

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Tension-type headache (TTH) affects more people than any other type of headache.1 TTH has negative impacts on the quality of life and work performance, and increases the health-care costs for both the affected individuals and society as a whole.2 Because TTH is more common, its associated social burden of disability is greater than that caused by migraine.1
Insufficient sleep is a common and chronic persistent condition that is associated with various health problems such as cardiometabolic disease, mental health disorders, accidents, injuries, occupational errors, and noise exposure.3456 Insufficient sleep is also implicated in sleep disturbances including excessive daytime sleepiness, insomnia, and short sleep duration.7
While an intimate relationship between migraine and sleep disturbances has been documented, the role of sleep disturbances in TTH has only recently been examined. Insomnia has been found to be more prevalent among individuals with TTH than in those without headaches.8 An 11-year longitudinal cohort study found that individuals experiencing TTH had a higher risk of developing insomnia.9 Restless legs syndrome (RLS) is reportedly also more common in individuals with TTH than in individuals without headache.10 In contrast, the prevalence of excessive daytime sleepiness was similar in individuals with chronic TTH and those with chronic migraine.11
The aims of the present study were 1) to estimate the prevalence of TTH and insufficient sleep in the general Korean population, 2) to determine the clinical impact of insufficient sleep on subjects with TTH, and 3) to identify the relationship between insufficient sleep and TTH while adjusting for covariates such as sleep quality, sleep duration, sociodemographic factors, and psychiatric conditions.
Go to : 
METHODS
Population and survey process
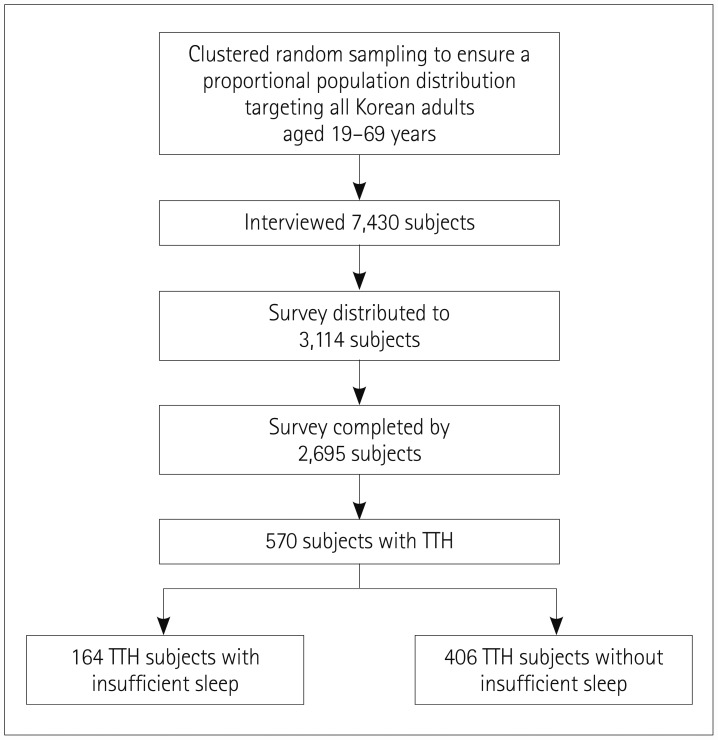
This study used data from the Korean Headache Sleep Study (KHSS). The detailed procedure of the KHSS has been described previously.12 In brief, the KHSS surveyed the headache and sleep status in Koreans aged 19 to 69 years as a nationwide, cross-sectional, and population-based survey that applied a two-stage clustered random sampling method. The survey was conducted in all Korean territories except for Jeju-do, and the sample of subjects was proportionally representative of the general Korean population (Table 1).
