

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Sleep problems have received considerable attention from the scientific community, especially in patients with Parkinson's disease (PD). The prevalence of sleep complaints is very high in PD patients, reportedly ranging from 35.1% to 98%.1234 These patients present with numerous sleep disorders such as insomnia, nocturia, rapid-eye-movement sleep behavior disorder, restless legs syndrome (RLS), circadian rhythm disorders, and excessive daytime sleepiness (EDS),5 which was the focus of the present study.
EDS is defined as the inability to sustain wakefulness during the usual awake periods of the day due to an uncontrollable need to sleep.6 Studies have found that 20–60% of individuals with PD exhibit EDS.4578 This wide variation in the prevalence of EDS seems to reflect variations in diagnosis criteria, intrinsic characteristics of assessed samples, and study designs. Nevertheless, previous studies have consistently found that the frequency of EDS is higher in patients with PD than in the general population.59
A myriad of factors has been implicated in EDS in PD, including a neurodegenerative process in specific brain regions implicated in regulating sleep and arousal.1011 The impact of nocturnal symptoms and other sleep disorders,121314 the presence of psychiatric comorbidities (especially depression and anxiety),51516 and the use of dopaminergic agonists have also been associated with EDS.717 There is some evidence indicating that sleepiness is mainly related to the pathology of PD rather than other concurrent factors. The application of polysomnography and daytime multiple sleep latency tests to 54 patients with PD preselected for sleepiness found that their EDS severity was not associated with dopamine-agonist treatment, age, disease duration, motor disability, total sleep time, periodic leg movement, apnea-hypopnea, or arousal indices, and so EDS was conceptualized as an integral feature of PD.8 This hypothesis was corroborated by a longitudinal study showing that the phosphorylated-tau/total-tau ratio in the cerebrospinal fluid is a strong predictor of EDS in PD. Moreover, EDS evolves more rapidly over time in PD than in healthy individuals.7
EDS has been associated with most of the motor and nonmotor symptoms in PD,5 including psychosis,18 falls,19 dementia,20 and fatigue.21 It is noteworthy that EDS is an important predictor of poor health-related quality of life2223 and markedly increases the burden experienced by caregivers.24 Therefore, the present study was designed to evaluate clinical factors associated with EDS in a sizeable sample of Brazilian patients with PD.
Go to : 
METHODS
Study design and participants
This cross-sectional study involved 85 patients with PD recruited from the Movement Disorders Outpatient Clinic, Hospital das Clínicas, Universidade Federal de Minas Gerais (UFMG), Belo Horizonte, Brazil. Patients met the diagnostic criteria for PD according to the criteria of the United Kingdom Parkinson's Disease Society Brain Bank.25 Patients were included if they were able to answer all of the clinical rating scales used in this study. A previous diagnosis of dementia, delirium, or neurological comorbidities, and a history of undergoing neurosurgical procedure were considered exclusion criteria.
The ethics committee of UFMG approved the study protocol (IRB No. ETIC 048/2006), and all participants provided written informed consent prior to study admission.
Clinical evaluation
All patients underwent a socioeconomic and clinical data evaluation followed by a psychiatric interview and a neurological examination. The Unified Parkinson's Disease Rating Scale (UPDRS)26 and the Modified Hoehn and Yahr Scale (MHYS)27 were used to assess the PD signs and symptoms and the disease stage, respectively. Complications of therapy were assessed using UPDRS part IV.26
Sleep features were assessed using the Epworth Sleepiness Scale (ESS)28 and the Parkinson's Disease Sleep Scale (PDSS).2930 The ESS is a self-administered questionnaire designed to measure the general level of daytime sleepiness, in which participants rate on a 4-point scale (from 0 to 3) their likelihood of dozing off or falling asleep while engaging in eight different activities.28 The PDSS is a visual analogue scale that assesses 15 commonly reported symptoms associated with sleep disorder in PD: overall quality of nighttime sleep (item 1), sleep onset and maintenance/insomnia (items 2 and 3), nocturnal restlessness (items 4 and 5), nocturnal psychosis (items 6 and 7), nocturia (items 8 and 9), nocturnal motor symptoms (items 10–13), sleep refreshment (item 14), and daytime dozing (item 15).29 The scores for each item range from 0 (symptom is severe and always experienced) to 10 (free of the symptom). The maximum cumulative score for the PDSS is 150, which would correspond to a patient without any sleep complaints.29 The PDSS items were grouped as proposed by Chaudhuri et al.29
