

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Computerized cognitive training is a nonpharmacological intervention for patients with cognitive impairment that has been commercialized by several research groups and companies. It can be much cheaper to implement than traditional neuropsychological training methods, which require trained neuropsychologists, and has the advantage of easy accessibility for community-dwelling elderly. Furthermore, compared to traditional methods, it might be easier to optimize computerized cognitive training according to the cognitive status of an individual patient.
Several studies have validated the clinical efficacy of computerized cognitive training applications.1 A recent systematic review found that working memory, executive function, and processing speed benefited the most from classic computerized cognitive training tasks, and that these benefits were comparable with those achieved using traditional cognitive training methods.1 Previous studies have demonstrated cognitive training to be primarily effective in patients with mild cognitive impairment (MCI) or subjective memory impairment (SMI).23 Moreover, another study confirmed that the levels of brain-derived neurotrophic factor were elevated after 12 weeks of cognitive training in MCI patients.4 These results suggest that the brains of MCI patients are still plastic and a suitable target for cognitive training.2
Aside from studies that have provided neuropsychological data, research on the neural substrates of computerized cognitive training is still lacking.5 Increases in the cortical thickness and the volumes of the posterior cingulate cortex, postcentral gyrus, and hippocampus have been reported; however, these studies did not examine functional changes.678 Previous studies using functional neuroimaging have noted activation of the left anterior hippocampus, inferior and middle frontal gyri, and left thalamus;910 however, those studies did not identify structural changes.
Brain plasticity due to cognitive training results from dendritic sprouting and synaptogenesis, and this process can be detected using structural and functional imaging.11 However, subtle changes may be obscured if only a single specific test is used, which may explain the inconsistency of previous reports.5 It may be advantageous to combine multiple types of assessment such as magnetic resonance imaging (MRI), positron-emission tomography (PET), and electroencephalography (EEG), rather than using a single specific test to investigate highly complex neurobiological processes.1213
In this study we aimed to identify the neural substrates underlying the effectiveness of computerized cognitive training using a multimodal approach, in order to understand the neurobiological processes underpinning the effectiveness of this training. We also investigated whether the same changes are induced in the brain in subjects with MCI, SMI, and normal cognition, in order to identify the target groups that can benefit from computerized cognitive training.
METHODS
Subjects
Eligible subjects who met the inclusion criteria were recruited from June 2012 to May 2013 at the memory clinic of Seoul National University Bundang Hospital. Participants in the normal-control group were recruited from the local community in Bundang district, Seongnam, Republic of Korea through advertisements. The Institutional Review Board of Seoul National University Bundang Hospital approved this study (IRB No. B-0809-061-008). All participants gave written informed consent.
The inclusion criteria were 1) aged >50 to ≤70 years, 2) ≥6 years of education, and 3) no physical limitations preventing the dominant hand from using a computer mouse. Subjects who had any structural lesions or psychiatric disorders that were associated with memory deficits were excluded. The subjects also had to be able to undergo pre- and posttraining evaluations such as EEG, fluorodeoxyglucose (FDG) PET, and MRI. We excluded patients who had scalp lesions, severe back pain, or claustrophobia that precluded such pre- and posttraining evaluations.
A computerized cognitive assessment was applied to eligible subjects for the baseline assessment. The computerized cognitive assessment tools evaluated six cognitive domains: memory, language, calculation, visuospatial function, attention and psychomotor speed, and executive function. Standardized scores (age-, sex-, and education-adjusted z-scores) were derived based on an independent validation study (n=120) and norm database (n=702) (unpublished data). The SMI, MCI, and normal-control groups were defined using clinical history, the Mini Mental State Examination (MMSE),14 Instrumental Activities of Daily Living (IADL),15 the Korean Dementia Screening Questionnaire (KDSQ), and a computerized cognitive assessment.16
SMI was diagnosed based on the following criteria: 1) sustained subjective memory complaints lasting at least 6 months with a positive response for the question, “Do you think you have memory problems nowadays?,” 2) self-belief that their current memory function had decreased compared to what it was previously, 3) MMSE score ≥mean minus 1.5 standard deviations relative to the age and education-level norms, 4) normal results in all domains of the computerized cognitive assessment, 5) IADL score <0.43,1517 and 6) KDSQ score ≤6.16
Based on the cognitive tests performed for a routine medical assessment, MCI was defined according to criteria that included concern about a change in cognition, impairment in one or more cognitive domains, preservation of independence in functional abilities, and absence of dementia based on the diagnosis of the attending physician.18 The homogeneity of the cohort was increased by only including patients with Clinical Dementia Rating (CDR) scores of 0.5 and CDR Sum of Boxes (SOB) scores ranging from 0.5 to 2.0.
