

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Women undergoing hysterectomy for cervical cancer (CC) and found to have positive surgical margins, positive lymph nodes, and/or parametrial invasion (the so-called “3 Ps”) achieve a survival benefit with adjuvant concurrent chemotherapy (CT) and pelvic radiation therapy (RT) over RT alone [1]. In a landmark trial, Peters and colleagues [1] found that clinical stage IA2, IB, and IIA patients with any of the three aforementioned risk factors experienced improved progression-free survival (PFS) and overall survival (OS) with the addition of CT to definitive pelvic RT following radical hysterectomy. Although there was no association between age and survival, most patients were quite young (median 38 and 41 years for the RT+CT and RT arms, respectively).
Due to the presence of underlying comorbid conditions that lead to greater treatment related toxicity as well as increased risk of death from non-oncologic causes, the elderly population represents unique challenges for oncologic management. Although less than 15% of all patients with CC are older than 65 years at diagnosis, these elderly patients comprise a large population, at an estimated 40,000 women in the United States [2]. In addition to a reduced life expectancy (thus potentially receiving comparatively less benefit from aggressive oncologic interventions), elderly patients are also more susceptible to treatment-related toxicities [13456]. It is thus unknown whether elderly women should be aggressively treated similar to their younger counterparts, or whether single-modality adjuvant therapy would provide similar survival. It is unlikely that dedicated phase III trials addressing this question would ever take place, given the age distribution of CC as well as the well-known under-representation of older patients on clinical trials [789101112].
To address this knowledge gap, the goal of this investigation, the first of its kind, was to evaluate postoperative chemoradiotherapy (CRT) vs. RT alone for elderly (≥70 years old) women with positive surgical margins, positive lymph nodes, and/or parametrial invasion.
MATERIALS AND METHODS
This study retrospectively analyzed the National Cancer Database (NCDB), a jointly sponsored database by the Commission on Cancer (CoC) of the American College of Surgeons (ACS), and the American Cancer Society. Data includes de-identified information regarding treatments and outcomes from over 29 million cancers and approximately 70% of all malignant cancers diagnosed at CoC-accredited facilities within the United States [13]. Review from an internal review board was not required because the NCDB is exclusively comprised of de-identified information.
1. Patient selection
Deidentified data for patients in the NCDB from 2004–2013 were included in this dataset. Inclusion criteria were patients ≥70 years of age with newly diagnosed IA2, IB, or IIA cervical cancer treated definitively with upfront surgery and either positive margins, parametrial invasion, or positive nodes found on pathology. This patient population was selected to allow direct comparison to historical trials [1]. The 70-year-old threshold was used because this is a commonly used cutoff to analyze “elderly” patients [1415].
Patients were excluded if <70 years of age, M1 or unknown M stage, clinically stage IA1, IIB+ or unknown stage, no hysterectomy or unknown surgical status, no/unknown adjuvant RT, or unknown CT status. Collected information on each patient broadly included demographic data, clinicopathologic parameters, and treatment data.
Median follow up was calculated using the reverse Kaplan-Meier method [16]. All statistical tests were 2-sided, with a threshold of p<0.05 for statistical significance, and were analyzed using IBM SPSS Statistics (version 24; IBM Corp., Armonk, NY, USA). Multivariable logistic regression modeling was utilized to identify characteristics that were predictive for receipt of CRT. The Kaplan-Meier method was used for survival analysis, and comparisons between groups were compared with log-rank test. OS was defined as the interval between date of diagnosis and death, or censored at the date of last contact. Univariate and multivariate Cox proportional hazard analysis was performed to determine factors associated with OS.
