

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
The profunda femoris artery (deep femoral artery, PFA) is the first and largest branch of the femoral artery (FA) in the thigh [1]. Thus, it constitutes the major source of blood supply to the thigh area, since the remaining (superficial) FA supplies mainly the rest of the lower limb (leg and foot) [1]. PFA originates dorsolaterally from the FA about 3.5 cm distal to the inguinal ligament, to pass downward and medially to the apex of the femoral triangle [12]. It courses posterior in front of pectineus muscle and thereafter between the adductor longus and adductor brevis muscles [12]. Afterwards, it travels between the adductor longus and adductor magnus, finally penetrating through the latter, to connect with branches of the popliteal artery behind the knee [12]. PFA gives rise to lateral and medial circumflex femoral branches, as well as numerous muscular branches and four perforating arteries: the first two perforating adductor brevis the other two the adductor magnus (the last perforating artery being the PFA itself as cited above) [2].
Variations of the normal pattern of the PFA have been described in the available literature [3456789], most of them concerning its point of origin from the FA and course.
We present a rare case of a double PFA, where each separate branch followed the expected arterial pattern.
Go to : 
Case Report
An embalmed female human cadaver of Caucasian (Hellenic) origin was examined during routine educational dissection at the Anatomy Department of the Medical School of the University of Athens. The cadaver derived from body donation with informed consent by the donator himself.
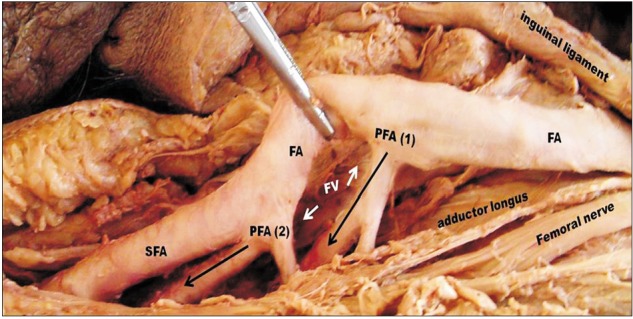
During the dissection of the left thigh an extremely rare vascular finding attracted our attention. Namely, routine dissection of the inguinal ligament, FA and its branches, revealed two PFAs. The first of it originated in a distance of approximately 5.4 cm from the inguinal ligament (Fig. 1) and after 1.2 cm it gave rise to a muscle branch for the adductor longus. It continued its course between the adductor muscles and gave two perforating branches. As the dissection of the FA continued, a second PFA was discovered, 3.7 cm after the origin of the first PFA and 9.1 cm after the inguinal ligament (Fig. 1). This artery gave immediately rise to a muscle branch and then two perforating ones. The lateral and medial circumflex arteries were absent. After the branching of the second PFA the FA continued as superficial femoral artery. The rest of the arterial pattern of the left thigh was the expected one. No variations were discovered at the right thigh.
Go to :
Discussion
A series of anatomical variations of the PFA are mentioned in the literature (Table 1). PFA is noted to arise in a dorsolateral direction in about 50% of cases and it is located strictly dorsal in about 40% [34567]. Furthermore, a medial origin is encountered in 10% of cases, while it may present a trifurcation (meaning the origin of the PFA and two circumflex arteries from a common stem from the FA) in 4.5% of cases [4]. Occasionally the superficial branches of FA may took origin from PFA instead of the femoral artery, as the rule is [345678]. PFA may be rarely absent, while its duplication is extremely rare with an incidence less than 1% [8]. A double PFA is rarely reported, usually as a radiologic finding [8].
