

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Ovarian cancer is the 5th leading cause of death due to cancer in the United States, with an estimated 22,000 new cases developing annually [1]. Proper staging is important for treatment planning and assessing prognosis. Ovarian cancer staging is surgical and based on surgical and pathologic findings; no imaging modality provides conclusive ovarian cancer staging [2]. However, pre-treatment imaging studies are important because their findings help determine the surgical approach or help assess optimal cytoreduction feasibility [3]. They can help with selecting candidates for neoadjuvant treatment. Although 18F-fluorodeoxyglucose (18F-FDG) positron emission tomography/computed tomography (PET/CT) is not recommended for the routine staging of ovarian cancer [4], it can provide additional information before surgery about disease extension and the resection possibility. A comprehensive review of available literature has indicated that 18F-FDG PET/CT has comparable or higher diagnostic accuracy in the staging and pre-treatment evaluation of ovarian cancer than CT and magnetic resonance imaging [567891011121314]. 18F-FDG PET/CT findings can enhance ovarian cancer staging, largely because of the detection of supra-diaphragmatic metastasis [15].
In recent years, many studies on the utility of pre-treatment 18F-FDG PET/CT have been published. However, differences in study population, design, and methodologic quality between studies have made it difficult to draw evidence-based conclusions. We therefore performed a systematic review and meta-analysis to evaluate the performance of 18F-FDG PET/CT in detecting metastasis in ovarian cancer as a staging imaging modality.
MATERIALS AND METHODS
This meta-analysis adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [16]. A priori study protocol is given in the Supplemental Material.
1. Search strategy and study selection
A systematic search of MEDLINE and Embase was performed for articles published before November 9, 2017. Search queries included synonyms and related terms for ovarian cancer, PET, initial staging, and diagnostic accuracy as follows: (“ovarian cancer” OR “ovarian carcinoma” OR “ovarian neoplasm” OR “ovarian tumor” OR “ovarian tumour”) AND (PET OR Positron) AND (preoperative OR pretreatment OR primary OR “lymph node” OR nodal OR “peritoneal carcinomatosis” OR “peritoneal seeding” OR distant OR metastasis OR metastases OR staging OR stage) AND (detection OR detectability OR detecting OR positivity OR sensitivity OR specificity OR diagnosis OR diagnostic OR accuracy OR performance). Reference lists of identified articles were checked to find additional relevant papers. No language restriction was placed. The following inclusion criteria were applied: patients with clinically suspected or newly diagnosed ovarian cancer; 18F-FDG PET or PET/CT used as the index test for detecting metastasis; surgical findings used as the reference standard; and sufficient information available to enable 2×2 tables to be reconstructed for diagnostic accuracy. Non-original articles were excluded. When 2×2 tables could not be reconstructed, authors were contacted. Two reviewers independently performed the literature search and selection, and any disagreement was resolved by discussion.
2. Data extraction and quality assessment
A standardized form was used to extract patient, tumor, study, and 18F-FDG PET/CT characteristics from included articles. Histological subtypes were reclassified according to the new World Health Organization classification [17]. Serous, endometrioid, and undifferentiated subtypes were regarded as FDG-avid [1819]. The methodologic quality of included studies was assessed using Quality Assessment of Diagnostic Accuracy Studies-2 [20]. Two independent reviewers performed data extraction and quality assessment, with any disagreement resolved by discussion.
3. Data synthesis
Two-by-two tables were tabulated from included articles. One article provided per-patient and per-site analyses; the latter, which is more informative for treatment planning, was selected [7]. Metastasis at each site (i.e., omentum, mesentery, bowel, peritoneal cavity) was evaluated as positive or negative regardless of its numbers in the per-site analysis. Pooled sensitivity, specificity, positive likelihood ratio (PLR), and negative likelihood ratio (NLR) were calculated using hierarchical methods, including bivariate and hierarchical summary receiver operating characteristic (HSROC) models [21]. Publication bias was assessed using Deeks' funnel plot asymmetry test [22].
Heterogeneity was assessed by Higgins I2 statistic. [23]. To explore the possible presence of threshold effect, Spearman's rank correlation between sensitivity and false-positive rate was calculated. Sensitivity analyses using several covariates were performed to explore potential causes of heterogeneity.
