

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Benign epilepsy of childhood with centrotemporal spikes (BECTS) is a common focal epilepsy syndrome with a good prognosis. It usually occurs before the age of 16 years.12 The treatment for BECTS is still controversial. Hughes reported that two-thirds of 96 articles on BECTS generally favored treatment with antiepileptic drugs (AEDs).3 The arguments for treatment are that patients with BECTS have a risk of daytime, generalized, or short-interval seizures and high probabilities of cognitive disability and learning deficits.45 Moreover, patients continue to show abnormal electroencephalography (EEG) findings even after seizure remission. These characteristics have led to the suggestion that all patients with BECTS require treatment.6 Several studies have proposed that BECTS can induce cognitive deficits and language ability impairment, and that antiepileptic drug should be considered for BECTS treatment.78910111213 In contrast, the arguments against treatment are that it may be unnecessary in most cases and potentially lead to worse outcomes than BECTS itself.1415 Hamada et al.16 maintained that patients with BECTS with isolated seizures at night do not require treatment.
The most commonly prescribed medications for patients with BECTS are oxcarbazepine, lamotrigine, topiramate, valproic acid, and gabapentin.17 We administered three representative drugs (lamotrigine, topiramate, and valproic acid) to patients with BECTS, and hypothesized that their language abilities would improve with antiepileptic treatment and that language abilities can be used to estimate changes in cognitive abilities. We attempted to quantify changes in language abilities after administering the three AEDs to patients with BECTS and to determine whether the improvement of language abilities is related to seizure control.
Go to : 
METHODS
Patients
From April 2000 to September 2015, 201 patients were newly diagnosed with BECTS at the Department of Pediatrics, Chonbuk National University. All of the patients had seizures that recurred at least twice and had typical clinical BECTS seizure patterns comprising vocalization and perioral focal seizures with or without secondary generalization, especially during light sleep. Patients who were not followed up within 12 months, did not complete one of the language tests or undergo EEG, or took two or more AEDs were excluded. The language abilities of the patients with BECTS were compared with those of a control group comprising 30 patients with no epilepsy or abnormalities in EEG who were of similar age and lived in the same province. The study was approved by the Institutional Review Board of Chonbuk National University Hospital (IRB No. 2016-04-032-007).
Methods
Our study involved a retrospective chart review of a prospectively collected database. The patients were divided into three groups according to the type of AED medication that they took. The lamotrigine group began treatment at a dosage of 1 mg/kg/day, which was titrated up to 7 mg/kg/day (or a maximum of 200 mg/day). Topiramate treatment began at a dosage of 1 mg/kg/day and ranged up to 5 mg/kg/day (maximum of 200 mg/day). Oxcarbazepine was administered at 10 to 30 mg/kg/day (or a maximum of 1,200 mg/day).
The patients included in this study had been treated with the same medication for at least 1 year. Clinical information, complete neurological examination results, EEG data (using sleep-deprived EEG, except in 29 patients), and our standardized language tests were applied just before the treatment and immediately after finishing the titration of the medication.18
Analysis of antiepileptic drugs (AED) effects
The effects of antiepileptic treatment were analyzed using the following two methods: 1) the seizure reduction rate within 1 year after treatment was assessed for each AED and 2) EEG responses were classified into three groups according to treatment. Secondary EEG examinations were performed using secondary language function tests. EEG abnormalities were classified into the following five categories according to the percentage of spikes per epoch: mild, mild to moderate, moderate, moderate to severe, and severe. The EEG readers were blinded to the treatment, and they judged the EEG spike percentage subjectively. EEG responsiveness was classified into three groups according to recovery status: 1) complete remission was classified as the complete disappearance of spikes on EEG, 2) in partial remission spikes were still observed but the EEG category was changed due to reduced spikes, and 3) no response was defined as either no improvement or aggravation in follow-up EEG.