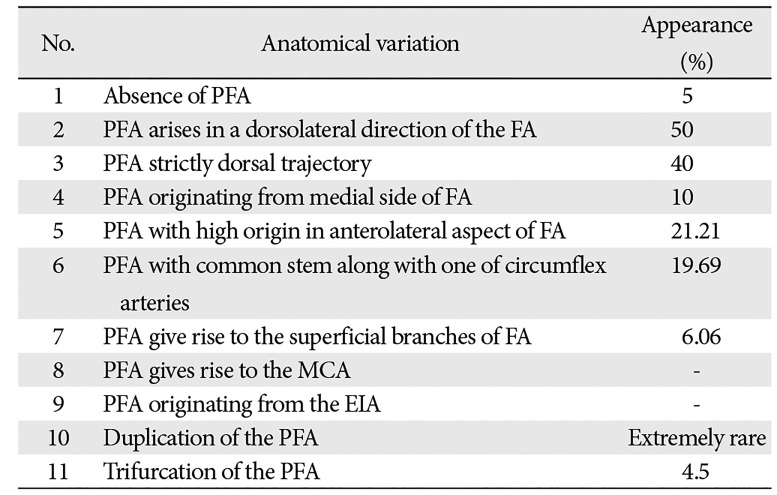
Table 1
Anatomical variations of the PFA
![]()
Most anatomical variations of the normal arterial pattern of the PFA seem to be asymptomatic. They are usually incidental findings in the operating theatre, or in the dissection room, or they may come to light during an angiographic or radiologic examination. However, in many cases, asymptomatic, or not, PFA's anatomical variations may influence technical considerations during all cases of interventional procedures [9].
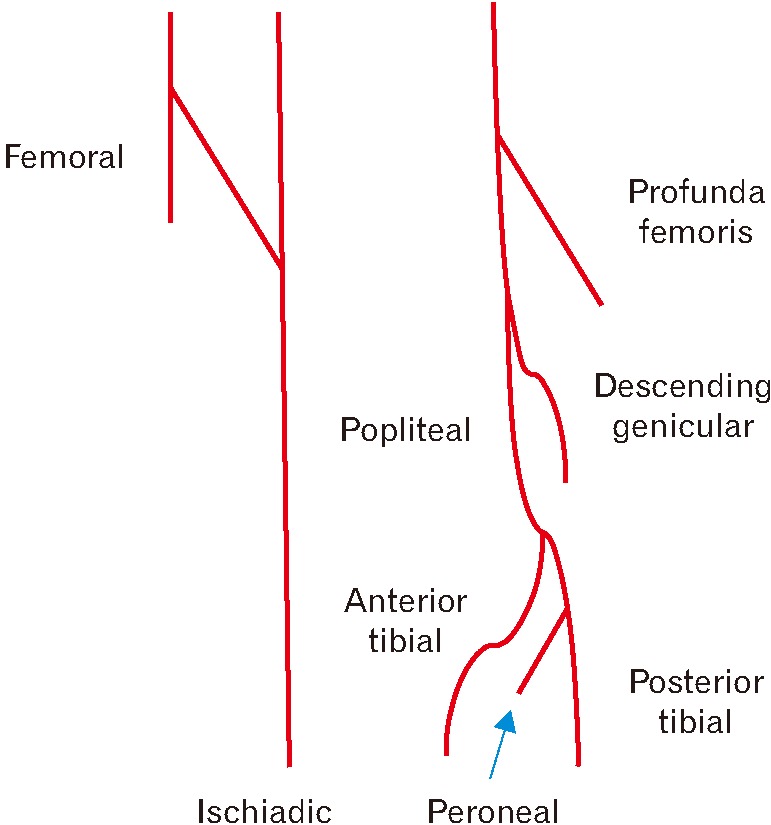
The arteries of the lower limp derive from the fifth lumbar artery, with a complicated path of an anastomotic network between two its branches, namely the dorsal sciatic and the ventral femoral artery, which will finally lead to the creation of the PFA [10] (Fig. 2). Various triggering factors may result in anomalies in the form of deviation from the expected pattern [10].
The PFA is an artery which is being exploited for a plethora of clinical procedures such as arteriography, ultrasonography, Doppler imaging, haemodialysis, plastic and vascular surgery, and angioplasty. In plastic surgery, free profunda artery perforator (PAP) flap has recently been brought back for head and neck reconstruction [11], while PAP is also proposed for autologous breast reconstruction [12]. On the other hand, obstructive disease in PFA, as well as aneurysms may be encountered and need intervention [13], while PFA itself may be used as an entrance point for vascular reconstruction [14]. Hence, accurate anatomical knowledge is very important for all clinicians [15], especially in the rare case of a double PFA.
Rarity of the duplication of the PFA may explain the lack of references concerning this anatomical variation. Our report highlights the importance for invasive practitioners to comprehend topographical anatomy and vascular variations of the PFA.
Go to :
 XML Download
XML Download