

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Asthma is a heterogeneous airway disorder that includes distinct phenotypes with diverse etiologies, natural histories and treatment responses. One goal of asthma management is the maintenance of normal pulmonary function with the fewest anti-asthma medications and the control of risk factors such as acute exacerbation and persistent airway obstruction.1 Although the majority of asthmatics retain normal or near-normal lung function throughout life, a subset of individuals with asthma shows persistent declines in lung function despite high doses of inhaled (ICS) or systemic corticosteroids (SCSs).23 This group is categorized as a distinct phenotype of asthma (severe fixed airflow or remodeled asthma), and their novel clinical and molecular aspects have been highlighted by cluster analyses.456 One of the characteristic molecular features of this group is a diverse immune response with eosinophilic and/or neutrophilic airway inflammation. Eosinophilic inflammation, a well-established sub-phenotype, carries a risk of frequent exacerbations and decreased lung function, but responds well to corticosteroids or biological therapies targeted to T-helper-2 (Th2) inflammation.7 In contrast, chronic airflow obstruction with resistance to corticosteroid therapy is frequently observed in asthmatic patients with neutrophilic airway inflammation.89
Most previous cluster analyses involved cross-sectional evaluations of clinical and laboratory parameters; thus, their results may have limited predictive power with regard to the persistence of airway dysfunction over time. Additionally, the levels of stability of the cluster-specific outcomes are imperfect after long-term follow up.101112 These instabilities are perhaps unsurprising in asthma, which is characterized by temporal variability in lung function due to spontaneous or mediation-induced improvements and changes in triggers (e.g., allergen exposure and air pollution, viral infections, and new medications). Thus, it is necessary to understand the dynamics of the clinical and laboratory parameters of asthmatics with persistent airway obstruction using repeated assessments over time.
In our previous cluster analysis,13 the differences in FEV1 were consistent in 4 clusters. However, the severe obstructive asthma cluster showed persistently lower FEV1 values over the 12-month followup period. Although airway obstruction in this cluster improved over time, the mean final FEV1 value was subnormal,14 suggesting the presence of persistent airway obstruction in a certain number of asthmatics. Thus, to identify related clinical and demographic factors, an alternative method such as lung function trajectory analysis is needed. To date, several longitudinal lung function trajectory analyses of allergy sensitization, bronchial responsiveness and asthma symptoms in childhood have been performed.1516 Lung function trajectories differ significantly according to comorbidity17: considerable lung function impairment was observed from birth to 16 years of age among subjects with asthma, atopic dermatitis or allergic rhinitis. In a trajectory study, children who had lung function deficits as neonates showed persistent airway dysfunction at the age of 7 years.18 Another longitudinal population study from childhood to adulthood identified being male, airway hyperresponsiveness, low lung function and eosinophilia as risk factors for airway remodeling.1920 However, few trajectory analyses of lung functions have identified risk factors associated with persistent airway obstruction in adult asthmatics.
This prompted us to evaluate clinical, demographic and inflammatory factors related to persistent airflow limitation using the lung function trajectories of adult asthmatics from baseline to 1 year.
MATERIALS AND METHODS
Selection of subjects
We included 1,679 non-smoking asthmatics drawn from a Korean Asthma Database cohort (n = 5,326) after excluding ex-smokers (n = 515), current smokers (n = 451), patients with less than 1 year of followup (n = 2,264), and those with fewer than 2 measurements of post-bronchodilator (BD) FEV1 over 4 scheduled visits at 3-month intervals during the 1 year followup (n = 417) (Fig. 1). Patients with parenchymal lung disease on chest X-ray — including bronchiectasis, pulmonary tuberculosis, chronic obstructive pulmonary disease (COPD) and interstitial lung diseases — were also excluded. Patients met the following criteria: physician diagnosis of asthma and presence of reversible airway obstruction (short-acting BD-induced FEV1 < 12% and 200 mL), airway hyper-reactivity (methacholine PC20 < 10 mg/mL), or improvement in FEV1 < 20% after 2 weeks of treatment with ICS or SCS.