Participants in the normal-control group met the criteria for normal elderly as suggested by Christensen.19 They did not complain of any subjective memory decline. Their MMSE score was at least mean minus 1.5 standard deviations relative to their age and education-level norms. The subjects in the control group had IADL scores <0.43 and KDSQ scores ≤6.
Computerized cognitive training
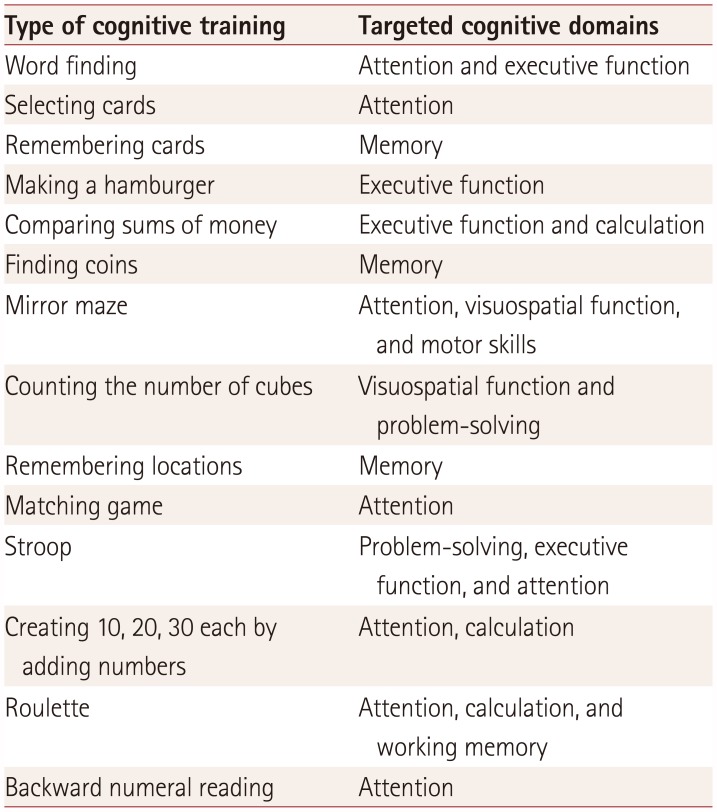
Cognitive training was conducted using a custom-developed computerized cognitive training apparatus developed through collaborative research with the Korean Institute of Science and Technology and the Primpo company. It was designed to stimulate numerous cognitive domains simultaneously by using objects and sounds familiar to the Korean elderly. Training themes and scenarios were developed and evaluated by six board-certified neurologists and three neuropsychologists who specialize in dementia. The most-appropriate training modules were selected through preliminary studies, and then simulated and finalized for application in this study through consensus reached by discussions among the participating neurologists and neuropsychologists. Detailed explanations of each task are provided in Table 1.
Each subject participated in 24 sessions of cognitive training, with each consisting of 40 minutes of training performed twice weekly. In the first training session, subjects underwent a pretraining evaluation of their cognitive function and were provided with instructions for the remaining sessions. Trained personnel provided close guidance to facilitate the training process and ensure the consistency of the cognitive training protocol.
Pre- and posttraining assessments
Subjects completed a pretraining evaluation prior to receiving the cognitive training. After a total of 12 weeks of computerized cognitive training, posttraining evaluations were conducted no more than 1 week after the last training session. Pre- and posttraining evaluations comprised cognitive assessments, EEG, FDG-PET, volumetric MRI, and diffusion-tensor imaging (DTI) (Fig. 1).
