

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Brain tumors have a very high likelihood of causing long-term disabling effects due to the tumor itself and treatment-related factors, including surgical complications, neurotoxic radiation effects, and debility caused by chemotherapy [1]. Patients with brain tumors frequently experience a combination of physical, cognitive, and communication deficits [2] and can achieve functional gains equivalent to those achieved by patients with stroke and traumatic brain injury in a conventional inpatient rehabilitation setting [3].
Physical therapists typically conduct one-on-one treatment sessions; however, given the heavy burden on therapists and the limited treatment time available, it is difficult to satisfy patient needs and perform effective rehabilitation therapy. Compared with conventional treatment, robot-assisted gait training (RAGT) with conventional therapy improved walking ability with intensive training [4]. Rehabilitation robotics allow a greater number of treatment cycles and reduce the burden on therapists [5]. Furthermore, RAGT may improve walking ability by accelerating neuroplastic processes [6]. In a Cochrane review, Mehrholz et al. [7] found moderately strong evidence that RAGT devices can improve gait after stroke. However, no validated evidence on the efficacy of RAGT in patients with brain tumors is available. This study aimed to investigate the effects of RAGT in patients with brain tumors, with Morning Walk® (Fig. 1), which is an end-effector type rehabilitation robot for lower limb rehabilitation.

Morning Walk® is an end-effector type robot, in which used for lower limb rehabilitation, ankle, knee, and pelvic movements are enabled by footplate trajectories [8]. Patients can be boarded safely on saddle that supports the patient's weight and provides stability. Thus, Morning Walk® has the advantages of relatively short working time and no harnesses, which enables easy boarding and landing. Additionally, various training techniques, including ground walking and ascending and descending stairs, could help provide effective rehabilitation treatment. To ensure patient safety, the machine is equipped with an upper body safety belt, parallel bars on both sides, and an emergency stop button. The training begins with a casual ground-level gait with a step length of 30–35 cm and a cadence of 30–35 steps/min. The program is adjusted according to the individual's performance, and the training progresses to walking up and down the stairs.
CASE REPORT
The Institutional Review Board of Asan Medical Center approved the study, and all patients were informed about the purpose and procedure of the study before they signed the informed consent form.
Three patients underwent RAGT for 30 minutes per session in combination with 1 hour of conventional physiotherapy, 5 times a week for 3 weeks (i.e., 15 sessions in total). Conventional physiotherapy, which was based on a traditional neurodevelopmental treatment technique, included sitting and standing balance, active transfer, sit-to-stand training, strengthening exercises, dynamic standing balance and functional gait training. Walking ability was assessed using the Functional Ambulation Categories (FAC) scale, and lower limb function was assessed using the Motricity Index (MI) for lower extremities. The 10-meter walk test (10-m WT), Modified Barthel Index (MBI), Rivermead Mobility Index (RMI), Berg Balance Scale (BBS), Karnofsky Performance Status Scale (KPS), and Brief Fatigue Index (BFI) were conducted to analyze post-training patient outcomes.
FAC is a reliable scale for measuring functional gait, and it categorizes patients according to the 6 levels of physical assistance required to maintain gait [9]. MI is a valid tool for evaluating muscular coordination and strength; it ranges from 0 to 100, with higher scores indicating better function of the tested lower limb [10]. The 10-m WT is a commonly used measure of gait velocity. We recorded participants' walking time of 10 minutes over 3 trials and calculated the average velocity (m/s) [11]. MBI (scored from 0 to 100) is a reliable index for measuring activities of daily living and mobility using 10, with higher scores indicating greater independence [12]. RMI (scored from 0 to 15) tests functional abilities and comprises 15 mobility-related items ranging from turning over in bed to running, with higher scores indicating better motor function [13]. BBS (scored from 0 to 56) is a widely used assessment tool for static and dynamic balance [13]. KPS describes a patient's functional status as a comprehensive 11-point scale correlating to percentage values ranging from 100% (no symptoms) to 0% (death) [14]. BFI consists of a 9-item, 11-point rating scale designed to assess the severity and impact of subjective fatigue on daily functioning, over the past 24 hours [15].
The characteristics of individual patients including the location of the brain tumor, treatment, and date of diagnosis are presented in Table 1. Changes in assessment factors before and after the rehabilitation treatment of the 3 cases are presented in Table 2. Adverse events were not reported in all 3 cases.
Table 1
Characteristics of patients with brain tumors

