrated that CR use was related with a significant reduction in CV death (adjusted HR, 0.57; 95% CI, 0.329–0.971; p=0.03). The subgroup analyses suggested that CR strategy was correlated with benefits of MACE in all subgroup. Especially, those of age >60 or Killip class II–IV were independent predictors of reduction of MACE and CV death.
The enrolled patients in our study have a few differences from those in the previous RCTs. First, we enrolled many more high-risk patients, 27% had Killip class II–IV and 47% had a LAD culprit lesion versus <10% with Killip class II–IV and around 33% with a LAD culprit lesion in previous studies. In addition, one of four patients revealed moderate LV systolic dysfunction (ejection fraction <40%). Most RCTs did not include cardiogenic shock patients. For example, if we exclude patients with Killip IV in our study, the incidence of MACE (11.3%) and CV death (5.9%) in our study is not much higher than in previous studies. That could, to some extent, account for the higher MACE and CV death rates especially in early period of our study.
Second, immediate CR was performed in 69% of patients versus staged-CR in 31% during the index admission. Regardless of CR strategy, both immediate CR and staged-CR were associated with better outcomes than culprit-only PCI. Staged-CR was preferred in patients who did not obtain final TIMI III flow and had a LAD culprit. We assumed that immediate CR would be performed in relatively stable patients. If the patient was unstable, staged-CR would be used, and choosing the CR strategy according to patient characteristics may lead to better outcomes. In terms of CR strategy, the staged-CR group was correlated with a trend toward better outcomes compared with the immediate-CR group especially in CV death. The recent study confirmed that routine immediate-CR lead to bad prognosis than culprit only or staged-CR in STEMI with cardiogenic shock24) and NSTEMI with high CV risk.25) They suggested that the higher dose of contrast that was used during immediate-CR may have led to negative effect on myocardial function and recovery. In addition, delayed procedure time of immediate-CR may be bad at a time when the patients were unstable. In our study many of hemodynamically compromised patients were also included; consequently staged-CR may be correlated with better prognosis compared with immediate-CR.
Third, we enrolled a larger number of STEMI and MVD patients (705 patients) who underwent PCI using only 2nd generation DES during the index admission. EES and ZES, both of which have validated efficacy and safety, were used in approximately 65% of the enrolled patients, while BD-DES was used in 12% of patients. The new-generation DES with more biocompatible polymers may reduce fatal events in patients with STEMI. These differences from previous RCTs explain the significant difference in CV death at 1-year of follow-up.
Our study has 2 main limitations. First, as an observational study, many confounders not adjusted by regression analysis would contribute to each of the composite endpoints. Second, there were insufficient data regarding coronary lesion characteristics and procedure details that could have influenced the decision to use CR or culprit-only PCI. In addition, the procedure was performed according to the judgment of operation in the treatment of non-culprit lesions, and lack of information on functional assessment or the result of additional imaging study.
In conclusion, use of the CR strategy might be associated with a marked reduction in MACE and even CV death among STEMI and MVD patients who underwent PCI using 2nd generation DES. Additionally, staged CR showed a trend of better outcomes than immediate CR.
 XML Download
XML Download