Demographic information such as age at enrollment, sex, body mass index (BMI), age at asthma onset and asthma duration was collected at the baseline visit. All patients underwent standardized assessments, which included peripheral blood total and differential cell counts, serum total immunoglobulin E (IgE), chest radiography, and skin prick tests with 24 common inhalant allergens (Bencard Co., Brentford, UK). Atopy was defined as the presence of a wheal reaction to 1 or more of the allergens characterized by a ≥3 mm greater diameter than the normal saline control or equal to or greater than that induced by histamine (1 mg/mL). Forced expiratory volume 1 second (FEV1), forced vital capacity (FVC), and pre- and post-BD FEV1 were measured before and after 2 puffs of albuterol (360 µg) were administered with a metered-dose inhaler at baseline and at 3-month intervals. PC20 methacholine (mg/mL) and sputum cell analyses were performed in eligible cases at enrollment. Sputum was induced using isotonic saline containing a short-acting BD and processed within 2 hours as previously described.21 Slides were prepared using cytocentrifugation, and 500 cells were counted on each slide after staining with Diff-Quick (American Scientific Products, Chicago, IL, USA). The patients were treated according to the Guidelines for Asthma Treatment issued by the Korean Academy of Asthma Allergy and Clinical Immunology.22 The total amounts of ICS and SCS administered during the first year were determined based on the electronic medical records and expressed as equivalent dosages of fluticasone propionate per day and equivalent dosages of prednisolone per year, respectively. Exacerbation was defined as described by American Thoracic Society/European Respiratory Society Task Force on Asthma.23 The protocol was approved by the Ethics Committees of Soonchunhyang Bucheon Hospital (SCHBC_2014_07_028) and Hallym Sacred Heart Hospital (2016_I009).
Trajectory clustering analysis
We performed a trajectory clustering analysis on the longitudinal post-FEV1 data (baseline and months 3, 6, 9 and 12) from 1,679 patients as follows: 1) the first estimate of the number of likely trajectories using the non-missing data of 448 subjects and 2) the second estimate using the full data from the total of 1,679 subjects after imputation of missing values (Supplementary Table S1). In the first step, a hierarchical cluster analysis of the longitudinal post-FEV1 values was performed using Ward's method to generate a dendrogram. Cluster boundaries were defined by large differences between successive fusion levels.24 Cluster quality was assessed by 2-step clustering using the Euclidean method with SPSS software version 18 (IBM Corp., Armonk, NY, USA) and then by trajectory clustering analysis using kml in the R package for k-means clustering of longitudinal data.25 In the second step, we imputed post-FEV1% missing values for 1,679 subjects using regression methods. The imputed data were subjected to trajectory clustering analysis as described above. The trajectory clustering analysis procedure is summarized in Fig. 1.
Statistical analysis
Analysis of variance (ANOVA) and Kruskal-Wallis and χ2 tests were used to compare parametric continuous, nonparametric continuous and categorical variables, respectively. Independent t tests and Mann-Whitney U tests were applied to compare continuous parametric and nonparametric variables between 2 trajectories. All statistical analyses were performed using SPSS.
RESULTS
Trajectory clustering analysis of post-BD FEV1% over 1 year in 448 asthmatics
Five clusters were optimal for discriminating the longitudinal values of post-BD FEV1 in the first 448 subjects and the second 1,679 subjects (Supplementary Fig. S1). The 5 trajectories yielded unique classification patterns for the 448 subjects (Tables 1 and 2, Supplementary Fig. S2): Trajectories 1 and 2 were characterized by normal baseline FEV1% values, which were maintained during the followup period. Trajectory 3 was associated with a mild decrease in baseline FEV1 with minimal, but significant, improvement over time (P < 0.001). Trajectory 4 was associated with moderate-to-severe derangement of baseline FEV1%, which dramatically increased to a normal level in the first 3 months (P < 0.001) and was maintained to the end of followup. Trajectory 5 was characterized by the lowest baseline FEV1%, which remained low to the end of the followup (P < 0.001).