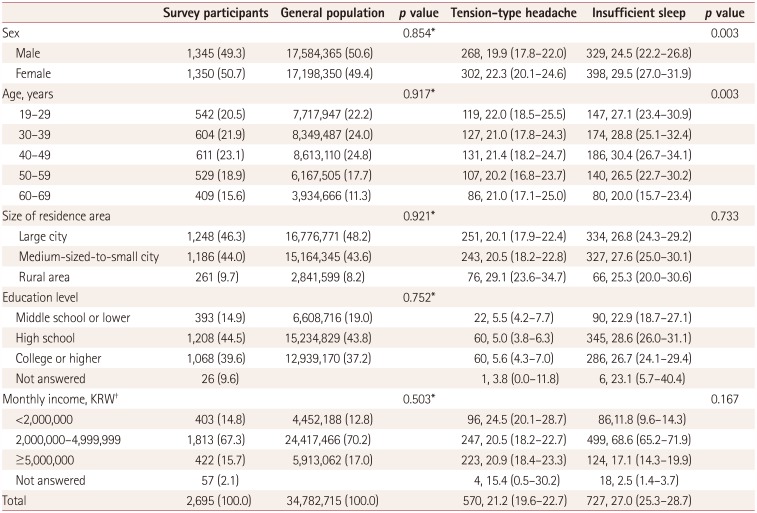
Table 1
Sociodemographic characteristics of the survey participants, the general Korean population, and cases identified as having tension-type headache and insufficient sleep
![]()
The survey was administered from November 2011 to January 2012 via door-to-door visits and face-to-face interviews using a questionnaire. All of the interviewers were employed by Gallup Korea (Seoul, Korea) and had previous experience of administering social surveys, but they were not medical professionals. The study was conducted with permission from the Institutional Review Board and ethics committee of Hallym University Sacred Heart Hospital (IRB No. 2011-I077). All subjects provided written informed consent.
Assessment of TTH
TTH was assessed using the current version of the International Classification of Headache Disorders (ICHD-3 beta), and diagnosed when criteria B to D for infrequent TTH (code 2.1) were met: B, symptom duration from 30 minutes to 7 days; C, at least two of the four characteristics present (bilateral location, nonpulsating nature, mild or moderate severity, and not aggravated by physical activity); and D, attacks associated with neither nausea or vomiting and no more than one of photophobia and phonophobia.13 The frequency criterion (criterion A) was not used in this study to diagnose TTH, and hence all cases of infrequent (code 2.1), frequent (code 2.2), and chronic (code 2.3) TTH were included. Subjects who satisfied all except one of the diagnostic criteria for migraine (ICHD-3 beta) were defined as having probable migraine (PM). Any subject who satisfied the criteria for both PM and TTH was diagnosed as TTH.13 The questionnaire for diagnosing TTH was validated by comparison with diagnoses confirmed by doctors via additional telephone interviews. The sensitivity and specificity of the questionnaire for a TTH diagnosis were 86.2% and 75.5%, respectively.14
Assessments of average sleep duration and short sleep duration
The average sleep duration was calculated as:
Short sleep duration was defined as existing when the average sleep duration was 6 hours or less.