The clinical application of 18F-FDG PET/CT was examined by pooling likelihood ratios and using them with Fagan's nomogram to generate the post-test probability for metastasis [24]. The estimated pre-test probability for detecting metastasis was based on prevalences of regional and advanced metastases of 20% and 60%, respectively [25].
Stata 10.0 (StataCorp LP, College Station, TX, USA) and R version 3.4.2 (R Foundation for Statistical Computing, Vienna, Austria) were used for statistical analyses. The p values of <0.05 were regarded as statistically significant.
RESULTS
1. Literature search
The study selection process is depicted in Fig. 1. The initial literature search yielded 1,076 articles. After removing 289 duplicates, screening of the remaining 787 titles and abstracts yielded 32 potentially eligible original articles. After performing full-text reviews, 24 were excluded. Thus, eight studies met our pre-defined criteria and were included [56789102627]. These studies included 594 patients.

2. Study characteristics
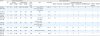
Table 1 summarizes patient and tumor characteristics, and Table 2 describes study characteristics. Five studies used laparotomy as the reference standard, whereas three included diagnostic laparoscopy. Seven studies confirmed surgical findings by histopathologic evaluation. The analysis level of metastatic lesions was per-site in all included studies. Peritoneal metastases were evaluated in seven studies, retroperitoneal lymph node (RPLN) metastases in six, and distant metastases in three. PET/CT characteristics are shown in Supplementary Table 1. Six studies used hybrid PET/CT scanners, one included a stand-alone PET scanner, and one used only a stand-alone PET scanner.
Table 1
Patient and tumor characteristics
| Author | Patient characteristics | Tumor characteristics | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| No. | Age (yr) | CA‒125 (U/mL) | Total lesions (No.) | Size | FIGO stage | Histologic subtype (No.) | ||||||||||
| Mean | Range | Mean | Range | Serous | Mucinous | Endometrioid | Clear cell | Transitional | Undifferentiated | Mixed epithelial | Others† | |||||
| De Iaco et al. [26] | 40 | 65 | 46–78 | 1,342.3 | 26–6,000 | 346 | 5 mm: 37.5% | IIIB–IV | 14 | 0 | 8 | 2 | 0 | 16 | 0 | 0 |
| 5 mm–5 cm: 10.6% | ||||||||||||||||
| >5 cm: 37.5% | ||||||||||||||||
| Hynninen et al. [10] | 41 | 65* | 45–79 | NR | NR | 693 | NR | IC–IV | 37 | 1 | 1 | 1 | 0 | 1 | 0 | 0 |
| Kitajima et al. [9] | 40 | 55.4 | 38–77 | NR | NR | 680 | 4.5±1.1 | IA–IV | 15 | 7 | 5 | 7 | 0 | 6 | 0 | 0 |
| Michielsen et al. [6] | 32 | 61.9 | 20–83 | NR | NR | 594 | <1 cm: 37.5% | IA–IV | 22 | 1 | 0 | 0 | 0 | 0 | 0 | 9 |
| >1 cm: 29% | ||||||||||||||||
| Confluent: 35% | ||||||||||||||||
| Schmidt et al. [8] | 15 | 65 | 31–89 | NR | NR | 195 | ≤5 mm: 17% | NR | 7 | 1 | 3 | 1 | 0 | 3 | 0 | 0 |
| 5 mm–5 cm: 54% | ||||||||||||||||
| >5 cm: 29% | ||||||||||||||||
| Shim et al. [27] | 343 | 55* | 20–80 | 715 | 4–123,000 | 1,029 | NR | IIIA–IV | 274 | 5 | 24 | 22 | 10 | 0 | 0 | 8 |
| Signorelli et al. [7] | 68 | 49* | 35–72 | NR | NR | 517 | 9.0 mm* (4–41 mm) | IA–IIIC | 29 | 6 | 13 | 10 | 0 | 3 | 7 | 0 |
| Yoshida et al. [5] | 15 | 60.4 | 34–89 | NR | NR | 240 | NR | IA–IIIC | 8 | 3 | 2 | 0 | 0 | 1 | 0 | 1 |
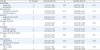
Table 2
Study characteristics

| Author | Publication year | Origin | Design | Reference standard | Readers | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Period | Country | Institution | Prospective | Multicenter | Patient selection | Consecutive enrollment | Method | Pathologic evaluation | PET-reference interval (days) | Analysis level | Site | No. | Experience (yr) | Interpretation | Blinded | ||
