

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Procedural memory is defined as the increased ability to perform a motor, visuomotor, or cognitive task with repeated exposition and fixed rules.123 Unlike hippocampal networks underlying declarative memory, corticostriatal and corticocerebellar pathways are involved in skill learning.4 Several stages of motor-cognitive learning have been described: an early stage with rapid improvement of both speed and precision, followed by a late learning stage in which further amelioration can be observed through repeated practice of a specific task, and finally a consolidation phase in which a spontaneous improvement in performance is observed even after the subject has not been exposed to the task for at least 6 h.56
Procedural learning has been studied extensively in patients with Parkinson's disease (PD) and has been shown to be equally impaired in the early phase,789 late-phase learning,10 and consolidation11 compared to age-matched healthy controls or patients with neurological disorders not associated with basal ganglia dysfunction (e.g., Alzheimer's disease and ruptured aneurysm of the anterior communicating artery). Procedural learning in PD has been negatively correlated with motor impairment, dopaminergic treatment,12 and axial motor involvement.13
123I-ioflupane (123I-FP-CIT) SPECT reveals presynaptic dopaminergic denervation in degenerative parkinsonism.14 We recently established local age-dependent semiquantitative uptake reference limits in our center15 and tested them on a cohort of patients with degenerative parkinsonism and dementia with Lewy bodies.161718 This produced a sensitivity of 98.7–100% compared with standard visual assessments.
In the present study we enrolled patients with early PD and results from 123I-ioflupane SPECT to study the procedural learning of a visuomotor task and to assess a putative correlation between their task performance and striatal 123I-ioflupane uptake. We aimed at enrolling PD patients in the early phase of the disease for the following reasons: such patients have milder motor impairment and are therefore more able to perform tasks, they do not have overt cognitive decline, and this is usually the period when diagnostic SPECT is performed.
Go to : 
METHODS
Study design and setting
We conducted a case–control study in which subjects performed a visuomotor skill learning task (mirrored drawing of star-shaped figures) on two consecutive days with four trials each. The study took place at the Laboratory of Cognitive Neurorehabilitation, Division of Neurorehabilitation, Geneva University Hospitals, Switzerland. Approval for the study was obtained from the Canton Geneva Ethics Committee (IRB No. 2016-01469), and all of the participants gave written informed consent. The trial is registered at ClinicalTrials.gov (NCT03076307).
Participants
Ten PD patients were recruited from the movement disorders outpatient clinic in the Division of Neurology, Geneva University Hospitals, based on the availability of dopamine transporter SPECT. Inclusion criteria were age ≥18 years, disease duration ≤2 years, and SPECT performed ≤6 months prior to inclusion. Exclusion criteria were a major depressive episode [Hospital Anxiety and Depression Scale (HADS) score ≥11],19 cognitive decline [Mini Mental State Examination (MMSE) score ≤26/30],20 debilitating rest, postural, or action tremor [≥2/4 in part III of the Movement Disorders Society Unified Parkinson's Disease Rating Scale (MDS-UPDRS III)],21 and ≥2/4 akinesia in the dominant upper limb on any corresponding item of the MDS-UPDRS III scale. Dopaminergic medication was not discontinued in PD patients who were receiving it, but we ensured that no changes were made during the 4 weeks prior to inclusion.
Twelve age-matched control subjects were recruited through advertisements in the Geneva University Hospitals and the Geneva Faculty of Medicine. The exclusion criteria were the presence of any neurological condition that could interfere with motor or cognitive function, actively taking medication that could interfere with cognitive abilities (any psychoactive drug, including antipsychotics, antidepressants, benzodiazepines, and sedatives), and the exclusion criteria applied to PD patients.
Prior to enrollment, the 22 included participants (10 PD patients and 12 controls) were evaluated by a neurologist (N.N.) who provided them with detailed information about the study and assessed demographics and baseline characteristics. Patients meeting the selection criteria signed an informed-consent form after being provided with written information about the study.
Procedures
The control subjects and PD patients performed a visuomotor skill learning task on a computer based on the mirrored drawing22 of black-line star-shaped figures on two consecutive days. This was implemented by reversing the effects of movements of the computer mouse: the arrow of the mouse on the screen moved to the right when the subject moved the mouse to the left, and vice versa. This task has been previously applied to healthy controls and PD patients.8 The error rate (ER) (total number of times moving inside or outside the boundary lines of the star) and time per trial (TPT) were assessed for all patients during four successive trials per day [trials 1–4 (T1–T4) on day 1 and T5–T8 on day 2]. The MDS-UPDRS III score was reassessed before the task on days 1 and 2. A questionnaire evaluating sleepiness (Karolinska Sleepiness Scale) was completed by the patient before each session, which was performed in the morning at the same time of day. PD patients receiving dopaminergic treatment were asked to take their medication as usual with the first dose in the morning at 1–2 h before performing the motor task in order to ensure that they were in the “on” motor state.