Assessments of sleep need and insufficient sleep
We assessed sleep need by asking subjects the following question: “How long do you want to sleep in a day?” Insufficient sleep was defined when the discrepancy between sleep need and average sleep duration was at least 1 hour.7
Assessment of insomnia, poor sleep quality, and risk of sleep apnea
The Insomnia Severity Index (ISI) was used for diagnosing insomnia. The ISI is a simple 7-item questionnaire that assesses the severity of insomnia,15 and a subject with an ISI score of 10 or more is defined as having insomnia.16 We used the Pittsburgh Sleep Quality Index (PSQI) to evaluate sleep quality,17 with subjects scoring 6 or more in the PSQI considered to have poor sleep quality. The Berlin Questionnaire (BQ) was used to assess the risk of sleep apnea. The BQ was developed to screen sleep apnea based on risk factors, and it comprises ten items in the following three categories: snoring and cessation of breathing, symptoms of excessive daytime sleepiness, and a history of hypertension.18 A BQ score of ≥2 indicates a high risk of sleep apnea. The Korean version of the BQ has shown a sensitivity of 72% and a specificity of 43% for detecting moderate or severe sleep apnea.19
Assessment of anxiety and depression
The Goldberg Anxiety Scale (GAS) consists of four screening items and five supplementary items.20 Individuals who answered positively to at least two of the screening items and at least five of the scale items were defined as having anxiety. The Korean GAS was found to have a sensitivity of 82.0% and a specificity of 94.4% for diagnosing anxiety.21 Depression was assessed using the Patient Health Questionnaire-9 (PHQ-9),22 with a PHQ-9 score of 10 or more indicating the presence of depression. The Korean version of the PHQ-9 has shown a sensitivity of 81.1% and a specificity of 89.9% for diagnosing depression.23
Statistics
Kolmogorov-Smirnov tests were used to determine whether the sample data conformed to a normal distribution. When normality was confirmed, continuous variables were analyzed using Student's t-test. Categorical variables were compared using the chi-square test. Univariable analyses were used to assess the relationships between insufficient sleep and the variables such as sociodemographic factors (sex, age, size of residence area, and education level), psychiatric conditions [anxiety (GAS) and depression (PHQ-9 ≥10)] and sleep-related factors [insomnia (ISI ≥10), poor sleep quality (PSQI ≥6), short sleep duration (average sleep duration <6 hours per day), and high risk of sleep apnea (BQ score ≥2)]. We subsequently performed multivariable analyses to identify the independent effects of insufficient sleep on TTH. Sociodemographic factors were adjusted in the first step (Model 1), and analyses in the second step (Model 2) were completed after also adjusting for psychiatric conditions (anxiety and depression) in addition to the factors adjusted in Model 1. In the third step (Model 3), sleep-related factors (insomnia, poor sleep quality, short sleep duration, and high risk of sleep apnea) were added to the sociodemographic factors of Model 1. The fourth step (Model 4) included all adjusted factors from the first three models.
All statistical analyses were performed using the Statistical Package for Social Sciences 22.0 (SPSS 22.0, IBM Corp., Armonk, NY, USA), and p values <0.05 were regarded as indicating statistical significance.
Go to :
RESULTS
Survey
Prevalence of TTH and insufficient sleep
Among the 2,695 included subjects, 570 (21.2%) had TTH and 1,422 (52.8%) did not have headaches. Additionally, 113 of the 570 (19.8%) subjects with TTH fulfilled the criteria for PM.
Insufficient sleep—needing at least 1 hour more of extra sleep in addition to the current average daily sleep—was reported by 727 (27.0%) subjects. Insufficient sleep was more prevalent in women than in men (29.5% vs. 24.5%, p=0.003) (Table 1), and was most prevalent in the age range of 30–50 years and least prevalent in those aged 60–69 years. The prevalence of insufficient sleep did not differ significantly with size of residence area or education level.
Average sleep duration, short sleep duration, and sleep need
The average sleep duration, prevalence of short sleep duration, and sleep need of subjects with TTH and those without headaches are summarized in Table 2. The average sleep duration of all subjects was 7.3±1.2 h daily, and did not differ significantly between subjects with TTH and those without headaches (7.2±1.2 h vs. 7.3±1.2 h, p=0.087). A short sleep duration was present in 469 (17.4%) subjects, and was more common in subjects with TTH than in those without headaches (19.6% vs. 15.9%, p=0.048). The sleep need differed marginally (but not significantly) between TTH subjects and those without headaches (7.9±1.2 h vs. 7.8±1.3 h, p=0.068).
