

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Systemic lupus erythematosus (SLE) is an inflammatory multisystem autoimmune disease with protean clinical features and diverse autoantibodies and a variable clinical course and prognosis, where widespread and diverse vascular lesions are one of pathologic hallmarkers [123]. Vasculopathy may manifest in 11%~20% of SLE patients [14] and can be classified into inflammatory vasculopathy, vasculitis, and non-inflammatory thrombotic vascular diseases, such as antiphospholipid syndrome (APS) [3]. Vasculitis may associate with the APS in SLE [5]. Lupus vasculitis may present different clinical manifestations based on the organ involvement and size of the affected vessels [1]. Whereas cutaneous vasculitis is the most common form of lupus vasculitis, visceral involvement is described in less than 20% of vasculitic events but can be life-threatening [35]. Histologically, of all lupus vasculitis, cases more than 60% involve leukocytoclastic inflammation, 30% are vasculitis with cryoglobulinemia, while necrotizing vasculitis that can form aneurysmal lesions constitutes about 6% and has a poor prognosis [3].
Vasculitis-related aneurysms in SLE were typically, multiple, fusiform, small and frequently found in atypical locations [67] and showed necrotizing, fibrinoid degenerating, or old fibrotic angiitis in mainly small to medium or large arteries of approximately 5~10 mm to 200 mm in diameter in the biopsy [7]. Although there are several case reports of SLE patients suffering from hepatic [7], pancreatic [7], cerebral [6] and coronary aneurysms [7], renal aneurysm in SLE is extremely rare and, to the best of our knowledge, only four cases with renal microaneuryms associated with vasculitis have been reported, to date [891011]. According to these cases, renal artery aneurysms observed in SLE patients were multiple intraparenchymal microaneurysms and showed a strong resemblance to those in patients with polyarteritis nodosa (PAN). Here, we report the first case of SLE in Korea that presented with renovascular hypertension due to multiple renal intraparenchymal microaneurysms and was successfully controlled with immunosuppressive therapy.
CASE REPORT
A 41-year old female patient was admitted with a history of uncontrolled blood pressure. She was diagnosed as hypertension with hypertensive retinopathy one month before admission at local clinic. Five years ago, she had been diagnosed as seronegative rheumatoid arthritis at our hospital. At that time, blood pressure had been in the normal range. After taking low dose of steroid and disease-modifying antirheumatic drugs, her joint symptoms had improved.
On admission, physical examination revealed body temperature of 36.5℃, blood pressure of 154/100 mmHg, pulse rate of 78 times/minute, and swelling on all metatarsophalangeal joints of the left foot. Neither abdominal bruit nor cutaneous lesion was detected. She had no history of mucocutaneous lesions, ear-nose-and-throat lesions, pregnancy complications, or arterial and venous thromboses. The eye ground examination demonstrated retinal exudate on left eye, which consisted with hypertensive retinopathy. The ear-nose-and-throat examination did not show any abnormal findings and lung sound was clear. Laboratory investigation showed a leukocyte count of 8,550/mm3 with lymphocyte of 920/mm3, hemoglobin of 10.7 g/dL, platelet count of 396,000/mm3, CRP of 0.75 mg/dL (reference range, 0~0.5 mg/dL), ESR of 92 mm/h (reference range, 0~20 mm/h), serum creatinine 0.8 mg/dL (reference range, 0.6~1.3 mg/dL) , K 3.9 mmol/l (reference range, 3.3~5.1 mmol/l), prothrombin time 11.2 seconds (reference range, 10~14 seconds), activated partial thromboplastin time 33.6 seconds (reference range, 20~40 seconds), Hepatitis B virus surface antigen negative, C3 115.7 mg/dL (reference range, 90~180 mg/dL), C4 36.1 mg/dL (reference range, 10~40 mg/dL), serum immunoglobulin G (IgG) 2,354 mg/dL (reference range, 700~1,600 mg/dL), D-dimer 0.6 µg/mL (reference range, 0~1.0 µ g/mL), direct Coombs' test positive, antinuclear antibody (ANA) positive (1:320, peripheral type), anti-dsDNA antibody 8.6 IU/mL (reference range, 0~7 IU/mL), anti-Smith antibody negative, lupus anticoagulant negative, anti-cardiolipin antibodies negative, anti-β2 glycoprotein I antibody 320.5 U/mL (reference range, 0~7 U/mL), anti-neutrophil cytoplasmic antibody (ANCA) positive (1:640), and anti-myeloperoxidase and -proteinase 3 antibodies negative. In urine analysis, hematuria and proteinuria were not detected. Chest X-ray (Figure 1A) and chest computed tomography (CT) did not demonstrate any abnormal lesions, such as lung nodule, parenchymal infiltration or cavities. Water's view showed no haziness or opacification of the maxillary sinus (Figure 1B). Bone scan for evaluation of the associated joint symptoms revealed an increase in uptake of the first to fifth metatarsophalangeal joints on left foot (Figure 1C), but there was no radiographic bone erosion on the joints of both feet (Figure 1D). She was diagnosed as SLE based on positive results of ANA and anti-dsDNA antibody, lymphopenia and peripheral non-erosive arthritis.
