

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Several recent studies have found that stroke induces sarcopenia and other changes in skeletal muscle.12 A meta-analysis of muscle atrophy revealed that the muscle mass is significantly lower in paretic limbs than nonparetic limbs.3 A loss of muscle mass in the lower limbs following a stroke leads to a decrease in muscle strength of the knee extensors,45 and so it is important to prevent any such loss of muscle mass.
Paretic limbs reportedly exhibit not only a decrease in muscle mass (i.e., change in muscle quantity) but also an increase in intramuscular fat and other noncontractile tissue (i.e., change in muscle quality). The increase in intramuscular fat is related to a reduction in muscle strength independent of the loss of the muscle mass,67 which indicates the importance of investigating both the muscle quantity and quality in stroke patients. Previous studies utilizing computed tomography48 and MRI9 found that there is more intramuscular fat in the thigh and lower leg on the paretic side than the nonparetic side. Several recent studies investigated the qualitative changes in muscle in stroke survivors using ultrasound imaging as a noninvasive and safe method.1011 A higher echo intensity (EI) indicates increased intramuscular fat and connective tissues,12 and so ultrasound imaging represents an easily accessible and suitable technique for assessing the characteristics of individual muscles at various anatomical sites. Lee et al.10 found that the EI of the biceps brachii was higher in the paretic limb than the nonparetic limb in stroke survivors. More recently, Berenpas et al.11 reported that the EI values of the biceps brachii, forearm flexors, and medial head of the gastrocnemius were higher in paretic limbs than nonparetic limbs in stroke survivors. However, while qualitative changes in the upper and lower extremities in stroke survivors have been reported, to the best of our knowledge the qualitative changes in abdominal muscles in stroke survivors have not been examined previously.
It has been reported that the strength of trunk muscles is impaired in stroke patients,13 and that the ability to control the trunk after stroke is predictive of the future functional ability in performing the activities of daily living.14 It is therefore important to determine the quantitative and qualitative changes in abdominal muscles in stroke survivors. Measuring the muscle thickness (MT) and EI in both the abdominal and lower extremity regions simultaneously would clarify the differences in quantitative and qualitative muscle changes among different anatomical sites in stroke survivors. The present study therefore investigated MT and EI in the abdominal region, thigh, and lower leg in community-dwelling stroke survivors. The obtained information may be used to develop rehabilitation strategies for stroke survivors that could improve muscle function in their trunk and lower extremities.
Go to : 
METHODS
This study recruited stroke survivors living in the community and receiving ongoing rehabilitation care at day service centers. The protocol was approved by the ethics committee of Kobe Gakuin University Graduate School (IRB No. HEB20151202-1). Written informed consent was obtained from all participants before collecting any data. The following inclusion criteria were used for selecting participants: independent ambulation, unilateral stroke, and at least 6 months after stroke. Patients were excluded if they had dementia, orthopedic or chronic pain conditions, severe sensory impairment, or spasticity. The hemiparetic severity was measured using Lower-Extremity Fugl-Meyer (LE-FM) evaluations.1516 The present study only used synergy items (22 points) of LE-FM evaluations to grade the hemiparetic severity.16 In addition, a possible indicator of physical activity—the frequency of going out per week—was evaluated by asking the participants the following question: “How many times do you go out per week?”
Ultrasound measurements
MT and EI were measured using B-mode ultrasound imaging (LOGIO e, GE Healthcare UK, Chalfont, Buckinghamshire, England) with a multifrequency linear transducer (8–12 MHz). A gain of 58 dB and a dynamic range of 78 dB were applied for the measurements performed on all muscles. Dynamic focusing was applied to the appropriate depth for the muscle of interest. The following 11 muscles were assessed on both the paretic and nonparetic sides:171819 the rectus abdominis, external oblique, internal oblique, transversus abdominis, rectus femoris, vastus intermedius, vastus lateralis, vastus medialis, tibialis anterior, gastrocnemius, and soleus.
The measurement site of each muscle and the patient position during the measurement are shown in Fig. 1. The MT of each abdominal muscle increases during expiration, and so recordings were made at a consistent time point at the end of relaxed expiration during the measurements of abdominal MT.19 An adequate amount of contact gel was applied to the skin to avoid excessive compression of the dermal surface by the probe. The EI was evaluated by analyzing images displaying 256 grayscale levels using Image-J (version 1.37; National Institutes of Health, Bethesda, MD, USA), with the EI of each muscle expressed as a value between 0 (black) and 255 (white). All measurements were performed by the same investigator in order to minimize interobserver variations.