Pre- and posttraining cognitive assessments were performed using the aforementioned computerized cognitive assessment methodology and a predetermined conventional neuropsychological battery, which comprised several neuropsychological tests for evaluating mainly the frontal domain: digit span (forward/backward) and spatial span (forward/backward) for attention and working memory, trailmaking test-black & white (TMT-B&W),20 and a digit symbol modality test. Each subject underwent neuropsychological evaluations 1 week prior to and also after the cognitive training. Subjects were also evaluated using the MMSE, CDR, CDR-SOB, Global Deterioration Scale, IADL, KDSQ, and the short version of the Geriatric Depression Scale.151617
The neuroimaging analysis involved changes in cortical thickness being detected using surface-based morphometry with Freesurfer software (version 5.1.0, MGH, Martinos Center, Harvard University, Boston, MA, USA). Pre- and posttraining changes were compared among the normal control, SMI, and MCI groups. We applied tract-based spatial statistics (TBSS) to investigate the possible neural substrates of cognitive training in DTI data. Any significant changes in local activation patterns in FDG-PET were analyzed by applying statistical parametric mapping (SPM version 8, http://www.fil.ion.ucl.ac.uk/spm) using MATLAB (The Math-Works, Sherborn, MA, USA). We also applied power spectral analysis to the pre- and posttraining EEG data. The spectral ratio was calculated as the ratio between fast (α+β1+β2+β3) and slow (δ+θ) frequency bands. Each spectral ratio was compared between the pre- and posttraining EEG recordings and among the normal, SMI, and MCI groups. The neuroimaging protocols are described in detail in the Supplementary Material in the online-only Data Supplement.
Statistical analysis
For the statistical analysis, continuous variables were compared using analysis of variance or the Kruskal-Wallis test followed by Scheffe's post-hoc test. Categorical variables were analyzed using chi-square tests or Fisher's exact test, as appropriate. In comparing the changes between before and after training, the Wilcoxon signed-rank test was used as a nonparametric test. Statistical significance was defined as a two-tailed p value of <0.05. Statistical analyses of volumetric MRI data were adjusted for age and education level, and the significance threshold was set at p<0.001, uncorrected for multiple comparisons and with an extended k threshold of 50 voxels. For TBSS, voxel-wise statistics were completed for all skeletonized DTI measures across all subjects, using a general linear model with threshold-free cluster enhancement methods and 10,000 permutations.21 A significance threshold for group comparisons was set at p<0.05, corrected for multiple comparisons.
RESULTS
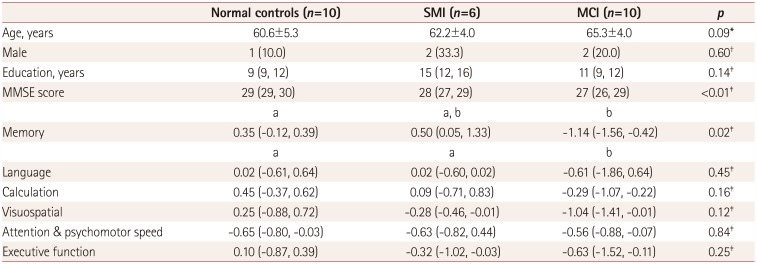
This study enrolled 26 subjects: 10 MCI patients, 6 SMI patients, and 10 normal controls. The MCI patients comprised six amnesia patients (two in a single domain and four in multiple domains) and four nonamnesia patients (two in a single domain and two in multiple domains). The baseline demographic characteristics did not differ among the three groups, but there were significant intergroup differences in MMSE and memory-domain scores (Table 2). All of the participants completed 24 sessions of cognitive training during the study period.
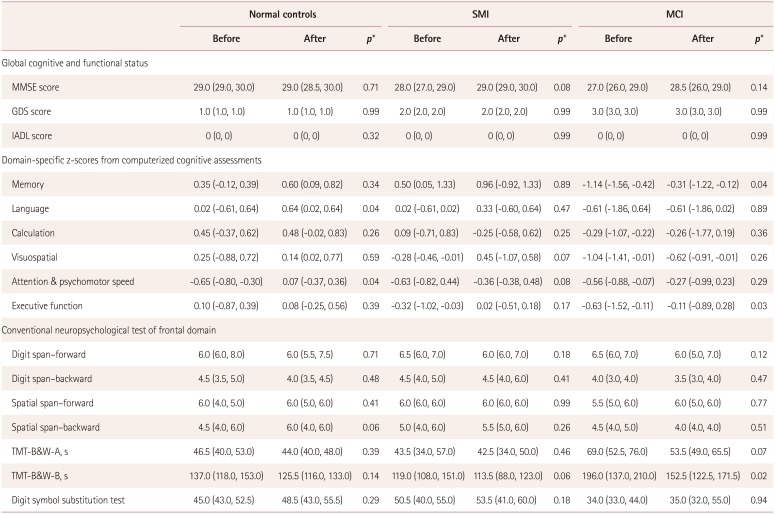
There were no significant changes in global cognition (MMSE score) or activities of daily living (IADL score) abilities in any of the groups between pre- and posttraining. However, the MCI group showed a significant improvement in the TMT-B&W-B (145.2±44.3 s at pretraining vs. 128.3±35.6 s at posttraining, mean±standard deviation, p<0.01) (Table 3). In addition, the MCI group showed a marginal improvement in the TMT-B&W-A (p=0.07). The computerized cognitive assessment revealed significant improvements in scores in the memory and frontal executive-function domains (Table 3).