All individuals underwent a cognitive evaluation, which included the Mini Mental State Examination (MMSE)31 and the Frontal Assessment Battery (FAB).32 The MMSE is widely test for cognitive screening, and encompasses different domains such as orientation, registration, attention and calculation, recall, and language.31 The FAB is a brief assessment tool for evaluating executive functioning. It comprises six subtests exploring frontal-lobe processes: conceptualization, mental flexibility, motor programming, sensitivity to interference, inhibitory control, and environmental autonomy. The score for each FAB subtest ranges from 0 (worst) to 3 (best), and the total FAB score is calculated as the sum of the subtest scores.32
The Beck Depression Inventory (BDI)33 and the Hamilton Rating Scale for Depression (HAM-D)34 were used to evaluate depressive symptoms. The BDI is a 21-item self-rating instrument that measures depressive symptoms, with the score for each item ranging from 0 to 3 according to its severity.32 The HAM-D is a 17-item scale designed to be applied by a health-care professional.34 This instrument rates the severity of the following depression-related symptoms on either a 5- or 3-point scale: mood, feelings of guilt, suicide ideation, insomnia, agitation or retardation, anxiety, weight loss, and somatic symptoms.
Anxiety symptoms were assessed using the Hamilton Anxiety Rating Scale (HAM-A), which consists of 14 items scored from 0 (not present) to 4 (severe).35 The Schwab and England Activities of Daily Living (SEADL) scale was used to assess functioning.36 RLS was diagnosed based on the criteria of The International RLS Study Group.37
Data analysis
The patients were initially divided into two groups according to the presence or absence of EDS, with EDS defined as a score higher than 10 points on the ESS as proposed by Johns28 in 1991. Categorical data are presented as frequency and percentage values, while continuous data are presented as mean±standard-deviation and median values.
All continuous variables were tested for conformity with a Gaussian distribution using the Shapiro-Wilk test. The two groups (presence vs. absence of EDS) were compared using Student's t test or the Mann-Whitney U test when variables did or did not conform to a normal distribution, respectively. Associations between dichotomous variables were assessed with Fisher's exact test.
Binary logistic regression using a backward elimination approach was performed to identify predictors of EDS. The following variables were included in the initial model: sex, age, education level, time since diagnosis, medications used (levodopa, antidepressant, and dopaminergic agonist), and scores for UPDRS total, MHYS, BDI, HAM-A, HAM-D, FAB, MMSE, and PDSS total. The goodness of fit of the logistic regression model was assessed using a receiver operating characteristics (ROC) curve.
Version 22 of SPSS (IBM Corp., Armonk, NY, USA) was used for all statistical tests, which were two-tailed and were performed using a significance cutoff of α=0.05.
Go to :
RESULTS
Thirty-four of our PD patients (40%) presented with EDS. Table 1 summarizes the sociodemographic and clinical data of the patients enrolled in this study. Most of the participants were male, married, and retired due to illness. There was no statistically significant intergroup difference in sex (p=0.825), marital status (p=0.068), or job situation (p=0.051). PD patients presenting with EDS were older than those without EDS (p=0.005). Both groups had a low education level, but it was significant lower in patients with EDS (p=0.020). Patients presenting with EDS were older at disease onset (p=0.002). There were no intergroup differences in the medications used, mean dose of levodopa, or side-effects profile. RLS was more prevalent in patients with EDS than in those without EDS (29.4% vs. 7.8%, respectively; p=0.015).
