

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cannabis or marijuana is the most commonly consumed recreational drug after alcohol in the world (1). However, in Korea, its usage is illegal, and methamphetamine was the most commonly abused illicit drug followed by cannabis (2). Cannabis has psychological effects in the central nervous system (CNS) including euphoria, relaxation, and goodness (3). However, CNS injury manifesting as ischemic stroke following use of cannabis has been rarely reported in literature (145678). We introduce a case of a female with acute ischemic stroke after cannabis usage with multifocal intracranial vasoconstriction on magnetic resonance angiography (MRA). We will also review literature about the underlying mechanism, clinical manifestation, and imaging findings of cannabis-related stroke.
CASE REPORT
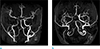
A 47-year-old female presented to the emergency department with sudden onset right gaze preponderance and left neglect. Her initial vital signs were normal, and the National Institutes of Health stroke scale score was 10. She had no underlying medical history and no family history of cerebrovascular disease. Her laboratory studies consisting of blood count, coagulation times, electrolytes, ammonia level, liver and renal functions were all normal. Brain non-contrast computed tomography (CT) revealed low attenuation in the right periventricular white matter and right parietooccipital lobes. Brain magnetic resonance imaging (MRI) revealed acute infarctions in the right parietooccipital lobes, basal ganglia and thalamus (Fig. 1). Time-of-flight (TOF) MRA revealed multifocal moderate to severe stenosis in right distal internal carotid artery (ICA), right M1 segment of middle cerebral artery, right A1 segment of anterior cerebral artery, distal basilar artery, right posterior cerebral artery (PCA), and left PCA (Fig. 2). Additional laboratory studies were conducted on admission to our intensive care unit to determine the underlying cause of stroke. Lupus anticoagulant, anticardiolipin antibodies, anti-beta2-glycoprotein I, anti-DNA and cryoglobulin levels were normal. Other studies to exclude cardio-embolism, including electrocardiogram, serum troponin I level, creatine kinase and transthoracic echocardiography were also normal. But, in a toxicological screening test for benzodiazepines, barbiturates, cocaine and synthetic cannabinoid metabolite (delta-9 tetrahydrocannabinol [THC]), results for cannabinoid metabolite were positive. She continued to deteriorate neurologically despite therapy. Follow up brain non-contrast CT revealed aggravation of cerebral edema with brain herniation. Her clinical condition had fulfilled the brain death criteria. Her organs were donated after brain death judgment by the Brain Death Assessment Committee.
DISCUSSION
Cannabis is the most commonly used recreational drug after alcohol in the world, that contains a complex mixture of 486 chemicals, including 60 cannabinoids. The major psychoactive ingredient of cannabinoid is delta-9 THC, lipid soluble and well distributed. The use of cannabis causes a variety of cardiovascular side effects including arrhythmias (atrial fibrillation and sinus tachycardia), increased cardiac output, postural hypotension, and peripheral vasodilatation (139). However, cerebrovascular effects are less well understood. Cannabis-related stroke has been infrequently reported in previous literature (145678). To the best of our knowledge, this is the first report of cannabis-related stroke in South Korea. Also image findings of multifocal intracranial stenosis related to cannabis use were previously reported in few cases (610), whereas a majority of cases demonstrated normal intracranial and distal neck arteries (1).
A review of previous literature suggests the association between cannabis use and ischemic stroke is relatively strong (145678). A case-control study also has revealed this association; cannabis was associated with cerebrovascular events after adjusting for age, sex and ethnicity (5). Brain death from cannabis-related stroke was rarely reported. In a previous study reporting a total of 17 patients with cannabis-related stroke, two patients with cerebellar infarcts expired. But one patient expired due to sudden death within 22 hours after admission, suggesting brainstem compression, and cause of death in the other patient was not specified (1). There are various hypotheses that explain the association between cannabis and ischemic stroke, including vasospasm, postural hypotension and cardio-embolism (7). But the precise effect or mechanism of cannabis on the brain in patients with ischemic stroke has not been elucidated. The most frequently proposed mechanism in cannabis-related stroke is vasospasm. Previous studies have demonstrated that THC increases oxidative stress and induces cerebral mitochondrial dysfunction, leading to vasoconstrictive effects with unstable cerebral blood flow and ischemia (18). Cannabis associated strokes were more frequent in the vertebrobasilar territory, suggesting susceptibility of posterior circulation (6). Few cases of cannabis associated reversible cerebral vasoconstriction syndrome have been also reported (410). In our case, MRA demonstrated multifocal intracranial stenosis with large vessel territories infarction on diffusion weighted images. Vertebrobasilar territory involvement of intracranial stenosis was also seen in our patient, consistent with the previous study that revealed susceptibility of posterior circulation (6).
Postural hypotension is another suggested mechanism of ischemic stroke, but in our case, the patient was normotensive and TOF MRA revealed multifocal stenosis of the intracranial vessels, making this mechanism less likely. Cardio-embolism is also considered as a possible mechanism of cannabis-related stroke. Cannabis use increased risk of tachyarrhythmia and myocardial infarction (39). In our case, work up for cardio-embolic causes of stroke was negative and TOF MRA revealed multifocal intracranial stenosis favoring vasospasm rather than thromboembolism.
In conclusion, we report of a case of acute ischemic stroke after use of cannabis, revealing multifocal intracranial stenosis on TOF MRA. Although the precise mechanism of cannabis on the brain remains uncertain, our case of acute ischemic stroke with multifocal intracranial stenosis after cannabis use suggests possibility of vasospasm. Awareness should be raised to cannabis-related stroke and toxicological screening test should be effective in the diagnosis.

 XML Download
XML Download