Table 1
Longitudinal changes in the complete data of post-BD (448 subjects)

![]()
Table 2
Longitudinal changes in the complete data of post-BD (1,679 subjects)

![]()
Clinical characteristics associated with the trajectory clusters in the total 1,708 asthmatics
Among the total of 8,395 followup FEV1 values (1,679 subjects at 5 time points), 2,722 FEV1 values (32.3%) were missing (Supplementary Table S1). Thus, imputed FEV1 values were obtained by a regression analysis of the 5,673 measured FEV1 values. The trajectory clustering of the total of 8,395 FEV1 values yielded 5 trajectories (Tables 1 and 2, Fig. 2 and Supplementary Fig. S2), which was similar to the 5 trajectories for the 448 subjects. The clinical and demographic characteristics associated with the 5 trajectories are shown in Table 3. Trajectory 1 (15.4% of the total subjects) was associated with a supra-normal FEV1% from baseline to the 12-month follow up (112.75% ± 13.93% pred. and 116.07% ± 11.49% pred., respectively, Tables 1 and 2). The patients whose course followed this trajectory were middle-to-old-aged, predominantly female (84.6%) and had a higher BMI than those whose course followed the other trajectories. Among these subjects, 10% showed a short-acting BD-induced increase in FEV1 (85.7% for PC20 methacholine), and 10.4% exhibited improvement in FEV1 after treatment. The majority (87.6%) were on a low dose of inhaled ICS (<250 µg fluticasone equivalent/day) and had the lowest frequency of exacerbations over 1 year (0.2/year, Table 3).
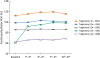 | Fig. 2Trajectory analysis of post-bronchodilator FEV1% values in 1,679 asthmatics and serial changes in the mean FEV1 values. Data are presented as mean ± standard deviation.FEV1, forced expiratory volume in 1 second.
|
Table 3
Clinical characteristics of the 5 trajectories in total 1,679 study subjects

Data are presented as mean ± standard deviation or number (%).
ANOVA, analysis of variance; BD, bronchodilator; BMI, body mass index; FEV1, forced expiratory volume in 1 second; ICS, inhaled corticosteroids.
*Dosages are presented as equivalent of fluticasone (µg/day), Low dose ICS ≤ 250 µg/day, medium dose 250–500 µg/day, and high dose < 500 µg/day of fluticasone or equivalent; †Dosages are presented as equivalent of prednisolone (mg/year).
![]()
Trajectory 2 (31.8% of the total subjects) was characterized by FEV1% values in the normal range from baseline (99.25% ± 9.64% pred.) to the end of follow up (100.98% ± 9.29% pred.); these values were lower than those associated with trajectory 1 (P < 0.001) (Tables 1 and 2, Fig. 2). This group was younger and predominantly females and had a high frequency of atopy. Among these subjects, 11.4% showed a short-acting BD-induced increase in FEV1 (81.7% for PC20 methacholine), and 11.2% showed improvement in FEV1 after treatment (Table 3). Most of these subjects (86.5%) received a low dose of ICS and had a low frequency of exacerbations over 1 year (0.3 ± 1.4). Thus, trajectories 1 and 2 represent mild asthma.
Trajectory 3 (32.0% of the total subjects) was associated with a mild decrease in basal lung function (86.09% ± 9.17% pred.), which was slightly improved at the 12-month followup (86.76% ± 9.60% pred., P < 0.001). These FEV1 levels were significantly lower than those of trajectories 1 and 2 (P < 0.001) (Tables 1 and 2, Fig. 2). This group comprised patients with a young age at onset with a longer disease duration. Among these subjects, 12.5% showed a short-acting BD-induced increase in FEV1 (85.9% for PC20 methacholine), and 10.8% showed improvement of FEV1 after treatment (Table 3). The exacerbation frequency over 1 year (0.4 ± 1.4) was slightly higher than that associated with trajectories 1 and 2 (P = 0.115) despite significantly higher doses of ICS and SCS (P = 0.007 and 0.020, respectively, Table 3).