| De Iaco et al. [26] | 2011 | 2004.09–2008.04 | Italy | Azienda Ospedaliero-Universitaria di Bologna | No | No | Clinically suspected | NR | Diagnostic LPS | No | NR | Per-site | PC | NR | NR | SUVmax >2 g/ml | NR |
| Hynninen et al. [10] | 2013 | 2009.10–2012.03 | Finland | Turku University Hospital | Yes | No | Clinically suspected | Yes | Laparotomy or Diagnostic LPS | Yes | ≤14 | Per-site | PC, RPLN | 2 | NR | Visual | Yes |
| Kitajima et al. [9] | 2008 | 2006.04–2008.04 | Japan | Dokkyo University School of Medicine | No | No | Clinically suspected | Yes | Laparotomy | Yes | ≤14 | Per-site | Contralateral ovary, PC, RPLN, liver, lung | 2 | 3/5 | Visual | Yes |
| Michielsen et al. [6] | 2014 | 2010.10–2012.02 | Belgium | University Hospitals Leuven | Yes | No | Clinically suspected | Yes | Laparotomy or diagnostic LPS | Yes | NR | Per-site | PC, RPLN | 1 | 11 | Visual | Yes |
| Schmidt et al. [8] | 2015 | NR | Switzerland | Lausanne University Hospital | Yes | No | Clinically suspected | Yes | Laparotomy | Yes | ≤29 | Per-site | PC, RPLN, pleural carcinomatosis | 1 | 10 | Visual | Yes |
| Shim et al. [27] | 2015 | 2006.01–2013.08 | South Korea | Asan Medical Center | No | No | Pathologically confirmed | Yes | Laparotomy | Yes | ≤28 | Per-site | PC | NR | NR | Visual | Yes |
| Signorelli et al. [7] | 2013 | 2006.01–2012.05 | Italy | San Gerardo Hospital | Yes | No | Pathologically confirmed | Yes | Laparotomy | Yes | ≤30 | Per-site | RPLN | 2 | NR | Visual | Yes |
| Yoshida et al. [5] | 2004 | 2001.09–2002.07 | Japan | Fukui Medical University | No | No | Clinically suspected | NR | Laparotomy | Yes | 14 | Per-site | Contralateral ovary, PC, RPLN, liver, lung | NR | NR | Visual | Yes |
3. Quality assessment
Supplementary Fig. 1 summarizes quality assessment results. One study had an unclear risk of bias in the patient selection domain because it was unclear whether consecutive patients were enrolled [26]. The same study had a possible risk of bias in the index test as it was unclear whether the index test was interpreted without knowledge of the reference standard [26]. Regarding the reference standard domain, three studies showed a high risk of bias because they used laparoscopy as the reference standard [61026], and there was an unclear risk of bias in three further studies for which it was unclear whether reference standard interpretation was blinded to index test results [5827]. In 2 studies, there was an unclear risk of bias in the flow and timing domain because the time interval between the PET/CT scan and reference standard was not provided [626].
There was low concern for applicability in the patient selection domain for all but two studies: one included only patients with advanced (stage III/IV) ovarian cancer [27] and the other excluded patients with abdominal dissemination [7]. There was high concern for applicability in the index test domain for 2 studies that included the PET only image results interpreted with enhanced CT scans [56]. For all studies, concern for applicability in the reference standard domain was low.
4. Diagnostic accuracy and heterogeneity assessment
Across all eight included studies, the pooled sensitivity and specificity of 18F-FDG PET/CT for identifying the presence of metastasis were 0.72 (95% confidence interval [CI]=0.61–0.81) and 0.93 (95% CI=0.85–0.97), respectively (Fig. 2). The pooled PLR and NLR were 10.5 (95% CI=4.5–24.5) and 0.30 (95% CI=0.20–0.44), respectively. The area under the HSROC curve was 0.89 (95% CI=0.86–0.91) (Supplementary Fig. 2). Higgins I2 statistic demonstrated considerable heterogeneity in sensitivity (I2=97.57%) and specificity (I2=96.74%). No threshold effect was observed (ρ=−0.003). The Deeks funnel plot suggested the presence of publication bias, with a p value of 0.08 (Supplementary Fig. 3).