123I-ioflupane SPECT (DaTscan®, GE Healthcare, Glattbrugg, Switzerland) was previously performed in the clinical setting for all PD patients at a maximum of 6 months before study enrollment according to the manufacturer's instructions. The patients received 185 MBq of 123I-ioflupane in a slow intravenous injection and Lugol solution (or sodium perchlorate) for thyroid blockade. SPECT image acquisition started 4 h after administering 123I-ioflupane. All scans were acquired using the same triple-head gamma camera (GCA-9300A/UI; Toshiba Medical Systems, Oetwil am See, Switzerland) equipped with fan-beam, low-energy, high-resolution collimators. Details of the acquisition and reconstruction processes are available elsewhere.15
Local semiquantitative uptake reference values were established previously based on a large cohort of patients with nondegenerative conditions (n=182) and a normal (grade 0) visual assessment.15 Since we found a consistent linear decrease in striatal uptake with age, this parameter was included in the calculation of our patient-specific reference limits.
The cutoff points for volume of interest (VOI) uptake values were taken as the 5th percentile of this cohort:16 uptake was considered abnormal when it was below 3.93074–0.02156×age for the striatum, 3.79744–0.02168×age for the putamen, and 4.03099–0.02141×age for the caudate nucleus. For example, to be considered as having normal dopaminergic function, a 65-year-old subject is expected to have uptake values of >2.53 for the striatum, >2.39 for the putamen, and >2.64 for the caudate nucleus. The specific uptake calculated as a percentage relative to age-dependent reference limits was obtained for each PD patient (e.g., a striatal uptake of 1.84 in a 68-year-old subject is 74.8% of the age-specific reference limit of 2.46). An asymmetry index (AI) between the right and left VOI uptake values was calculated according to the usual formula: [(right-left)/(right+left)]×2×100.
We also segmented the putamen into its anterior and posterior parts. Preprocessing was performed with the Statistical Parametric Mapping software (SPM12, Wellcome Trust Centre for Neuroimaging, London, UK; http://www.fil.ion.ucl. ac.uk/spm/software/SPM12/), running on MATLAB (R2017a version 9.2.0, MathWorks, Sherborn, MA, USA). This included approximate manual image reorientation and positioning according to a T1-weighted MRI template available in the SPM toolbox. Images were spatially normalized to a 123I-ioflupane SPECT template.23 The anterior and posterior parts of the putamen were identified in the Talairach atlas, and its corresponding Montreal Neurological Institute coordinates were used to create spherical 4-mm and 5-mm masks for the posterior and anterior parts of the putamen, respectively.24 Uptake values were extracted using the Wake Forest University Pickatlas Software (version 3.0.5; Winston-Salem, NC, USA) toolbox running on SPM12.25
Outcome measures
The primary study outcome was the correlation between procedural motor skills performance indices (for TPT and ER) and striatal VOI uptake in patients with PD. The secondary outcome was the presence or absence of a statistically significant difference in the task performance indices between control subjects and PD patients for learning and consolidation.
Statistical analysis
The required total number of patients was estimated using an a-priori power analysis with GPower software (version 3.1., Universität Heinrich Heine, Düsseldorf, Germany).26 Procedural tasks performed in various studies in the literature show that the improvement in motor skills when performing simple tasks such as repeating a sequence of digit buttons or a serial response-time task is 10–20% lower in patients with PD than in healthy age-matched subjects.111227
We estimated that the improvements in TPT and ER would be 20% lower in the PD group than the control group. Considering a two-mean, two-sample equality test with a power of 80% (beta), an alpha of 5%, and a 1:1 ratio, the sample-size calculation indicated that seven subjects were required in each group.
Statistical analysis was performed with Stata software (version 14.2, StataCorp, College Station, TX, USA). The distribution of the continuous variables was assessed with the Shapiro-Wilk test, and Student's t and Mann-Whitney U tests were applied accordingly. The chi-square test was applied to discrete variables. We used analysis of variance (ANOVA) to assess group and intervention (trial) effects. To measure learning, we contrasted the first two trials on day 1 (T1–T2) with the last two trials on day 1 (T3–T4) using a repeated-measures analysis of variance (rmANOVA) with trial (T1–T2/T3–T4) and group factors. To measure consolidation, we contrasted the first two trials on day 2 (T5–T6) with the last two trials on day 1 (T3–T4) using rmANOVA. ANOVAs were performed for ER and TPT separately.