RESULTS
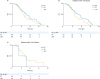
There were 98,347 patients in the NCDB CC database (Fig. 1), of which 166 met the pre-specified inclusion criteria. Table 1 displays the clinical characteristics of those patients, 62 of whom underwent RT alone (37.3%) and 104 underwent CRT (62.7%). Multivariable analysis revealed that increasing age (as a continuous variable) and higher zip-code level income (≥$30,000) (p<0.05 for all) were associated with decreased likelihood of CRT delivery (Table 2). Parametrial invasion (p=0.037), nodal involvement (p=0.003), and later years of diagnosis (2009 or after) (p=0.004) were significantly related with increased likelihood of CRT receipt, while positive surgical margins were not (p=0.963).
 | Fig. 1Patient selection diagram.3 Ps, positive surgical margins, positive lymph nodes, and/or parametrial invasion; CC, cervical cancer; CRT, chemoradiotherapy; NCDB, National Cancer Database; RT, radiation therapy.
|
Table 1
Baseline characteristics

Values are presented as number (%) or median (range)
CRT, chemoradiotherapy; EBRT, external beam radiation therapy; FIGO, International Federation of Gynecology and Obstetrics; RT, radiation therapy.
*Parenthesis value of ‘Radiation dose’ are interquartile range.
![]()
Table 2
Multivariable logistic regression analysis evaluating predictors of receiving CRT

Statistically significant p-values (p<0.05) are in bold.
CI, confidence interval; CRT, chemoradiotherapy; EBRT, external beam radiation therapy; FIGO, International Federation of Gynecology and Obstetrics; OR, odds ratio; RT, radiation therapy.
![]()
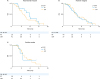
The median follow-up was 35.3 months (interquartile range=20.7–52.3 months). Kaplan-Meier estimates comparing OS in patients that received postoperative RT alone vs. CRT revealed no significant differences, with corresponding median OS times of 56.1 (95% confidence interval [CI]=36.1–76) months and 43.5 (95% CI=36.3–50.6) months, (p=0.314), respectively (Fig. 2A).
 | Fig. 2Kaplan-Meier curve of OS for (A) patients who received RT vs. CRT and OS stratified by (B) 1 risk factor and (C) 2 or more risk factors.CRT, chemoradiation therapy; OS, overall survival; RT, radiation therapy.
|
On univariate analysis, there were several variables predictive of OS: higher education, higher income, urban residence (relative to metro), and later years of diagnosis (Table 3). Of these, only year of diagnosis (2009–2013 vs. 2004–2008) remained a significant predictor of OS on multivariate analysis (hazard ratio [HR]=15.75; 95% CI=5.49–45.24; p<0.001). Other factors predictive of worse OS in the multivariate model were mixed/other histology (relative to squamous cell carcinoma) (HR=3.81; 95% CI=1.18–12.28; p=0.025) and treatment at an academic (vs. community) center (HR=2.47; 95% CI=1.16–5.25; p=0.019), while International Federation of Gynecology and Obstetrics (FIGO) stage IA (relative to IB) was associated with improved OS (HR=0.02; 95% CI=0.01–0.22; p=0.025, Table 3).
Table 3
HRs determined by univariate and multivariate Cox proportional hazards model adjusted for covariates

Statistically significant p-values (p<0.05) are in bold.
CI, confidence interval; CRT, chemoradiotherapy; EBRT, external beam radiation therapy; FIGO, International Federation of Gynecology and Obstetrics; HR, hazard ratio; RT, radiation therapy.
![]()
To further explore potential patients at increased risk of death, patients were stratified by 1 vs. 2 or more risk factors (parametrial invasion, positive surgical margins, or positive lymph nodes). There were no statistically significant differences in OS between CRT and RT alone in patients with 1 vs. 2 or more risk factors (Fig. 2B and C), nor were there any differences in OS when directly comparing 1 vs. 2 or more risk factors (Supplementary Fig. 1). Stratification by specific risk factors (parametrial invasion, positive margins, positive nodes; Fig. 3A, B, and C, respectively) similarly showed no differences in OS between CRT vs. RT alone.
DISCUSSION
To the best of our knowledge, this is the largest known report assessing patterns of care and outcomes for elderly women with CC receiving either postoperative CRT or RT for positive surgical margins, positive lymph nodes, and/or parametrial invasion. Our study of a large, contemporary national database did not discern an additional OS benefit in combined-modality adjuvant therapy in the elderly CC patient population. As such, clinicians must continue to weigh the benefits of adjuvant CRT with additive toxicities associated with concurrent CT administration.