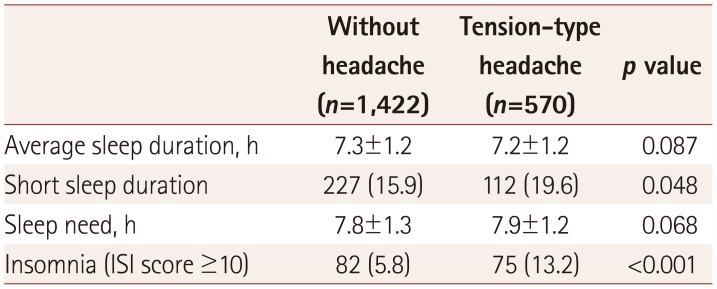
Table 2
Average sleep duration, prevalence of short sleep duration (average sleep duration of <6 h), sleep need, and insomnia in participants with tension-type headache and those without headache
![]()
Insomnia, poor sleep quality, anxiety, and depression
Insomnia was present in 290 (10.8%) of the 2,695 subjects, and was more common in subjects with TTH than in those without headaches (13.2% vs. 5.8%, p<0.001) (Table 2). Poor sleep quality was present in 715 (26.5%) subjects, and was more common in subjects with TTH than in those without headaches (36.3% vs. 26.2%, p<0.001). Anxiety and depression were present in 268 (9.9%) and 116 (4.3%) subjects, respectively. Subjects with TTH were much more likely than those without headaches to have anxiety (9.5% vs. 5.3%, p=0.001) and depression (4.2% vs. 1.8%, p=0.002).
Insufficient sleep and TTH
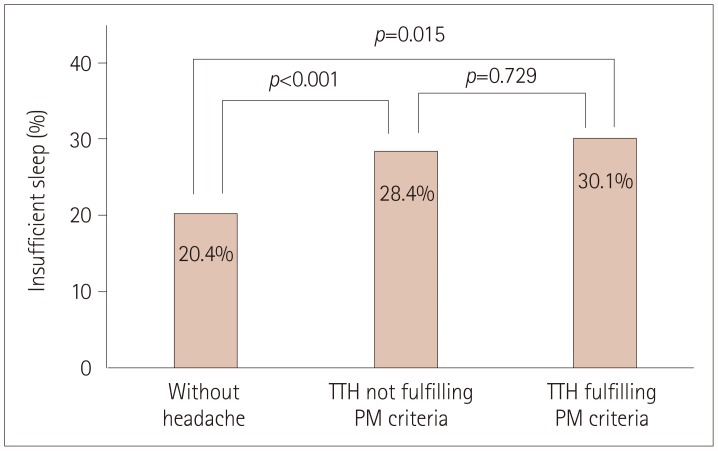
Insufficient sleep was more prevalent in subjects with TTH than in those without headaches (28.8% vs. 20.4%, p<0.001), but its prevalence did not differ between subjects with TTH who fulfilled the criteria for PM and those who did not fulfill the criteria (30.1% vs. 28.4%, p=0.729) (Fig. 2). The rate of insufficient sleep differed between non-PM TTH subjects and those without headaches (28.4% vs. 20.4%, p<0.001). The frequency of TTH attacks had no significant effect on insufficient sleep. The prevalence of insufficient sleep in subjects with <1 attack per month (26.6%) did not differ significantly from that in subjects with 1–14 attacks per month (32.3%, p=0.145) or from that in subjects with >15 attacks per month (21.4%, p=0.668).
Population characteristics and clinical manifestations of TTH according to the presence of insufficient sleep
The age and sex distributions were not significantly related to the presence of insufficient sleep. The headache characteristics, headache frequency per month, and risk of sleep apnea did not differ significantly with the existence of insufficient sleep. In contrast, the score on a visual analogue scale for pain intensity, the Headache Impact Test-6 score, and the prevalence rates of anxiety, depression, insomnia, short sleep duration, and poor sleep quality were all significantly higher in TTH subjects with insufficient sleep than in those with sufficient sleep (Table 3).