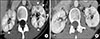
Evaluation of the cause of secondary hypertension revealed plasma renin activity 42.87 ng/mL/h (reference range, 1.31~3.95 ng/mL/h) and aldosterone 363.44 pg/dL (reference range, 10~105 pg/dL). Abdominal CT showed wedge-shaped low-attenuation regions on bilateral renal parenchyma in the postcontrast scan (Figure 2A) and renal angiography revealed multiple microaneurysms and stenosis in the branches of the renal artery (Figure 3A). Renal biopsy showed a well-demarcated parenchymal area with inflammatory cell infiltration and atrophic tubules and glomeruli, which was consistent with ischemic renal patholgy. However, there were no fibrinoid necrosis, granuloma, and luminal thrombus formation (Figure 4). In immunofluorescence stain, there were no abnormal depositions of IgG, IgA, IgM, C3 and fibrinogen. Based on the results of abdominal CT, renal angiography and renal pathology, she was diagnosed as renovascular hypertension due to renal microaneuryms and infarctions associated with SLE vasculitis.
She was treated with high dose of steroid (prednisone, 1 mg/kg) and myocophenolate mofetil (MMF) (2 g/day) for vasculitis and with antihypertensive drugs (valsartan 160 mg/day, amlodipine 5 mg/day) for renovascular hypertension. She did not receive anticoagulant therapy, such as heparin or warfarin. After two months of treatment, normalization of plasma renin activity and aldosterone level was observed (plasma renin activity 3.50 ng/mL/h; aldosterone 46.24 pg/mL). After ten months of therapy, abdominal CT showed decreased lesions with the wedge-shaped hypodensities in the renal parenchyma (Figure 2B), and renal angiography revealed remarkably reduced number of microaneurysms (Figure 3B). Follow-up ANCA level was 1:160. Blood pressure was well controlled by only amlodipine 5 mg/day.
DISCUSSION
Vasculitis, an inflammatory change of vascular walls, may manifest in as many as 56% of SLE patients throughout their life [3] and take many clinical forms due to its capacity to affect vessels of different size (arteries, veins, and/or capillaries) and sites (involving either skin or internal organs) [1]. Although vasculitis presents mainly as cutaneous lesions, life-threating ischemic injury may result from vasculitis of medium-sized vessels in gastrointestinal, cardiac, pulmonary, or cerebrovascular regions [1]. True renal vasculitis, accompanied by leukocyte infiltration of vascular walls and necrosis, is one of rare renal vascular lesions and was detected in only 2.4%, while immunoglobulin microvascular cast, lupus vasculopathy, was commonly detected lesions with 24% of 169 renal biopsies from SLE patients [12]. Furthermore, aneurysmal changes due to renal vasculitis have been extremely rarely reported and showed poor prognosis with high mortality [891011]. Renal arterial aneurysms observed in SLE patients are multiple intraparenchymal aneurysms which are rare among the renal artery aneurysms, less than 10% of all renal aneurysms, and have potential complications of peripheral dissection, thrombosis, renal infarction, and hypertension [13]. Our case also demonstrated renovascular hypertension and renal infarctions associated with multiple saccular intraparenchymal microaneurysms, which corresponded with the earlier reports.