5. Heterogeneity exploration
Sensitivity analysis results are presented in Table 3. Sensitivity and specificity estimates were significantly higher in studies that used laparotomy as the reference standard than in those that included diagnostic laparoscopy (sensitivity: 0.77; 95% CI=0.67–0.87 vs. 0.62; 95% CI=0.46–0.77; p=0.02; specificity: 0.96; 95% CI=0.92–0.99 vs. 0.84; 95% CI=0.69–0.99; p=0.01). Specificity estimates were significantly higher in studies that confirmed surgical findings by pathologic evaluation than in the study without histopathologic confirmation (0.95; 95% CI=0.90–0.99 vs. 0.69; 95% CI=0.24–1.00; p=0.03). Studies with a greater proportion (≥70%) of the FDG-avid subtype showed lower specificity than those with a lower proportion (<70%) (0.89; 95% CI=0.80–0.97 vs. 0.97; 95% CI=0.94–1.00). There were no significant differences in sensitivity and specificity estimates with regard to the International Federation of Gynecology and Obstetrics (FIGO) stage, scanner type, or PET interpretation method. However, pooled estimates for these subgroups were considered unstable because only 1 or 2 studies were included in each subgroup.
Table 3
Sensitivity analysis results
CI, confidence interval; CT, computed tomography; FDG, fluorodeoxyglucose; FIGO, International Federation of Gynecology and Obstetrics; LPS, laparoscopy; PET, positron emission tomography; SUVmax, maximum standardized uptake value.
*FIGO stages I and II were regarded as early stage; †The FDG-avid subtype comprised serous, endometrioid, and undifferentiated tumors.
6. Subgroup analysis and clinical application
Subgroup analyses were performed for detecting peritoneal carcinomatosis (PC) and RPLN metastasis. Subanalysis for PC included data from seven studies with 526 patients. The pooled sensitivity and specificity were 0.70 (95% CI=0.56–0.82) and 0.90 (95% CI=0.82–0.94), respectively, and the pooled PLR and NLR were 7.0 (95% CI=3.7–13.2) and 0.33 (95% CI=0.21–0.52), respectively. The area under the HSROC curve was 0.89 (95% CI=0.86–0.91). Subanalysis for RPLN metastasis included 6 studies with 211 patients. The pooled sensitivity and specificity were 0.77 (95% CI=0.61–0.87) and 0.97 (95% CI=0.93–0.99), respectively, and the pooled PLR and NLR were 28.5 (95% CI=10.5–77.2) and 0.24 (95% CI=0.13–0.43). The area under the HSROC curve was 0.95 (95% CI=0.92–0.96). The subgroup analysis for detecting distant metastasis was not performed because of the paucity of studies.
At a pre-test probability of 20%, a positive result for RPLN metastasis remarkably increased the post-test probability (88%), whereas a positive result for PC moderately increased the post-test probability (63%) (Fig. 3). At a pre-test probability of 60%, positive results for PC and RPLN metastases increased the post-test probability by up to 91% and 98%, respectively. Negative results for these conditions moderately reduced the post-test probability to 33% and 26%, respectively.

DISCUSSION
We evaluated the performance of pre-treatment 18F-FDG PET/CT as a staging modality for detecting metastasis in ovarian cancer. Previous meta-analyses investigating the role of 18F-FDG PET/CT in ovarian cancer focused on diagnosing recurrent disease [28] or detecting metastasis in a mixed primary/recurrent population [429]. The present meta-analysis provided a comprehensive overview of literature, explored the causes of heterogeneity, and investigated the clinical application of the staging performance of 18F-FDG PET/CT in practice. The sensitivity and specificity of 18F-FDG PET/CT for revealing metastasis, pooled across the eight included studies, were 0.72 (95% CI=0.61–0.81) and 0.93 (95% CI=0.85–0.97), respectively.
There was considerable heterogeneity among the included studies. Comprehensive sensitivity analyses provided some insight into the potential causes of heterogeneity. Studies that used laparotomy as the reference standard showed significantly higher sensitivity and specificity than those that included diagnostic laparoscopy. There has been no conclusive evidence that laparoscopic staging is comparable to standard surgical staging by laparotomy in either the advanced disease or apparent early stage ovarian cancer [30]. With laparoscopy, it can be difficult to assess some abdominal regions, including the retrohepatic area, hepatophrenic junction, and porta hepatis [31]. Tumor deposits at the peritoneal folding and in the subdiaphragmatic space can be missed because laparoscopy lacks the tactile sense [32]. Biopsy under laparoscopy is technically demanding and occasionally unsuccessful because of adhesions or unsatisfactory exposure [33]. Some FDG-avid lesions may be missed due to technical problems, leading to false-positive results and thus low specificity. There was a significant difference in specificity estimates between studies with and those without histologic surgical specimen evaluations. This difference may be attributable to a study [26] that used only diagnostic laparoscopy as the reference standard and showed a much lower specificity (0.69) than other studies. The low sensitivity in studies that included laparoscopy was difficult to explain because there may have been more false-negative cases in the setting of laparotomy. One explanation could be that laparoscopic staging was preferentially performed in early stage ovarian cancer, thus leading equivocal 18F-FDG PET/CT findings to negative.