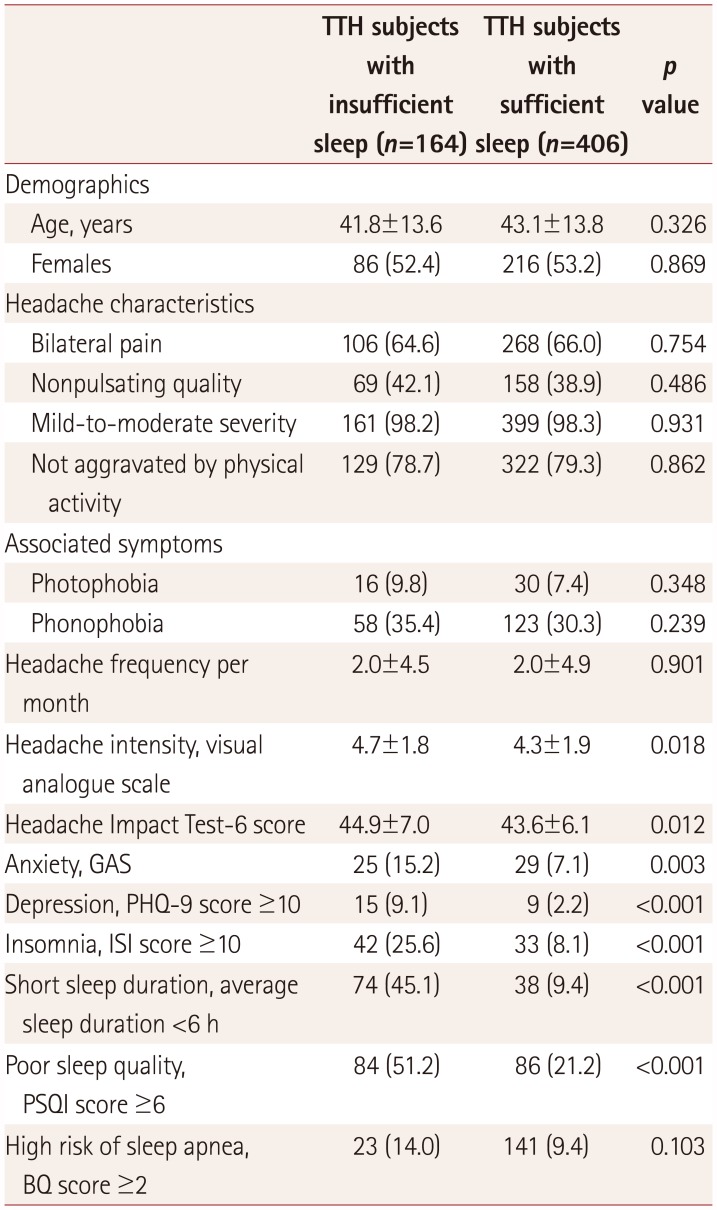
Table 3
Demographics and clinical presentation of subjects with TTH according to the presence of insufficient sleep
![]()
Univariable and multivariable analyses of insufficient sleep in subjects with TTH
Univariable analyses showed that anxiety [odds ratio (OR)=2.3, 95% CI=1.3–4.1], depression (OR=4.4, 95% CI=1.9–10.3), insomnia (OR=3.9, 95% CI=2.4–6.4), poor sleep quality (OR=3.9, 95% CI=2.7–5.8), and short sleep duration (OR=8.0, 95% CI=5.1–12.5) were significantly related to insufficient sleep (Table 4).