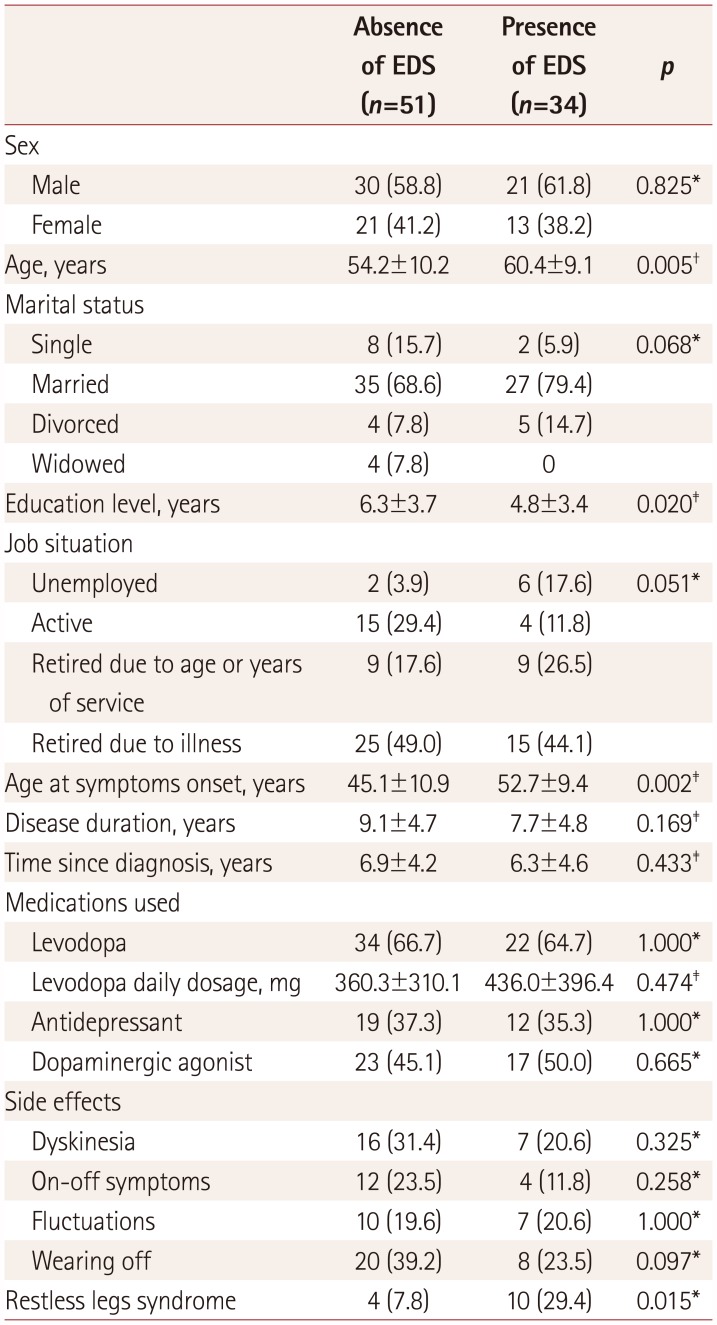
Table 1
Sociodemographic and clinical data of patients with Parkinson's disease with and without EDS
![]()
The scores on the clinical rating scales are presented in Table 2. The mean MHYS score did not differ between the two groups (p=0.659). Patients presenting with EDS had higher scores on UPDRS part I (p=0.001), UPDRS part II (p=0.022), BDI (p=0.001), HAM-A (p=0.003), and HAM-D (p=0.001) than patients without EDS. There were no significant intergroup differences in scores on the cognitive tests (FAB and MMSE).
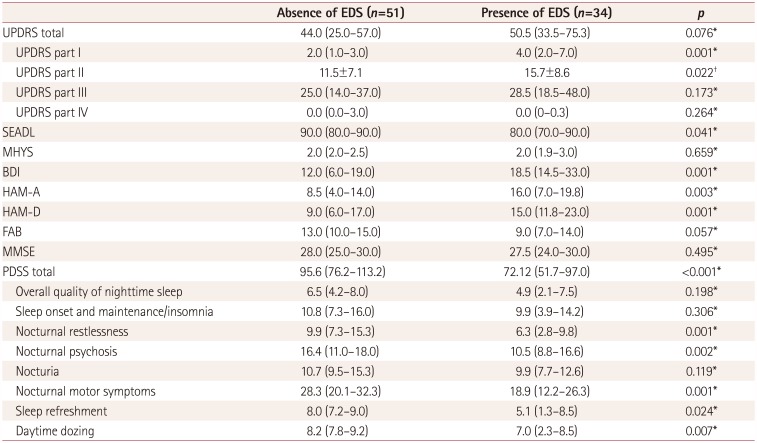
Table 2
Comparison of scores on the clinical rating scales between Parkinson's disease patients with and without EDS
Data are mean±standard-deviation or median (interquartile) values.
*Mann-Whitney U test, †Student's t test.