Language tests
Language tests assessing important aspects of pragmatic ability were designed as reported previously.16
Test of Language Problem Solving Abilities (TOPS)
The Test of Language Problem Solving Abilities (TOPS) consists of 17 scenes and 50 questions, and it is designed to assess how the logical thinking process is expressed using highrank language skills. These questions were divided into the following three categories: ‘why’ questions about determining cause, ‘how’ questions about making inferences, and ‘what happens’ questions about predicting ability. The score for each test question depends on the length of the sentences, and ranges from 0 to 2, and so the top score for the entire test is 100. This examination was developed by the Seoul Community Rehabilitation Center.19
Mean Length of Utterance in Words (MLU-w)
The Mean Length of Utterance in Words (MLU-w) is used to count the number of words in each utterance. It is useful for measuring linguistic productivity and general language development. The total number of words was divided by the number of words in the questions in the TOPS. The MLU-w was used in the present study to determine whether taking a medication led to a change in the score for grammatical complexity.
Phonological test
A phonological test comprising the Urimal Test of Articulation and Phonology (U-TAP) was used to examine the 19 consonants and 10 vowels of the Korean language. The test was divided into word and picture sentence inspection sections. The tester obtained information regarding phoneme pronunciation following the presentation of a picture, and analyzed the phonemes based on the articulation.
Receptive language test
A receptive language test is a test of receptive vocabulary for individuals aged from 2 to 16 years. This test involves presenting patients with words such as an adjectives, nouns, or verbs, and the patient then matching one picture to four proposed example words. We applied the Preschool Receptive-Expressive Language Scale to preschool-age children and the Receptive and Expressive Vocabulary Test to older children. Each overall score was converted into the corresponding age in months.
Statistical analysis
Mean±SD values were calculated. Pearson's chi-square tests were used to compare the antiepileptic effects of each drug, while paired t-tests were used to compare language function between before and after taking a medication. A one-way analysis of variance was used to determine the relationship between language and EEG findings. Statistical significance was determined using SPSS 22.0 for Windows (IBM Corp., Armonk, NY, USA). Probability values <0.05 were considered statistically significant.
Go to :
RESULTS
Characteristics of the patients
One-hundred and twenty patients underwent both EEG and language testing within 1 year in this study. Eighty-one patients were excluded from the analysis: 23 due to incomplete data, 33 were lost to follow-up, and 25 had delayed data collection for the second time point. The 120 patients comprised 69 males and 51 females aged 7.9±2.4 years (age range from 36 months to 13 years). The age in the control group was 10.1±2.3 years. The patient group was found to have a delay of 1.3 month in the language test before starting treatment with anticonvulsants. The control group had an advance of 3 months compared to the reference age group but there was no significant difference between the two groups with unpaired t-test (p=0.179). It can therefore be assumed that there was no preceding language development delay in the patient group. The second examination was conducted as soon as possible after completing titration, which took 5.0±3.2 months.
Recurrence rates for patients taking AEDs
The recurrence rates within 1 year after AED treatment were 21.7% (n=5), 19.4% (n=12), and 11.4% (n=4) for patients taking topiramate, lamotrigine, and oxcarbazepine, respectively. There were no statistically significant differences in the recurrence rates among the groups (p>0.05).
Correlation between EEG responses and taking AEDs
Complete remission was achieved in 26.1%, 8.6%, and 14.5% of the patients taking topiramate, oxcarbazepine, and lamotrigine, respectively, and the proportions achieving partial remission showed a similar trend (13.0%, 8.6%, and 17.7%, respectively). As a result, complete or partial recovery occurred in 39%, 16%, and 32% of the patients. However, there were no significant differences among the three groups (p>0.05) (Table 1).

Table 1
Recovery rate in the EEG data after initiating antiepileptic drug use
![]()
Improvement in language ability according to drug taken
One-hundred and twenty patients participated in the receptive language test and the test of phonology, while 88 patients underwent TOPS and MLU-w testing. The scores for the four tests were compared in order to assess changes in the language ability, as presented below.
TOPS
The score for the TOPS is calculated using age in months. The overall mean age of patients undergoing the TOPS was 106.4 months. The topiramate group had the highest mean age among the groups, at 115.4 months, followed by 104.9 months for oxcarbazepine and 102.8 months for lamotrigine. Lamotrigine led to significant improvements in the ‘making inferences’ (from 14.2±5.3 to 15.5±5.4, p=0.009) and ‘predicting’ (from 9.1±4.6 to 10.1±4.3, p=0.017) categories, and in the total score (from 36.4±11.8 to 38.9±12.3, p=0.008), but no significant improvement was observed in the ‘determining cause’ category (from 13.1±3.5 to 13.3±3.7, p>0.05). In contrast, taking oxcarbazepine did not produce any significant difference in any category, but it led to a significant increase in total score (from 32.6±14.1 to 36.0±13.3, p=0.012). Taking topiramate also did not produce any significant changes in the three categories of ‘determining cause’ (from 12.7±4.4 to 11.6±4.4, p>0.05), ‘making inferences’ (from 13.5±5.0 to 13.2±5.7, p>0.05), or ‘predicting’ (from 8.8±3.6 to 8.9±4.6, p>0.05), or in the total score (from 34.9±12.0 to 33.7±13.0, p>0.05) (Table 2). Fig. 1 indicates that topiramate decreased the score while oxcarbazepine and lamotrigine increased the score.