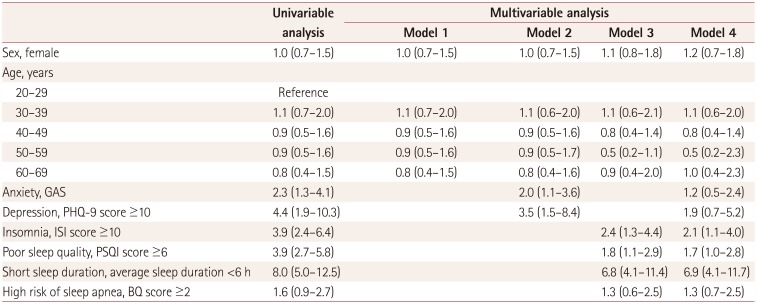
Table 4
Results from univariable and multivariable analyses of insufficient sleep in subjects with tension-type headache adjusted for sociodemographics, anxiety, depression, insomnia, poor sleep quality, short sleep duration, and high risk of sleep apnea
Data are odds ratio (95% CI) values. Model 1: adjusted for sociodemographic variables (sex, age, size of residence area, and education level), Model 2: adjusted for sociodemographic variables, anxiety, and depression, Model 3: adjusted for sociodemographic variables, insomnia, poor sleep quality, short sleep duration, and high risk of sleep apnea, Model 4: adjusted for sociodemographic variables, anxiety, depression, insomnia, poor sleep quality, short sleep duration, and high risk of sleep apnea.
BQ: Berlin Questionnaire, GAS: Goldberg Anxiety Scale, ISI: Insomnia Severity Index, PHQ-9: Patient Health Questionnaire-9, PSQI: Pittsburgh Sleep Quality Index.
![]()
Multivariable analyses adjusted for sociodemographic factors (Model 1) indicated that sex and age were not significant predictors of insufficient sleep. Multivariable analyses including sociodemographic factors and psychiatric conditions (Model 2) revealed that anxiety (OR=2.0, 95% CI=1.1–3.6) and depression (OR=3.5, 95% CI=1.5–8.4) were significantly related to insufficient sleep. In Model 3 (adjusted for sociodemographic variables and sleep-related factors), insomnia (OR=2.4, 95% CI=1.3–4.4), poor sleep quality (OR=1.8, 95% CI=1.1–2.9), and short sleep duration (OR=6.8, 95% CI=4.1–11.4) were significant factors. The final model (Model 4, adjusted for sociodemographic factors, psychiatric conditions and sleep-related factors) revealed that insomnia, poor sleep quality, and short sleep duration had significant positive associations with insufficient sleep (Table 4).
Go to :
DISCUSSION
This study investigated the prevalence and impact of insufficient sleep in subjects with TTH in a general population-based setting. The main results of this study were that 1) more than a quarter of the subjects with TTH had insufficient sleep, which was a significantly higher proportion than for subjects without headaches, 2) the severity and clinical impacts of headache were significantly greater in TTH subjects with insufficient sleep than in those without insufficient sleep, and 3) insomnia, poor sleep quality, and short sleep duration were significant risk factors for insufficient sleep in subjects with TTH. Our findings suggest that insufficient sleep is prevalent among subjects with TTH and that appropriate management of sleep could help in the management of TTH.
This study found that the subjects with headaches did not sleep significantly more or less than subjects without headaches. This finding is similar to our previous finding that the average sleep duration did not differ significantly between migraineurs and subjects without migraine.24 Considering that migraine and TTH are two common primary headache disorders, our results indicate that the average sleep duration does not differ between subjects with primary headache disorders and those without headaches. We found that the sleep need of subjects with TTH differed marginally, but not significantly, from that of subjects without headaches. This result contrasts with migraineurs reportedly having a greater sleep need than non-migraineurs.25
Univariable analyses suggested that anxiety and depression were significant risk factors for insufficient sleep (Table 4), but this significance was lost after adjusting for insomnia, poor sleep quality, and short sleep duration. These findings suggest that insomnia, poor sleep quality, and short sleep duration are closely related to anxiety and depression, which is consistent with significant associations of anxiety and depression with sleep disturbances including insomnia, excessive daytime sleepiness, sleep apnea, RLS, and poor sleep quality also being reported previously.2627282930
One possible mechanism underlying insufficient sleep in subjects with TTH is the higher level of insomnia that they suffer from compared to those without headaches. A longitudinal study found that risk of developing TTH after 11 years was 40% higher in subjects with insomnia.9 Insomnia is strongly associated with poor sleep quality, and so the higher level of insomnia in TTH subjects may lead to higher levels of insufficient sleep. The rate of poor sleep quality is reportedly higher in subjects with TTH than in those without headaches.31 Another possible mechanism is the higher prevalence of a short sleep duration in TTH. Both sleep quantity and sleep quantity are key elements of sufficient sleep, and this study has demonstrated that short sleep duration is more prevalent in subjects with TTH than in those without headaches.