In the normal group, the language- and attention-/psychomotor-domain scores improved significantly, and there was a nonsignificant improvement after training in the spatial span (backward) test (4.6±1.4 at pretraining vs. 5.4±1.2 at posttraining, p=0.06) (Table 3).
In the SMI group there was a tendency for improvement in general cognition based on MMSE scores (28.0±0.9 at pretraining vs. 29.2±0.8 at posttraining, p=0.08) and trail-making test-B (123.0±35.7 s at pretraining vs. 107.5±27.2 s at posttraining, p=0.06), although these differences did not reach statistical significance (Table 3).
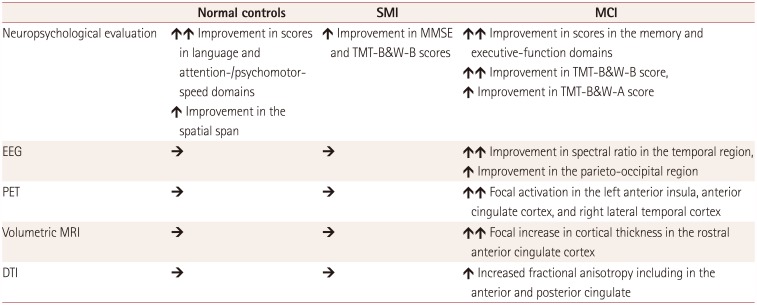
We compared the spectral ratio between the baseline and follow-up EEG data. The posttraining EEG data showed significant increments in the spectral ratio, particularly from the temporal electrodes in the MCI group (0.9 vs. 1.6, p=0.03) (Supplementary Table 1 in the online-only Data Supplement). There were no significant differences in the frontal, temporal, and parieto-occipital areas in the normal and SMI groups.
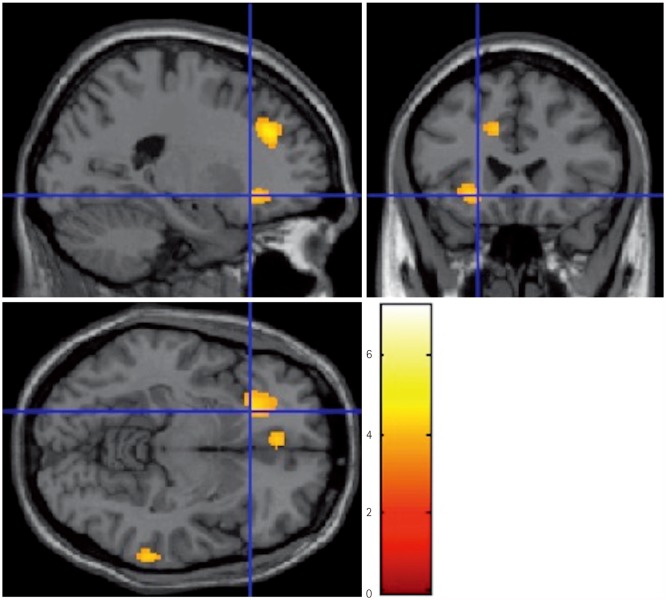
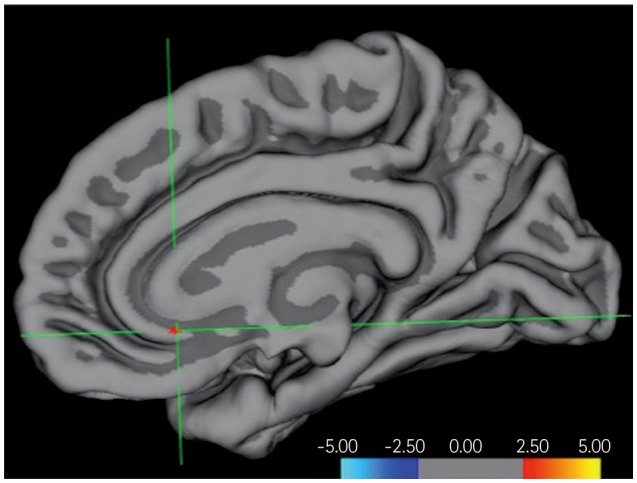
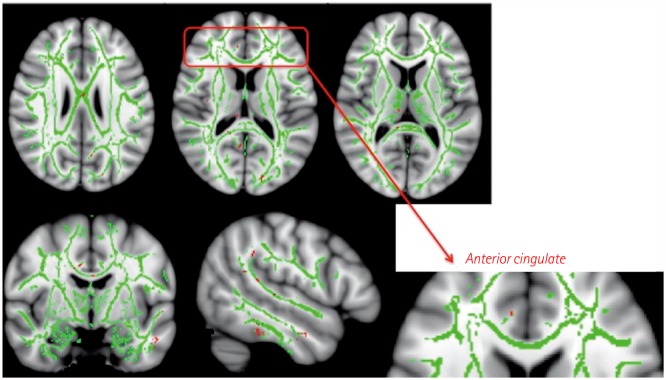
The neuroimaging analysis revealed significant functional and structural changes only in the MCI subgroup. Statistical parametric mapping of FDG-PET data revealed focal activation in the left anterior insula, anterior cingulate cortex, and right lateral temporal cortex in the MCI group (uncorrected p<0.001; Fig. 1 and Supplementary Table 2 in the online-only Data Supplement). Volumetric MRI also showed a focal increase in cortical thickness in the rostral anterior cingulate cortex after training in the MCI group, as analyzed using surface-based morphometry (Fig. 2 and Supplementary Table 2 in the online-only Data Supplement). The TBSS analysis of the posttraining DTI data revealed several regions of increased fractional anisotropy compared to the pretraining DTI, including the anterior and posterior cingulate cortices (Fig. 3 and Supplementary Table 2 in the online-only Data Supplement). These changes in the anterior cingulate cortex and insula were not observed in patients with SMI or the normal controls.
DISCUSSION
In this study we found that the cognitive improvement induced by computerized cognitive training was accompanied by structural changes in the anterior cingulate cortex and anterior insula. Subjects with MCI and normal cognition showed significant improvements mainly in scores in the memory, language, and frontal domains (Table 4).