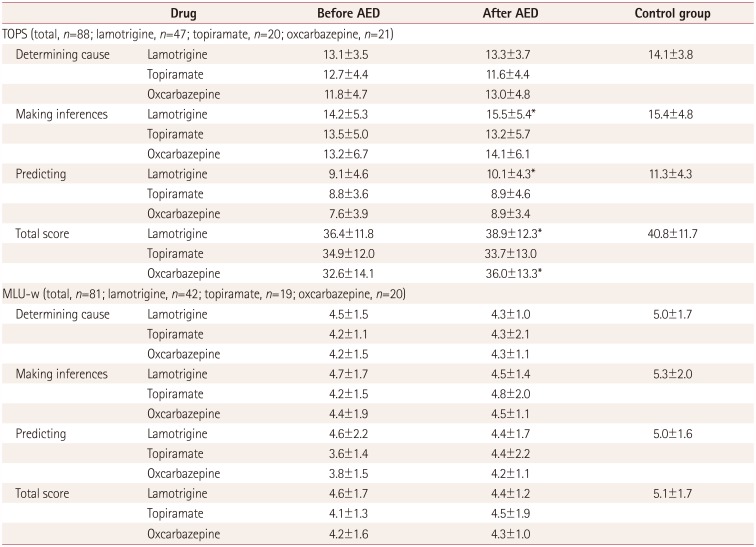
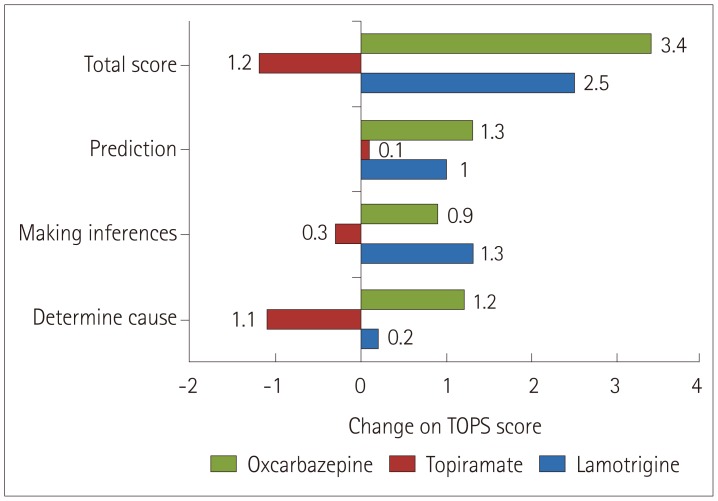 | Fig. 1Change in TOPS score between before and after taking an antiepileptic medication. TOPS: Test of Language Problem Solving Abilities.
|
Table 2
Changes in language function tests after initiating AED use
![]()
MLU-w in the TOPS
There were no significant differences in the MLU-w for any of the categories in the three medication groups. The patients used four syllables on average when answering the questions (p>0.05), while the subjects in the control group used an average of 5.1 syllables. Taking AEDs did not affect language expressiveness as assessed based on syllable use (Table 2).
Receptive language function
All three drugs led to better scores for receptive language function. The improvements when taking lamotrigine, oxcarbazepine, and topiramate occurred at 11.4, 7.3, and 5.4 months (p=0.001, p=0.001, and p=0.032) after the start of treatment, respectively. While the three drugs produced statistically significant differences, only lamotrigine led to meaningful improvement considering that the mean age difference between before and after drug administration was 9 months (Table 3).

Table 3
Changes in receptive language tests after initiating AED use
![]()
Phonology
The U-TAP in Korean was used to systematically evaluate pronunciation by dividing Korean words into consonants and vowels. Most of the children had scores close to 100%, and taking AEDs did not affect their pronunciation.