Table 2
Changes in the assessment factors before (T0) and after (T1) the treatment
T0, before the treatment of Morning Walk® with conventional therapy; T1, after the treatment of Morning Walk® with conventional therapy, 5 times a week for 3 weeks; BBS, Berg Balance Scale; BFI, Brief Fatigue Index; FAC, Functional Ambulation Categories; 10-m WT, 10-meter walk test; K-MBI, Korean version of Modified Barthel Index; MI-lower, Motricity Index-lower; RMI, Rivermead Mobility Index.
Case 1
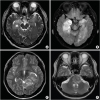
The first case was of a 62-year-old man with high-grade gliomas in the bilateral temporal lobes (Fig. 2A and B). He underwent brain tumor resection and received radiation therapy and drug therapy with temozolomide. After the tumor resection, ambulation required minimal assistance. The patient's muscle strength in both the lower extremities was good with the absence of ataxic features. After 15 sessions of RAGT, the FAC score and MI-lower remained the same. Improvements in the 10-m WT score, Korean version of Modified Barthel Index (K-MBI), RMI, BBS score, and Karnofsky score were observed, but his BFI deteriorated.
Fig. 2
(A) High-grade gliomas in the bilateral temporal lobes. T2-weighted magnetic resonance image of the brain. (B) High-grade gliomas in the bilateral temporal lobes. T2-flair magnetic resonance image of the brain. (C) High-grade glioma (anaplastic pleomorphic xanthoastrocytoma) in the left temporal lobe. T2-weighted magnetic resonance image of the brain. (D) Astrocytoma on the left pons. T2-weighted magnetic resonance image of the brain.
Case 2
The second case was that of a 20-year-old woman with high-grade glioma (anaplastic pleomorphic xanthoastrocytoma) in the left temporal lobe (Fig. 2C). At the time of admission after tumor resection, her muscle strength on right hip flexion was fair, knee flexion was poor, ankle dorsiflexion was trace, and ankle plantar flexion was also fair. Moderate assistance was required for ambulation, and no ataxic features were observed. After 15 sessions of RAGT, the MI-lower remained the same. Outcomes showed improvement in the FAC score, 10-m WT score, K-MBI, RMI, BBS score, and Karnofsky score, but BFI deteriorated.
Case 3
The third case was a 61-year-old man with astrocytoma on the left pons (Fig. 2D). At the time of admission after tumor resection, his muscle strength on the right hip, knee, and ankle was good, and minimal assistance was required for ambulation. After 15 sessions of RAGT, improvements in the FAC score, 10-m WT score, K-MBI, MI-lower, RMI, BBS score, and Karnofsky score were observed, but BFI deteriorated.
Detailed results of BFI deterioration
Among the subcategories, all 3 patients commonly answered that fatigue had interfered with their general activity, walking ability, and normal work (e.g., work outside, daily chores). They also reported difficulty to continue rehabilitation therapy because of increased fatigue after RAGT.
DISCUSSION
To the best of our knowledge, this is the first case series to demonstrate that RAGT together with conventional physiotherapy was beneficial for patients with brain tumors and gait disturbance. Through this study, we verified that RAGT accompanied with conventional physiotherapy is beneficial in managing gait disturbances and results in faster gait, better mobility, and improvement in functional ambulation in patients with brain tumors. Perhaps, Morning Walk® can support weight using a saddle and enable patients to perform continuous and repetitive exercises, so that repetitive exercises can be performed more efficiently at the same time. Some studies have reported that robotic therapy combined with conventional therapy was more effective than conventional therapy alone in patients with greater motor impairment during inpatient stroke rehabilitation [1617]. In a Cochrane review, Mehrholz et al. [7] included 17 trials with a total of 837 patients in this review and found evidence that the use of electromechanical-assistive devices in combination with physiotherapy in rehabilitation settings may improve walking function after stroke.
However, we need to consider the level of fatigue. Fatigue is an important factor affecting treatment continuity in patients with brain tumors. Debilitating cancer-related fatigue produced by both the disease and its treatment [18] is one of the most common adverse effects of cancer [19]. We speculate that this increase in fatigue is caused by the greater intensity of the treatment in robot therapy with conventional treatment. Because conventional treatment is performed one-on-one with the therapist, adjusting the treatment level, such as resting immediately or lowering the intensity of treatment when the patient presents with fatigue. In the robot therapy, although the exercise protocol was adapted to the patient's initial condition, we speculate that the intensity of RAGT reacts less immediately to lower the intensity of exercises when the patients presented with fatigue. The increase in fatigue in patients with cancer is not only unfavorable for cancer treatment [20] but also needs to be adjusted to continue exercise at home after discharge. Through further studies, gaining a deeper insight into the mechanisms underlying fatigue during RAGT is essential for determining therapeutic plans for individual patients.
In conclusion, RAGT combined with conventional physiotherapy improved several outcomes, such as motricity of the affected limb, endurance, functional status, and balance, but the level of fatigue is deteriorated at the same time. If the time, intensity, and protocol of RAGT accompanied with conventional physiotherapy are tailored to the level of fatigue expressed by patients with brain tumors, RAGT accompanied with conventional physiotherapy may be more effective in improving gait disturbances. Further research comprising a larger sample size and randomized controlled studies pertaining to this subject are warranted.
 XML Download
XML Download