We established subject-specific performance indices (expressed as percentages) for TPT, ER, and combined TPT and ER outcomes (combined index) using the following formula:

For example, the time index for consolidation was TPT (T5+T6)-TPT (T3+T4)/TPT (T3+T4), expressed as a percentage. The indices for TPT and ER are negative when the subject improves his/her performance over a given period. However, for clarity we mainly quote positive values and specify whether they constitute improvements or deteriorations for each parameter.
The correlations between nonparametric striatal VOI uptake and performance indices in PD patients were assessed with Spearman's rank correlation test. We also performed multiple linear regression to predict the outcome for VOI uptake and levodopa equivalent daily dose (LEDD), using the caudate nucleus, whole striatum, and putamen (both as a whole and separately for its anterior and posterior parts).
Go to :
RESULTS
Twenty-two potential participants were screened between October 28, 2016 and May 23, 2017, of which 19 were enrolled in this study (9 PD patients and 10 control subjects). Further investigations revealed that one of the PD patients had a longer-than-required disease duration. One control subject was unable to finish the task due to shoulder pain and one was not included due to not fully understanding the task.
The baseline characteristics of the participants are presented in Table 1. There was no significant difference between the PD and control groups regarding age, male/female ratio, educational level, MMSE score, or HADS score (both the total score and the subscores for depression and anxiety). The MDS-UPDRS III score differed significantly between controls (1.3±1.1, mean±SD) and PD patients (15.0±10.4, p=0.0002).
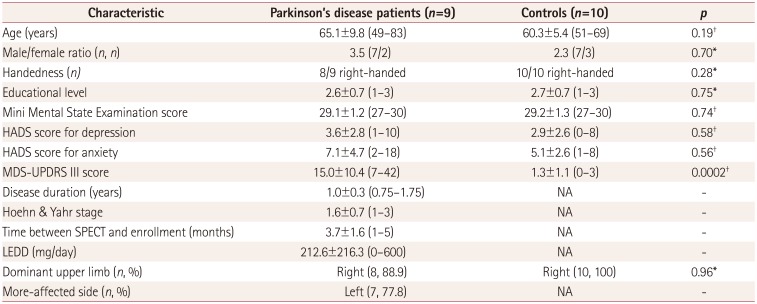
Table 1
Clinical baseline characteristics of the study participants
Data are mean±standard deviation (range) values except where indicated otherwise.
*Chi-square test, †Mann-Whitney U test.
HADS: Hospital Anxiety and Depression Scale, LEDD: levodopa equivalent daily dose, MDS-UPDRS III: part III of the Movement Disorders Society Unified Parkinson's Disease Rating Scale, NA: not available.
![]()
The MDS-UPDRS III score for PD patients was 15.0±10.4 (range 7–42) at baseline, 14.8±10.5 on day 1, and 14.6±10.4 on day 2 (p=1.00, Mann-Whitney U test). The Karolinska Sleepiness Scale score for PD patients was 3.1±1.2 on day 1 and 3.6±1.4 on day 2 (p=0.47, Mann-Whitney U test), and did not differ significantly from that for the control subjects either on day 1 (3.0±1.5, p=0.74) or on day 2 (2.8±0.9, p=0.25). There were no differences across groups and days regarding hours of sleep (PD patients: 6.6±1.7 and 6.9±1.3 h on days 1 and 2, respectively, controls: 7.0±1.4 and 6.7±1.3 h, all p>0.17).
The mean values of ER and TPT for the PD and control groups are shown in Figs. 1 and 2. For learning, rmANOVA with the factors of trial (T1–T2/T3–T4) and group did not reveal any group interaction [errors: F(1, 17)=0.28, p=0.60, time: F(1, 17)=0.07, p=0.79)]. There was a main effect of trial on the completion time [F(1, 17)=9.31, p=0.007]. However, for testing consolidation, rmANOVA with the factors of trial (T3–T4/T5–T6) and group revealed a trial×group interaction for both TPT [F(1, 17)=6.49, p=0.021] and ER [F(1, 17)=4.65, p=0.046]. PD patients showed significantly weaker consolidation than controls for both TPT (p=0.04) and ER (p=0.003).