In general, aneurysm formation and growth is influenced by hemodynamic and endothelial changes. In addition to these mechanisms, in situ formation, or the deposition, of immune complexes within the vascular wall may trigger the inflammatory responses and lead to aneurysmal changes [2]. Especially, antibodies against endothelial cells (AECAs) have been implicated as a major endothelial cell cytotoxic effector in the pathogenesis of lupus vasculitis and AECA-endothelial cell interaction attracts monocyte adhesion and induces secretion of chemoattractant proteins and cytokines, thus triggering vasculitis [23].
APS is a condition defined as a predisposition of vascular thrombosis and/or recurrent miscarriages or other obstetric emergencies in association with hematologic abnormalities and specific antibodies against phospholipid-binding plasma proteins [2]. There are several case reports on visceral aneurysms associated with primary and secondary APS [14]. Even though SLE patients with vasculitis have a higher prevalence of some APS-related features than those without vasculitis, possible roles for APS antibodies in the pathogenesis of vasculitis has been suggested [1], we tried to distinguish lupus vasculitis from APS in this case, because therapeutic implications are different between these two diseases (immunosuppression vs. anticoagulation). We made the diagnosis of lupus vasculitis in this case for the following reasons. First, she had no history of pregnancy complications or vascular thrombosis and did not show thrombocytopenia or prolongation of coagulation time on admission, even though she had anti-β2 glycoprotein I antibody. In addition, she did not show an APS-related features, such as livedo reticularis. Second, the most frequently reported pattern on renal angiography in APS vasculopathy was smooth, delineated, generally noncritical stenosis distal to the ostium of the renal artery [15]. However, renal angiography in our case demonstrated multiple intraparenchymal microaneurysms, which was consistent with those of previously reported renal vasculitis. Third, although there are some case reports on arterial aneurysms associated with APS, the association of APS and arterial aneurysms is not established and in most cases of secondary APS, the presence of arterial aneurysms can be attributed to the underlying systemic diseases [14]. Actually, our patient showed dramatic improvement in the renal pathology after treatment with steroid and immunosuppressive agent. She did not receive any anticoagulant therapy. Considering that treatment of APS patients must be based on the use of platelet anti-aggregating agents or anticoagulants [3], this case is thought to be indicative of vasculitis, not APS vasculopathy.
The two most common systemic inflammatory vasculitis associated with aneurysmal formation are PAN and microscopic polyangiitis (MPA) [15]. Furthermore, renal involvement in PAN and MPA may induce renovascular hypertension, renal arterial aneurysms and infarctions, as is the case with our patient, although the underlying mechanisms of vasculitis in PAN and MPA are different from those in SLE. However, being a clinically young woman without involvement of peripheral nervous system, subcutaneous nodules and presence of ANA and anti-dsDNA antibody were all against the diagnosis of PAN. In addition, renal pathology did not show any granuloma or glomerulonephritic features. We also considered that SLE patients may show positive ANCA without any clinical significance and have renal microaneurysms similar to those in patients with PAN.
Because vasculitis significantly impairs the quality of life of SLE patients and represents the most frequent cause of death intensive treatment to reduce the SLE activity and prevent flares may be needed [23]. For the treatment of visceral forms of SLE vasculitis, cyclophosphamide and azathioprine are the two most commonly used cytotoxic immunosuppressive agents [3]. In addition, MMF has been introduced in the treatment of SLE and seems to be effective in controlling global disease activity even when other therapeutic regimens have failed. Recently, biologics, including rituximab and belimumab, may be considered in SLE patients with visceral vasculitis who are refractory to various combinations of immunosuppressive agents. In our case, with consideration for maintenance of ovarian function, high dose glucocorticoid and full-dose of MMF were given for reduction of disease activity and antihypertensive drugs for control of hypertension. After ten months of therapy, follow-up abdominal CT and angiography showed a significant improvement of renal infarctions and microaneurysms, which suggested that visceral aneurysmal changes associated with lupus vasculitis are gotten better through effective treatment. Her blood pressure was also well controlled with much lower dosage of antihypertensive drug.
SUMMARY
We report a case of a SLE patient with renovascular hypertension due to renal microaneurysms associated with renal vasculitis which improved after immunosuppressive therapy. This case suggests that it is considered for clinicians examining SLE patients presenting with hypertension to consider the possibility of renovascular hypertension resulting from vasculitis. In such conditions, further investigations with associated imaging studies, such as abdominal CT and renal angiography, are clearly warranted.



 XML Download
XML Download