Previous studies of the neural correlates of cognitive training have produced inconsistent results, which have varied with the characteristics of the study population and the types of cognitive training.22232425 For instance, combined cognitive training and progressive resistance training was found to prevent deterioration in the memory domain and increase the cortical thickness in the posterior cingulate cortex in patients with MCI.6 In middle-aged and elderly healthy adults, memory training also increased the cortical thickness in the right fusiform and lateral orbitofrontal cortices.23 Processingspeed training resulted in changes in cortical thickness in the right precentral gyrus, left superior temporal gyrus, and bilateral occipitotemporal junction, as well as the functional activity in the left operculum and superior temporal gyrus.26 Fractional anisotropy in left anterior white-matter structures was also significantly increased by so-called Methods of Loci training.27
Functional assessments using FDG-PET have produced conflicting results. Several studies using FDG-PET showed increased resting activity after cognitive training, which can reflect compensatory mechanisms in patients with severe brain disease. It may also reflect reduced resting activity, perhaps indicating a normalization of activation owing to greater efficiency in allocating and deploying cognitive resources.2425 Quantitative EEG is also useful for detecting the early phases of Alzheimer's disease. However, there have been few reports on changes in quantitative EEG parameters after computerized cognitive training.28
Previous studies have generally used only a single neuroimaging modality to test a particular hypothesis.232527 In contrast, the present study used both structural and functional neuroimaging modalities to investigate the effects of cognitive training. Similar changes were detected by these multimodal neuroimaging techniques, and they therefore provide more-robust information regarding the neural substrates of cognitive training. Our results corroborate current evidence that training for relatively short periods of 12–26 weeks can induce structural and functional changes in the brain, which supports the presence of brain plasticity in patients with MCI.67 Understanding the underlying neural mechanisms may assist in the development of strategies to overcome pathological processes and enhance compensatory mechanisms.