BDI: Beck Depression Inventory, EDS: excessive daytime sleepiness, FAB: Frontal Assessment Battery, HAM-A: Hamilton Anxiety Rating Scale, HAM-D: Hamilton Rating Scale for Depression, MHYS: Modified Hoehn and Yahr Scale, MMSE: Mini Mental State Examination, PDSS: Parkinson's Disease Sleep Scale, SEADL: Schwab and England Activities of Daily Living, UPDRS: Unified Parkinson's Disease Rating Scale.
![]()
Patients with EDS reported worse sleep quality as assessed by the PDSS total score (p<0.001), especially for nocturnal restlessness (p=0.001), nocturnal psychosis (p=0.002), nocturnal motor symptoms (p=0.001), sleep refreshment (p=0.024), and daytime dozing (p=0.007).
Backward stepwise regression revealed that older age, levodopa use, and lower score on the PDSS (i.e., worse sleep quality) were significant predictors of EDS. The results are presented in Table 3. The logistic regression model can be considered reliable since the predicted variability resulted in an area under the curve of 0.820 in the ROC analysis (Fig. 1). The obtained results were replicated when binary logistic regression was performed using forward selection, in that age, levodopa use, and PDSS total score were still significant predictors of EDS.

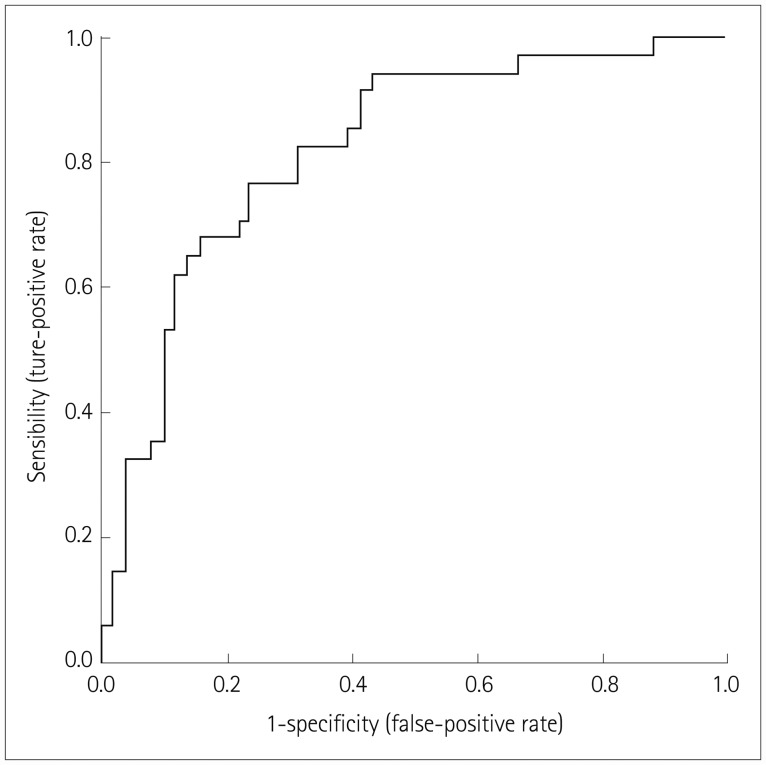 | Fig. 1ROC curve for the binary logistic regression. The logistic regression model provided a good fit to the data, since the area under the ROC curve was 0.820. ROC: receiver operating characteristics.
|
Table 3
Final binary logistic regression model (step 11) to predict excessive daytime sleepiness in Parkinson's disease patients
![]()
Go to :
DISCUSSION
To the best of our knowledge, this study has performed the most-comprehensive evaluation of EDS in a sample of Brazilian patients with PD. We confirmed that EDS is a common problem among patients with PD, with it affecting 40.0% of the evaluated subjects. The main predictors of EDS in PD were advanced age, levodopa use, and worse sleep quality.
The aging process results in both qualitative and quantitative changes in sleep patterns.3839 Typically there is a pronounced phase advance in the normal circadian sleep cycle, which results in a tendency to fall asleep and wake up earlier than usual, a longer sleep-onset latency, and a shorter total sleep duration.394041 Moreover, the elderly population exhibits changes in neurophysiological parameters of polysomnography, such as significant reductions in slow-wave activity and the range of sleep spindles.39 Together these alterations lead to worse sleep quality and an increase in daytime sleepiness and naps. Accordingly, the prevalence of EDS is relatively high in the elderly population, reportedly ranging from 13.6% to 25.2%.42434445 The current study has revealed that neurodegenerative diseases such as PD enhance these effects on sleep.