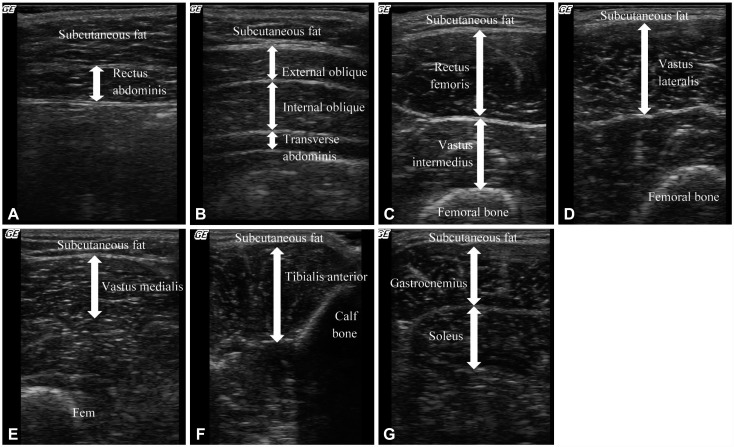 | Fig. 1Muscle ultrasound images and measurement sites and positions. A: Rectus abdominis, at 3 cm lateral to the umbilicus, with the patient supine. B: External oblique, internal oblique, and transverse abdominis, at 2.5 cm anterior to the midaxillary line at the midpoint between the inferior rib and the iliac crest, with the patient supine. C: Rectus femoris and vastus intermedius, at midway between the anterior superior iliac supine and the proximal end of the patella, with the patient supine. D: Vastus lateralis, at midway between the great trochanter and the lateral condyle of the tibia, with the patient supine. E: Vastus medialis, at 30% proximal between the great trochanter and the lateral condyle of the tibia, with the patient supine. F: Tibialis anterior, at 30% proximal between the lateral malleolus of the fibula and the lateral condyle of the tibia, with the patient supine. G: Gastrocnemius, at the medial head of the gastrocnemius at 30% proximal between the lateral malleolus of the fibula and the lateral condyle of the tibia, with the patient sitting. Soleus, at 30% proximal between the lateral malleolus of the fibula and the lateral condyle of the tibia, with the patient sitting.
|
Statistical analyses
Statistical analyses were performed using SPSS (version 20.0; SPSS Japan, Tokyo, Japan). Differences in all variables between the paretic and nonparetic sides were determined using paired Student's t-tests. For muscles for which the MT and EI differed significantly between the paretic and nonparetic sides, partial correlations were performed to evaluate the relationship with either the frequency of going out or latency from stroke onset, while considering the possible confounding factors of age, sex, body mass index (BMI), LE-FM score, and latency from stroke onset or frequency of going out. The criterion for statistical significance was p<0.05.
Go to :
RESULTS
A total of 32 stroke survivors (21 men and 11 women) aged 71.3±10.2 years (mean±SD; range, 43–87 years) participated. Their height, weight, and BMI were 1.62±0.08 m, 60.2±10.6 kg, and 23.0±3.3 kg/m2, respectively. The latency from stroke onset was 68.2±60.5 months, the LE-FM score was 15.2±4.5 points, and the frequency of going out was 3.7±1.7 times per week.
Table 1 lists the MT and EI values of the abdominal and lower limb muscles on the paretic and nonparetic sides. Regarding MT, the rectus femoris, vastus intermedius, vastus lateralis, vastus medialis, and tibialis anterior were significantly thinner on the paretic side (p<0.05). The gastrocnemius, soleus, and all abdominal muscles showed no significant differences between the paretic and nonparetic sides. The EI values of the vastus intermedius, vastus lateralis, vastus medialis, and soleus were significantly higher on the paretic side (p<0.05). The EI values of the rectus femoris, tibialis anterior, gastrocnemius, and all abdominal muscles did not differ significantly between the paretic and nonparetic sides.
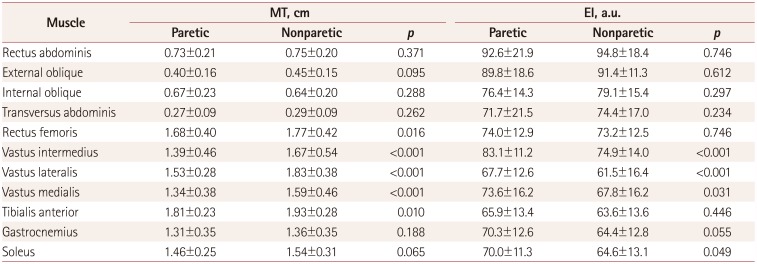
Table 1
MT and EI values of abdominal and lower limb muscles on the paretic and nonparetic sides in stroke patients
![]()
Correlation analysis revealed that the frequency of going out was significantly correlated with the MT values of the paretic rectus femoris (r=0.421, p=0.026), vastus intermedius (r=0.582, p=0.001), and vastus lateralis (r=0.439, p=0.019) after adjusting for age, sex, BMI, and latency from stroke onset. Latency from stroke onset was significantly correlated with the MT of the nonparetic vastus lateralis (r=0.487, p=0.009) after adjusting for age, sex, BMI, and frequency of going out. The other muscles were not significantly correlated with the frequency of going out or the latency from stroke onset.