Correlation between EEG recovery and improvement in language ability
The relationship between EEG recovery and language function was analyzed for receptive language function, the TOPS, and MLU-w (Table 4 and 5). Correlations were found between EEG responses and the change in score between before and after the tests. In the receptive language test, the mean change for the complete-remission group was 8.7 months, which was smaller than the 12.8-month change found in the partial-remission group. This change did not differ significantly from that in the nonresponders group (p=0.445), and the same result was found for the TOPS and MLU-w (p>0.05). The performance in the four categories of the TOPS also was not correlated with the EEG group. When the ‘making inferences’ category was considered, lower responsiveness in EEG was correlated with a smaller change in score, although there was no statistically significant difference (p>0.05). Similarly, the MLU-w was not correlated with the EEG response.
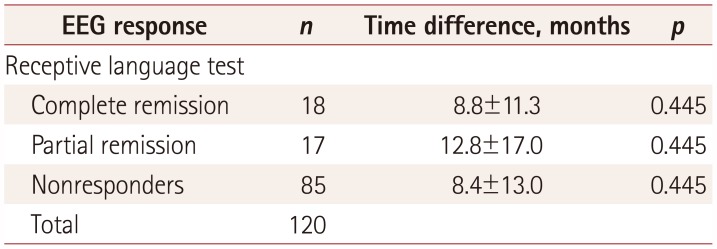
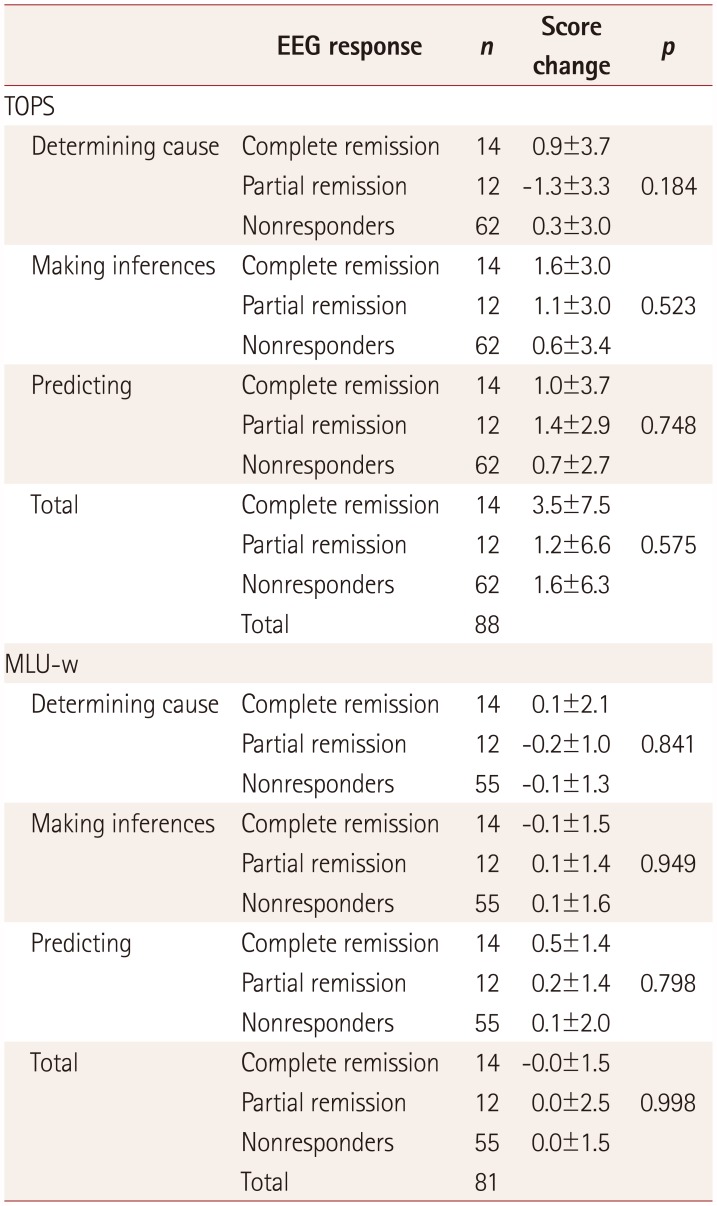
Table 4
Correlation between EEG responses and receptive language test results after initiating AED use
| EEG response | n | Time difference, months | p |
|---|---|---|---|
| Receptive language test | |||
| Complete remission | 18 | 8.8±11.3 | 0.445 |
| Partial remission | 17 | 12.8±17.0 | 0.445 |
| Nonresponders | 85 | 8.4±13.0 | 0.445 |
| Total | 120 |
![]()
Table 5
Correlation between EEG responses and language test results after initiating AED use
![]()
Go to :
DISCUSSION
The results of this study can be used to assess two hypotheses based on investigations of the recurrence rate, the EEG response level, and language testing according to the types of AEDs used in patients with BECTS undergoing monotherapy. Several researchers have already studied the relationship between cognitive development and language ability enhancement.2021222324 The underlying mechanisms were not well understood, and many children with language developmental delays showed impaired auditory processing.25 Also, working memory is necessary to perform complex cognitive activities and seems to be a specialized resource for language processing.26 Many patients with language problems appear to have cognitive weaknesses.27 We therefore first analyzed changes in cognitive ability using language tests in patients with BECTS categorized based on AED use.