It is well known that FDG-avidity is important for the diagnostic accuracy of 18F-FDG PET/CT. Studies with a lower prevalence of the FDG-avid subtype showed higher specificity than those with a greater prevalence. A possible partial explanation is that interpretations are prone to be negative under the assumption that a primary lesion is FDG-non avid. Sensitivity was higher in studies with a greater prevalence of the FDG-avid subtype, but this difference was not statistically significant because of the wide confidence interval as a result of pooling three studies with low prevalence.
Lesion size is another well-known factor that affects the diagnostic accuracy of 18F-FDG PET/CT. Although positive correlations between lesion size and PET positivity have been reported [7926], sensitivity analysis with regard to lesion size was not possible because the type of description for size varied (mean ± standard deviation, median value with range, and classification into categorized values). Further studies are needed to clarify this issue. In addition, the numbers of patients and lesions varied among the included studies, which may be explained by the differences in the FIGO stage, extent of surgery, and image analysis methods. These discrepancies could result in heterogeneity.
Our analysis showed that pre-treatment 18F-FDG PET/CT provided moderate sensitivity and high specificity for detecting metastasis in ovarian cancer. The likelihood ratios and post-test probabilities provided information relevant to clinicians. For instance, at a pre-test likelihood of 60%, which is the probability of unknown patients having advanced disease, PET-positive results of both PC and RPLN metastasis increased post-test likelihood to >90%. Test positivity of 18F-FDG PET/CT provided a reliable estimate to clinicians for the risk of lymph node metastasis. The use of 18F-FDG PET/CT moderately improved the probability of PC. Depending on its location, a test-positive lesion may require a modified surgical approach or can be interpreted as a resectable condition that may require surgical subspecialty expertise (such as hepatic metastasis, implant near the hepatic vein, or bowel implant) or a potentially non-resectable condition (such as mesenteric root involvement or suprarenal lymph node metastasis) with a low false-positive rate of 18F-FDG PET/CT [3]. However, surgical staging is still required because the possibility of a false-negative result cannot be overlooked. The detection of distant metastasis is another important role of 18F-FDG PET/CT for accurate staging. In general, 18F-FDG PET/CT has been known to be effective for the identification of distant metastases at pretreatment evaluation in patients with ovarian cancer [34]. However, we could not provide meta-analytically pooled estimates for detecting distant metastasis because only three of the included studies evaluated distant metastasis.
There were limitations to this meta-analysis. Only eight studies were included. A systematic search of the literature without language restrictions could only identify 8 studies for evidence synthesis. Nevertheless, the meta-analysis provides a general overview of the currently available literature on this topic. Further, there was considerable heterogeneity in the pooled analysis, suggesting a need for exercising caution in applying summary estimates more generally. The type of reference standard used, use of histopathologic confirmation, and prevalence of the FDG-avid subtype may explain some of the heterogeneity, but part remains unexplained. Additionally, our pooled results were site-based, making them prone to overestimation compared with those from a per-lesion analysis. Nevertheless, none of the included studies provided a lesion-based analysis because the head-to-head comparison of surgical and PET/CT findings is not realistically feasible. Finally, publication bias affected included studies; studies with no significant or unfavorable results are more likely to be discarded. It is therefore possible that the diagnostic performance of 18F-FDG PET/CT was overestimated in this meta-analysis.
In conclusion, pre-treatment 18F-FDG PET/CT showed moderate sensitivity and high specificity for detecting metastasis in ovarian cancer. With its low false-positive rate, 18F-FDG PET/CT can help decide the selection of surgical approaches or alternative treatment options. However, surgical staging is required even with negative results because of the considerable false-negative rate.
 XML Download
XML Download