Trajectory 4 (8.3% of the total subjects) was associated with a very low FEV1% at baseline (61.25% ± 13.04% pred.), and this dramatically increased to normal in the first 3 months (92.44% ± 11.17% pred., P < 0.001) and was maintained over the followup period (98.69% ± 10.53% pred.). This trajectory was associated with the highest prevalence of atopy (51.1%) and the highest mean IgE level. Among these subjects, 12.9% showed a short-acting BD-induced increase in FEV1 (89.2% for PC20 methacholine), and 97.1% showed improvement in FEV1 after treatment. The exacerbation frequency over 1 year (0.6 ± 1.4) was significantly higher in those whose course followed this trajectory than in those whose course followed trajectories 1, 2, and 3 (P = 0.027). The PC20 methacholine value of trajectory 4 was the lowest among the 5 trajectories. Larger quantities of ICS and SCS were used for individuals in this trajectory than for those who courses followed trajectories 1, 2 and 3.
Trajectory 5 (12.4% of the total subjects) was associated with a marked decrease in baseline FEV1% values, similar to trajectory 4; however, the FEV1 improved over the followup period (69.21% ± 13.47% pred. at 12 months; P < 0.001), suggesting persistent airway obstruction. Trajectory 5 was associated with a lower FEV1% over the followup period than trajectory 4 (P < 0.001). Among these subjects, 14.8% showed a short-acting BD-induced increase in FEV1 (87.9% for PC20 methacholine), and 39.2% showed improvement in FEV1 after treatment. This group was associated with the lowest frequency of atopy, the longest duration of asthma, the highest exacerbation frequency over 1 year (0.8 ± 1.6), and the highest total ICS and SCS among the trajectories.
Compared with trajectory 4, trajectory 5 was associated with asthmatics with less atopy (P = 0.056), a lower IgE level (P = 0.007), a higher dosage of SCS (P = 0.006), and a similar dosage of ICS (Table 3). Interestingly, trajectory 4 was associated with a higher proportion of subjects experiencing exacerbations over 1 year than was trajectory 5 (69.1% vs. 47.4%, P = 0.008).
Medication other than ICS and SCS showed similar patterns with the corticosteroids; Trajectories 4 and 5 showed higher dose of aminophylline, doxofylline, indacaterol, pranlukast, tiotropium and acebrophylline than other trajectories during the study period (Supplementary Table S3). Among them, dose of doxofylline was higher for subjects in trajectory 5 than those in trajectory 4 (P = 4.9×10−5). Dose of other drugs were comparable between trajectories 4 and 5.
Inflammatory cells in sputum and peripheral blood
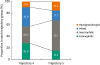
Sputum inflammatory cell patterns were stratified into eosinophilic, neutrophilic, mixed and paucigranulocytic. The subjects whose course followed trajectory 4 showed predominantly eosinophilic (28.0%) and mixed (32.9%) inflammation, and those whose course followed trajectory 5 predominantly showed neutrophilic inflammation (52.1%) (P = 0.001, Fig. 3, Supplementary Table S3). Unlike those whose course followed trajectory 5, subjects whose course followed trajectory 4 also had peripheral blood eosinophilia (P = 0.001) (Table 3).
DISCUSSION
In the present study, we identified 5 lung function trajectories based on post-BD FEV1 values over a 1 year followup and identified between-group differences in clinical and demographic parameters. Among the trajectories, 2 represented severe asthma: trajectories 4 and 5 (8.3% and 12.4% of the subjects, respectively) were associated with marked reductions in baseline FEV1; thus, about 20% of the subjects had severely deranged lung function at baseline. Interestingly, the baseline FEV1 value of those whose course followed trajectory 4 dramatically increased after 3 months of treatment, whereas those whose courses trajectory 5 showed persistent derangement of FEV1 despite continuous treatment with ICS. These data indicate that about 12% of asthmatics suffer from persistent airway obstruction.