Four types of language tests can be used to measure competence in different areas. Comprehension can be evaluated by testing receptive language and language-based thinking skills, such as clarification and analysis, using the TOPS. Language acquisition is tested using the MLU-w, and phonological disorders are tested using the U-TAP.1828 Lamotrigine and oxcarbazepine exert positive effects not only on receptive language but also in the TOPS. In particular, lamotrigine has the most-favorable effect on receptive language ability and leads to significant improvements in the scores for most of the categories of the TOPS; this drug therefore has the most-positive effect on language ability. The AED did not produce any observable effects on the MLU-w. When considering that auditory comprehension and naming can reflect cognitive processes, this finding suggests that lamotrigine has more-positive effects on language and cognitive abilities than do the two other AEDs administered to the patients with BECTS in this study.2930 This is consistent with a previous study finding that lamotrigine had no adverse effects on language ability and produce positive effects on cognitive ability and behavioral disability in patients with newly diagnosed epilepsy, as well as those with BECTS.31 To summarize, our data indicate that lamotrigine and oxcarbazepine had stronger effects on language ability, while topiramate was the most effective in improving EEG outcomes.
EEG recovery reflects the neurophysiological remission of epileptic spikes. We tested the hypothesis that the disappearance of epileptic spikes indicates improvement in cognitive ability and improvements in language test scores. We analyzed the positive correlation between EEG recovery and improvements in language ability. It was found that three drugs produced no statistically significant differences in recurrence and EEG recovery rate. In other words, there were no differences in their antiepileptic effects. There was also no correlation between the improvement in language function and EEG recovery. Berroya et al.32 reported that patients with BECTS had difficulty understanding and responding in language tests, despite their epilepsy being controlled. This suggests that EEG recovery does not affect cognitive development in areas such as receptive language and expressive thinking.
The effects of AEDs on language ability have been studied previously, and taking carbamazepine, levetiracetam, and topiramate reportedly affects language ability.33343536 However, the present study is significant in that few previous studies have investigated the three drugs simultaneously, especially in patients with BECTS. Moreover, because various biases such as age differences among individuals or the presence of speech therapy might affect the results obtained in language testing, we strived to perform a secondary follow-up as soon as AED titration was completed. Our analysis of patients with BECTS was carried out over a period of 3 to 12 months, and the results might accurately reflect the short-term impacts on BECTS. It has been reported that the seizure remission rate in patients with BECTS increases after treatment with an antiepileptic medication.37 The positive effects of lamotrigine and oxcarbazepine (but not topiramate) on linguistic and cognitive abilities might indicate that taking AEDs provides short-term benefits to patients with BECTS.
The limitations of this study include that the mean age of the patients was 26 months higher in the control group than in the BECTS group, which would have resulted in the language ability being better in the control group. Also, the analysis was limited by the retrospective nature of the study, since the data were collected prospectively. Finally, receptive language and articulation were not examined in the control group.
In conclusion, we recommend taking AEDs to minimize complications and to control seizures when EEG recovery is achieved within 12 months after antiepileptic treatment. In addition, we have shown that taking AEDs other than topiramate did not impair language ability.
Go to :
 XML Download
XML Download