This study investigated insufficient sleep using subjective questions, which is consistent with several studies evaluating insufficient sleep by asking whether participants perceived that they did not get enough sleep.5 Another study assessed insufficient sleep by asking about the number of days during the previous month when the participants felt that they did not get enough sleep.6 In contrast, a Finnish-population-based study investigated insufficient sleep more objectively by evaluating the difference between the required and actual sleep times, with a difference of at least 1 hour considered to indicate insufficient sleep.7 We adopted the more-objective method employed by the Finnish study to assess insufficient sleep. The prevalence of insufficient sleep in the present study was similar to that in the Finnish study, which suggests that the present study properly evaluated insufficient sleep.
We used the ISI and PSQI to measure the levels of insomnia and sleep quality, respectively. The Korean versions of the ISI and PSQI had already been validated for the Korean language using data from hospital settings including various sleep disorders and normal controls.3233 However, those studies did not validate the instruments in population-based settings, and so we used the cutoff values for the ISI and PSQI that have been shown to be valid in population-based studies.1634
This study gives clues for the optimal management of sleep in individuals with TTH. Insomnia, poor sleep quality, and short sleep duration were found to be significant risk factors for insufficient sleep. Insomnia and poor sleep quality can be treated both pharmacologically and non-pharmacologically, while short sleep duration can be relieved by ensuring a sufficient sleep duration and good sleep hygiene. Although the rate of cooperation with the survey was less than ideal, we adopted a clustered sampling method that ensured a proportional population distribution—the distribution of sociodemographic factors (i.e., age, sex, size of residence area, and education level) was similar to that of the general Korean population. Previous studies of the prevalence of TTH in Asian countries (including Korea) found prevalence rates similar to that in the present study.135
This study was subject to some limitations. First, sleep characteristics—including sleep duration, presence of insomnia, sleep quality, and sleep apnea—were not assessed objectively using polysomnography or actigraphy, since these methods are not feasible in a population-based study. Instead, we assessed these parameters using validated instruments (e.g., the ISI, PSQI, and BQ). Second, although this study utilized a two-stage clustered random sampling method with a low sampling error to reflect the general population, the resulting smallness of the sample of subjects with headache could have negatively impacted the analyses in some subgroups. Third, we did not investigate the napping behaviors of or the hypnotic use by the participants, and therefore did not include these parameters in the analyses. The napping behavior may affect the average nocturnal sleep duration, especially in elderly populations.36 In addition, the hypnotic use is associated with longer sleep duration and poor sleep quality.3738 Further studies including the napping behavior and hypnotic use are needed to better clarify the relationship between insufficient sleep and TTH.
Notwithstanding the aforementioned limitations, this study also had several strengths. First, we used data from a large sample with clustered random sampling corresponding to the population distribution in order to make results more representative of the general Korean population. Second, we analyzed the influences of insufficient sleep together with those of additional sleep parameters (e.g., insomnia and poor sleep quality) and psychiatric conditions (e.g., anxiety and depression) in subjects with TTH. Third, the headache characteristics were examined in relation to the existence of insufficient sleep in subjects with TTH.
This is the first population-based study to have investigated the relationship between insufficient sleep and TTH. Our findings suggest that insufficient sleep affects more than a quarter of subjects with TTH, which is significantly higher than the prevalence in subjects without headaches. Moreover, subjects with TTH and insufficient sleep experience more severe headaches and a higher impact of headaches compared to subjects with sufficient sleep. Therefore, the proper evaluation and management of insufficient sleep may help to improve the management of TTH.
Go to :
 XML Download
XML Download