Initial lung function is an important determinant of asthma outcomes; indeed, a low FEV1 value is a major risk factor for asthma exacerbations.126 Interestingly, the 2 groups, trajectories 4 and 5 in the present study showed similar responses to short-acting BDs (18.7% vs. 23.9%, P = 0.248) and to methacholine (3.6 ± 4.9 vs. 3.9 ± 5.8 mg/mL, P = 0.716). Therefore, airway constriction and bronchial smooth-muscle responsiveness were similar in the 2 groups because these 2 methods are related to the function of bronchial airway smooth muscle.2627 Accordingly, other factors may be responsible for the variation in the outcomes of asthma treatment.282930 Trajectory 4 was associated with atopic tendency, high IgE levels and high frequency of exacerbations, whereas trajectory 5 was associated with less atopic, lower IgE levels, and less frequent exacerbations. Additionally, differences in airway inflammation patterns may be related to the diverse responses to conventional treatments including ICS. In the present study, trajectories 4 and 5 were associated with contrasting patterns: eosinophilic inflammation in trajectory 4 and neutrophilic inflammation in trajectory 5. Eosinophilic inflammation is a pivotal trait of asthma and a marker of a good response to ICS and SCS.31 Although the FEV1 value for trajectory 4 at month 12 ranged from 77.7% to 135.0% of the predicted value, only 4 of 139 subjects had a subnormal FEV1 (< 80%), suggesting that, for those whose course follows this trajectory, airway obstruction with eosinophilic inflammation can be controlled using ICS.
Our finding of a high frequency of exacerbations in those whose course followed trajectory 4 is in agreement with previous reports that persistent eosinophilia in the peripheral blood and airways is associated with frequent exacerbations and fatal asthma attacks.43233 Moreover, 15% of the subjects whose course followed trajectory 5 also had eosinophilic inflammation. Therefore, the eosinophilic inflammation in this group may be resistant to treatment with ICS and may require anti-IgE and -IL-5 treatment.134 Our patients did not receive any additional medication to control their asthma during the study period.
Trajectories 1, 2 and 3 accounted for 79.3% of the study population. Trajectories 1 and 2 were associated normal to upper-normal lung function at baseline, whereas trajectory 3 was associated with a lower FEV1 at baseline, which remained evident at the end of the study (86.76%) (Tables 1 and 2). Additionally, trajectories 1 and 2 represent mild asthma with an annual frequency of exacerbations of less than 10%. In total, 20.8% of the subjects whose course followed trajectory 3 had at least 1 exacerbation during the first followup period. Thus, trajectories 1, 2, and 3 were categorized as mildly to moderately severe asthma. However, the demographic data were not consistent with previous cluster analyses of asthma phenotypes in Europe35 and the USA5: The subjects in our study were less atopic, older at asthma onset, and had a normal BMI compared to asthmatics in Western countries.51035 These parameters are in agreement with a previous study in Korea,3637 suggesting that they are limited to adult Korean asthmatics.
Trajectory 3 showed distinct characteristics from the other groups; the final FEV1 was even worse than that in trajectory 4. When compared with other trajectory groups, trajectory 3 is more severe phenotypes than trajectories 1 and 2 regarding baseline lung function, final FEV1 value, the number of exacerbation and medication requirement during the study period. When compared with trajectory 4, trajectory 3 showed lower prevalence of BD reversibility, lower total IgE, and lower blood and sputum eosinophils. These observations suggest that these features might contribute to decreased lung function after 1 year of treatment in trajectory 3 compared with trajectory 4.
Among 1,679 asthmatics in this study, 1,457 (86.8%) were newly enrolled patients who were treatment-naïve at baseline assessment, but 222 had been treated with asthma medications before the enrollment. The distributions of the 222 subjects in trajectory groups 15 were 10.4% (27 of 259 patients), 12.7% (68/534), 13.6% (73/538), 18.0% (25/139) and 13.9% (29/209), respectively, which showed no statistical significance (P = 0.313, Table 3). Among them, corticosteroid was administrated to only 1 patient in trajectory group 3, who was treated by a beclomethasone/formoterol inhaler (100/6 µg) at 28 days before the enrollment. Thus, our observation may be not biased by the previous treatment with inhaled corticosteroids.