Go to :
DISCUSSION
To the best of our knowledge, the present study is the first to investigate changes in muscle quantity and quality in the abdominal, thigh, and lower leg regions using ultrasound in chronic stroke patients. It was found that the MT values of the quadriceps femoris and tibialis anterior were lower and the EI values of the vastus intermedius, vastus lateralis, vastus medialis, and soleus were higher in the paretic limb than the nonparetic limb. Conversely, none of the abdominal muscles showed any significant changes in either MT or EI. Additionally, we observed significant associations between the MT values of the paretic rectus femoris, vastus intermedius, and vastus lateralis and the frequency of going out, as well as between the MT of the nonparetic vastus lateralis and the latency from stroke onset.
Previous studies have found lower muscle mass and higher intramuscular fat or noncontractile tissue in the lower extremities in stroke survivors.48911 The present study found significant differences between the sides of the lower leg muscles only for the MT of the tibialis anterior and the EI of the soleus. In contrast, there were substantial differences for the quadriceps, particularly in the vastus muscles, for which the MT was 13.3–14.9% lower and EI was 11.3–13.9% higher on the paretic side.
Atrophy of the quadriceps muscles in stroke survivors might be associated with a reduction in physical activity. The quadriceps are the lower limb muscles that are particularly susceptible to age-related loss of muscle mass.202122 Abe et al.2122 speculated that a reduction in physical activity with advancing age may contribute to the loss of muscle mass in the quadriceps.
Physical activity is significantly lower in stroke survivors than in healthy older individuals23 and is associated with physical functioning,24 muscle cross-sectional area,25 concentric strength,26 and the prevention of secondary complications27 Hachisuka et al.25 found a strong correlation between physical activity—quantified as the number of steps per day— and muscle fiber diameter of the vastus lateralis in stroke survivors. Therefore, the thinner quadriceps femoris and its higher EI observed in the present study might have been caused by reduced physical activity. The frequency of going out per week was positively correlated with the MT values of the rectus femoris, vastus intermedius, and vastus lateralis on the paretic side after adjusting for age, sex, BMI, latency from stroke onset, and LE-FM score. In healthy adults, the weekly frequency of performing activities including walking, exercise, and sport has been used as a measure of physical activity.282930 Although the present study did not ask the purpose of going out, it is possible that the frequency of going out represents a simple alternative parameter for measuring the extent of physical activity in stroke survivors. However, the EI values of the quadriceps and other muscles were not found to be related to the frequency of going out. Clarifying the association between physical activity with EI may require the use of a measurement device for actual physical activity (e.g., an accelerometer) in future studies. It was particularly interesting that a positive association was also observed between the MT of the vastus lateralis on the nonparetic side and the latency from stroke onset. It is possible that the long-term gait pattern associated with lower limb asymmetry3132 induces hypertrophy of the nonparetic vastus lateralis; this possibility should also be examined in future studies.
One strength of this study was related to it measuring the EI of the abdominal muscles. Kim et al.33 reported that the MT did not differ significantly between the paretic and nonparetic sides, which is consistent with the present study finding that the MT and EI of the abdominal muscles did not differ significantly between the two sides. The absence of a significant difference in the abdominal muscles could be attributed to them being innervated bilaterally. Previous studies have found the abdominal muscles to be spared following a stroke due to them being innervated bilaterally from the motor cortex.3435 Therefore, if a cerebral lesion occurs on one side only, the abdominal muscles might be not affected. However, Bohannon et al.13 reported that the strength of trunk muscles is impaired in stroke patients compared to healthy controls, which indicates the need to compare the MT and EI values of abdominal muscles between stroke survivors and healthy controls.
Our study was subject to some limitations. First, the number of subjects was small, and so type 2 errors might have been present. Second, our cross-sectional data did not allow us to identify any causal relationship between the frequency of going out and the MT or EI in the paretic leg. Third, it is not clear whether the frequency of going out reflects physical activity. Longitudinal studies are needed to identify whether objectively measured physical activity contributes to future changes in MT and EI in a large number of stroke survivors.
In conclusion, a thinner quadriceps and tibialis anterior and a higher EI of the vastus intermedius, vastus lateralis, vastus medialis, and soleus were observed in the paretic limb, with no significant changes in MT or EI of the abdominal muscles in stroke survivors. In addition, the MT values of the rectus femoris, vastus intermedius, and vastus lateralis on the paretic side were associated with the frequency of going out, while that of the vastus lateralis on the nonparetic side was associated with the latency from stroke onset. Although further investigation is required to confirm our findings, the present results provide valuable information for assessing and maintaining the abdominal and lower extremity muscles in stroke survivors.
Go to :
 XML Download
XML Download