Our application of multimodal neuroimaging modalities revealed significant changes in the anterior cingulate cortex and anterior insula. The anterior cingulate cortex is part of the medial frontal cortex and is involved in decision-making. It is known to play a role in judging the subjective value of actions, which facilitates optimal performance by allowing evaluations of potential gains or losses.29 Moreover, it is also important in dynamic communication with the medial and lateral frontal cortices during conflict adaption, which involves mediation among various incongruent stimuli.29
Both the anterior cingulate and anterior insula are also major hubs of the salience network.30 The salience network simultaneously receives inputs related to several internal and external stimuli, and makes decisions regarding which stimuli are the most pertinent to the current situation.30 In situations of impaired memory or cognition, activation of the salience network could improve both the processing speed and the use of coping strategies to select the most-valuable stimuli and suppress unwanted cognitive processes. The efficient recruitment of impaired cognitive resources could improve the ability to cope with cognitive impairment. A previous study using functional MRI demonstrated that the salience network activity was up-regulated during attention tasks.31 Furthermore, the degree of dopaminergic D2 receptor binding in the salience network is significantly lower in patients with Parkinson's disease (PD) and MCI than in patients with PD but without cognitive impairment. These results suggest that the salience network is vulnerable in PD, including associative memory and executive function.32
There were no significant changes in the results from the neuroimaging evaluations in the SMI and normal control groups. There are conflicting reports regarding the effectiveness of cognitive training in these groups. Previous studies found that loci training induced increases in the cortical volume in episodic memory networks that were comparable in the SMI and normal control groups.3 The normal control subjects in the present study also showed significant increases in hippocampal volume after training. However, a recent systematic review of computerized cognitive training in cognitively healthy older adults found diverse results, with scores for the training effect ranging from 0.19 to 7.14 for neuropsychological software interventions, depending on the age of the participants and the type and duration of the interventions.1
We hypothesize that the lack of neuroimaging changes in the SMI and normal control groups in our study was due to insufficient statistical power as well as ceiling effects of the measures used. The lack of statistical power is a feasible explanation given the small number of subjects (six in the SMI group). Moreover, relative changes in the neuroimaging characteristics of patients who still have normal cognitive function might not be as significant as those in the MCI group, and would therefore be obscured by a ceiling effect. Indeed, a previous study suggested that subjects with cognitive decline may benefit the most from cognitive training.33 Additionally, subjects with worse baseline cognitive function demonstrated greater improvements from so-called CognitFit training.34
The main limitation of our study is the small number of patients, and so the conclusions drawn should be regarded as preliminary. Furthermore, we followed up patients for only 12 weeks, and it is not clear if the improved cognition and neural activity would persist beyond this time frame. Our cognitive training program was designed to stimulate cognitive functioning in multiple domains simultaneously, which made it difficult to discern the exact effect on each cognitive domain by each training apparatus. However, our experiments reflect the complex situations encountered in everyday life that necessitate the utilization of more than one cognitive domain. Another limitation is that there was no active control group. Future studies that include an active control group should assess whether the results of the present study are reproducible.
One strength of our study is the multimodal assessment utilizing several neuroimaging tools that meant that we could detect any structural or functional changes caused by cognitive training, resulting in more-robust conclusions being drawn. Although the small number of patients in this study may be a limitation, few studies with larger numbers of patients have performed multimodal neuroimaging evaluations simultaneously. Furthermore, structured sessions with supervisors were conducted in this study to ensure that the training was more consistent. Finally, there were no dropouts during the study, and most of the subjects expressed satisfaction with the training programs. Compliance with training programs is likely to be an important factor for attaining the expected effects in clinical practice and research.
In conclusion, this study shows that computerized cognitive training can improve memory and frontal executive function in patients with MCI. This improvement was accompanied by structural and functional changes in the anterior cingulate cortex and the anterior insula. Our results suggest that computerized cognitive training may improve coping strategies for overcoming impaired cognitive resources, and may lead to the development of strategies for allocating and deploying these cognitive resources more efficiently. Finally, our study has provided further insight into the neural mechanisms underlying the improvements caused by computerized cognitive training.
 XML Download
XML Download