Similar survival outcomes between treatment groups may in part be attributed to only well-selected elderly patients with risk factors and comorbidities incompletely captured by the NCDB. Although the NCDB does not capture details such as cancer-related survival, PFS, and local/regional recurrence, there are several reasons this selection bias is unlikely. First, there were similar baseline characteristics between treatment groups, including Charlson/Deyo comorbidity score (which is acknowledged is not synomymous with performance status), decreasing the likelihood of selection bias. Second, there were only three non-socioeconomic characteristics significant on multivariable logistic regression analysis that predicted for CRT use: age, parametrial invasion, and nodal involvement. Nonetheless, age and socioeconomic factors have been shown to be independent predictors of undertreatment and mortality in cervical cancer [17181920], possibly contributing to selection bias within our study population. With this in mind, it is important to note that our results certainly do not imply causation.
While 2 of the “3 Ps” (parametrial invasion and positive nodes) were associated with increased likelihood of CRT, positive surgical margins were not. This may be due to positive surgical margins possibly being the most “localized” and thus decreasing the necessity of additional systemic therapy in addition to RT. It is also plausible that the patients with positive surgical margins received brachytherapy (38% and 10% in the RT and CRT groups, respectively) in place of CT.
Our results suggest that elderly patients, who are at risk of death from competing causes, may not receive as high of a benefit to additional postoperative CT, regardless of the number or type of risk factors. In a smaller single institution retrospective analysis, researchers similarly found no differences in survival by age groups [21]. Of note, the study also examined toxicity events and found no differences in toxicity rates among age cohorts receiving CRT. Similar lack of survival and toxicity differences have been reported in populations with relatively heterogeneous stages and/or treatments [2223242526], but no studies to date, to our knowledge, have exclusively evaluated outcomes of elderly patients receiving postoperative RT vs. CRT.
The strengths of our study include a well-defined population from the validated NCDB, allowing for robust statistical analyses. However, although the NCDB provides a unique opportunity to study this important clinical question, this study did have some weaknesses that are inherent to all retrospective and/or NCDB analyses. First, selection and lead time bias are always a concern in retrospective studies. Second, as previously mentioned, toxicity data is not recorded within the NCDB. Third, the NCDB does not record details of CT, including agent, duration of treatment, dosage, number of cycles, and reasons for withholding CT. Fourth, the NCDB does not provide data on performance status, number of positive lymph nodes and degree of involvement therein, degree of positive surgical margins (e.g., grossly vs. microscopically positive), and the degree of parametrial invasion. Based on this lack of data, it is likely that the CRT group was, as a whole, “higher” risk and thus warranted receipt of CT. Thus, it remains possible that these patients may have achieved a benefit from additional CT, though the magnitude of this benefit may not have been enough to overcome the potential for selection bias favoring the RT alone cohort. Lastly, the small sample size of this study severely limited the power of subgroup analysis, making it difficult to draw any definitive conclusions. Due to this prohibitively small sample size and similar characteristics between groups, propensity matching could not be reliably performed.
Another important consideration not fully captured by the NCDB is radiation therapy technique. There is some prospective evidence that suggests intensity modulated radiation therapy (IMRT) may lower toxicity over 3-dimensional conformal radiotherapy (3D CRT) [2728]. In a phase III multicenter randomized controlled trial, patients with cervical or endometrial cancer were randomized to receive either traditional RT or IMRT. The IMRT group had significantly less gastrointestinal and urinary toxicity compared to the conventional RT group [27]. In a phase 2 trial, researchers reported that pelvic IMRT resulted in acceptably low hematologic toxicity rates in cervical cancer patients receiving postoperative chemoradiation therapy [28]. Together, these trials highlight the importance of radiation therapy technique in consideration of outcomes and a limitation of our NCDB analysis that warrants evaluation with prospective trials.
 XML Download
XML Download