PD progression leads to worsening of motor symptoms74647 and consequently a need for higher doses of dopaminergic drugs.7 It is worth remembering that besides acting as a proxy for dopamine in PD, dopaminergic drugs can induce sleepiness. We found that levodopa use was a strong predictor of EDS, which corroborates the findings of other studies.574849 For example, de la Riva et al.49 found that 31% of patients treated with dopamine replacement therapy for at least 1 year developed EDS, in contrast to only 10% of untreated patients developing EDS. After following PD patients for 3 years, Amara et al.7 found that the levodopa equivalent dose differed between groups with and without EDS, especially during the second and third years of follow-up. The systematic review conducted by Chahine et al.5 showed that dopaminergic agonists induce EDS as a side effect, but the results with levodopa were unclear. It is noteworthy that, in contrast to previous findings of the use of dopaminergic agonists rather than levodopa being associated with EDS,5,7,17 we found that the use of levodopa (but not dopaminergic agonists) was a significant predictor of EDS in PD. This discrepancy between studies can be explained by differences in the characteristics of the included patients, such as their age, disease severity, and phenotype. Medication management might also influence the results. For example, the timing and dosing of dopaminergic medication intake relative to sleep might vary between the studied populations. Also, a higher levodopa equivalent dose has been associated with sleep disturbances, including EDS, especially when the medication is administered later in the day.5
EDS has also been considered a consequence of nighttime problems in PD.14 Corroborating this, we found a significant relationship between sleep quality (as evaluated by the PDSS) and EDS. In particular, nocturnal symptoms were more frequent among patients presenting with EDS than in those without EDS. An important aspect that must be taken into account when evaluating EDS in PD is the presence of RLS, since this is a sensorimotor disorder characterized by an urge to move associated with unpleasant sensations in the legs.50 This condition seems to be implicated in the development of EDS. We observed that RLS was more common among PD patients with EDS than those without EDS. It is particularly interesting that EDS appeared more frequently in PD patients with RLS than in controls with RLS.51
Depressive and anxious symptoms are common manifestations in patients with PD.4 The coexistence of depression and anxiety is also commonly observed in PD, being reported in from 34.12% to 41% of patients with PD.452 Corroborating previous findings, we observed that the scores on depressive and anxiety scales were worse for patients with EDS than for those without EDS. EDS may be understood either as a cause or as a consequence of anxious and depressive symptoms, and its treatment seems to be very important for improving the quality of sleep in these patients.5 However, EDS tends to be underrecognized and inadequately treated.553 It is worth emphasizing that although patients with EDS exhibited higher scores on the scales evaluating depressive and anxiety symptoms (Table 2), these findings were not supported by the logistic regression analysis.
Daytime sleepiness may directly affect the functioning of PD patients and contribute to the burden experienced by caregivers. In a nationwide survey in France, Ghorayeb et al.54 found that an impaired ability to perform the activities of daily living (ADL) was a risk factor for EDS. These data corroborate our findings that ADL impairment was more common in PD patients with EDS than in those without EDS, as evaluated using the SEADL scale. Nevertheless, the results obtained in the univariate analysis were again not supported by the binary logistic regression, with the SEADL score not being a significant predictor of EDS in our sample.
A major limitation of our study is its cross-sectional design, which made it impossible to determine the causality of any relationships between EDS and other variables. In addition, the lack of information about the physiological changes that occur during sleep (which could be obtained using either actigraphy or polysomnography) prevented the acquisition of a better understanding of the factors associated with EDS. However, the sample size and conducting comprehensive neuropsychiatric assessments can be regarded as strengths of our study. In addition, it should be noted that the use of multivariate analysis strengthened the reliability of our results. A univariate analysis alone might not be sufficient, especially for complex data sets, because it does not account for covariate effects. For example, although we found no significant difference in the frequency of levodopa use when we compared patients with and without EDS, levodopa use was a significant predictor of EDS when other variables (e.g., age) were considered in the analysis.
In conclusion, EDS in PD must be understood as a complex and multifactorial entity. Nighttime sleep problems, older age, and levodopa use are significant predictors of EDS in PD. A careful assessment and the management of sleep problems in PD patients might help to improve their quality of life.
Go to :
 XML Download
XML Download