When the same analysis was performed in 2,645 asthmatics including ex-smokers (n = 515) and current smokers (n = 451), the similar results between trajectories 4 and 5 were observed except smoking status; trajectory 4 was likely to be more eosinophilic, more atopic with higher levels of serum IgE, more frequent exacerbations, and more responsible to corticosteroids than those in trajectory 5 (Supplementary Fig. S3 and Supplementary Table S4). Interestingly, trajectory 5 had less proportion of ex-smokers and smokers compared to trajectory 4 (18.0% vs. 39.3%), but with greater amount of smoking (15.4 vs. 7.29 pack years) and longer periods of being ex-smoker (4.09 vs. 0.76 years). Thus, the different proportions of smoking and the difference of ex-smoking period were expected to have great confounding effects on interpretation of the longitudinal change of FEV1 trajectory: It was not clear whether the persistent airway obstruction of trajectory 5 was due to different airway dysfunctions or due to the different features of smoking and ex-smoking compared to trajectory 4. Accordingly, we excluded the effect of smoking on the 1-year trajectory of post-BD FEV1% changes to make the result to be clear. The effect of smoking on longitudinal changes in asthma symptoms should be assessed in further study with more precise design regarding balanced and matched duration and habits of cigarette smoking.
This study had several limitations. First, one-third of the longitudinal FEV1 data were missing; however, the missing data were imputed based on FEV1 values measured at least twice during the study period. Especially, the FEV1 values of 504 among 1,679 study subjects were restricted in the baseline and 3 months, which may introduce a bias in the imputation of late (over 6 months) values (Supplementary Table S1). However, as shown in Tables 1 and 2, and Fig. 2, the 5 FEV1% trajectories were mostly determined by values in the early stage of followup. When FEV1% trajectories were clustered using only the baseline and 3-month data (1,578 subjects, Supplementary Table S1), the concordance rate of the trajectory with those using full-set data described in this study (1,679 subjects) was 74.2% for entire trajectory groups, and 92.0% for trajectories 4 and 5. Thus, our observation, especially the difference between trajectory 4 and 5, could be acceptable. Furthermore, FEV1 values are unstable: in healthy individuals, the between-visit weekly variability in FEV1 is 12% and the annual variability is 15%; these values are higher in patients with airway disease.27 Secondly, we did not assess treatment adherence because we obtained medication information from the medical records. Thirdly, we did not collect longitudinal data on the blood and sputum levels of inflammatory markers, including eosinophils and neutrophils. Fourth, we excluded smokers from our asthma cohort to minimize the effect of smoking on lung function trajectories. As the prevalence of smoking in asthmatics is similar to that in the general population,38 our exclusion of smokers was unrealistic. However, this could be a strength of our study. Trajectory 5 was similar to the phenotype of severe asthmatics with fixed airflow obstruction or asthmaCOPD overlap, for which smoking is a major predisposing factor.3940 Thus, our finding demonstrates that severe neutrophilic asthma is an important phenotype after controlling for the effect of smoking. Finally, we could not rule out the possibility of the over-diagnosis of asthma in patients whose course followed trajectories 1 and 2 because this occurs frequently (25%35%) in primary care patients.4142 Additionally, blood and sputum cell counts were assessed in 612 (36.5%) and 757 (45.1%) of total 1,679 study subjects, respectively. Although the distributions of the subject assessed the inflammatory cell counts were statistically comparable between trajectories 4 and 5 (46.8% vs. 37.3%; P = 0.095 for blood cells, and 59.0% and 56.0%; P = 0.583 for sputum cells), the large proportion of subjects, who were not assessed, could introduce a bias in interpreting our observation about the different profiles of inflammatory cells between trajectory clusters.
In conclusion, this longitudinal analysis of post-BD FEV1 values identified 5 distinct trajectories. Trajectories 1, 2 and 3 comprised 80% of subjects with well-preserved lung function, whereas trajectories 4 and 5 were associated with different clinical parameters. Additionally, eosinophilic inflammation in sputum, particularly in individuals whose course follows trajectory 4, may be predictive of the response to conventional treatment for asthma, whereas neutrophilic inflammation in those whose course follows trajectory 5 suggests persistent airway obstruction. Further research should identify other predictors of the clinical course of asthma to facilitate personalized and effective treatment.
 XML Download
XML Download