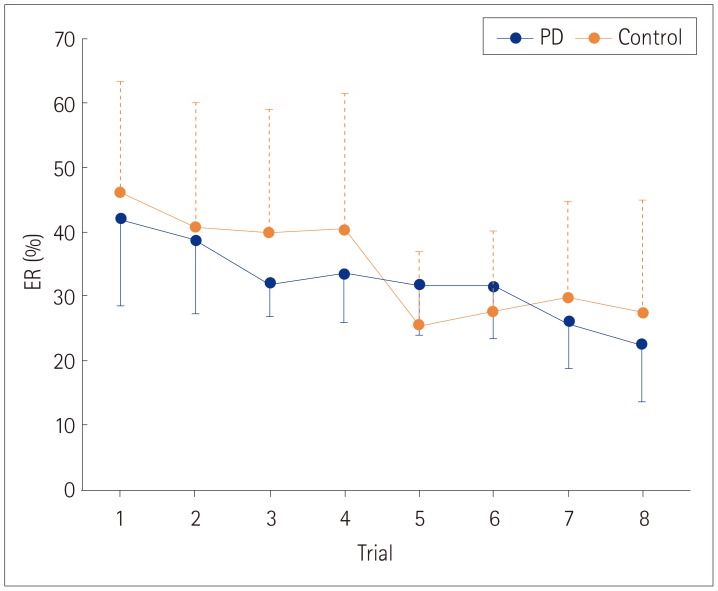
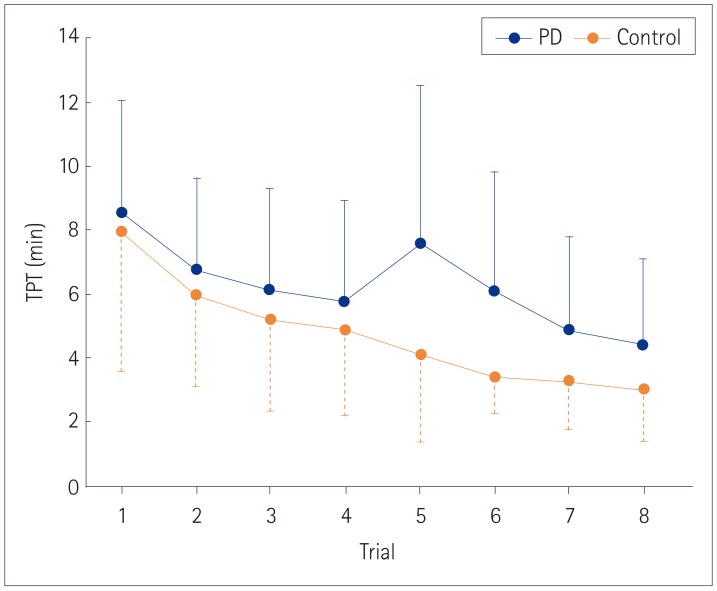
Regarding performance indices, the ER (p=0.63), TPT (p=0.79), and combined learning indices (p=0.98) did not differ between the two groups (all t-tests). However, there were significant differences in the consolidation indices for TPT alone (22.4±15.7% improvement for control vs. 11.0±32.1% worsening for PD, p=0.009) and the combined TPT and ER index (22.6±24.3% improvement vs. 5.2±27.3 worsening, p=0.03), but not for ER alone (22.8±35.7% vs. 0.7±29.3% improvement, p=0.16).
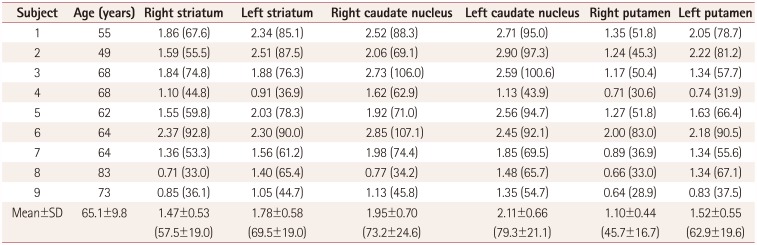
The semiquantitative 123I-ioflupane uptake in the putamen, caudate nucleus, and whole striatum in PD patients as well as the specific uptake preservation compared to previously obtained age-dependent reference limits are presented in Table 2. Spearman's rank correlation analysis of VOI semiquantitative values and procedural motor performance indices showed a strong negative correlation between TPT consolidation and the right caudate nucleus (Spearman's rho=−0.82, p=0.007) as well as for the whole right striatum (Spearman's rho=−0.67, p=0.049)—a higher uptake indicates a better consolidation index (Fig. 3). Multiple linear regression was performed to predict consolidation indices from VOI uptake and LEDD. These variables significantly predicted TPT consolidation index [F(2, 6)=12.18, p=0.0077, R2=0.8024]. The right caudate uptake improved the prediction (p=0.005, 95% CI=0.46–1.65) as did the right striatal uptake (p=0.024, 95% CI=0.22–2.25) after adjusting for LEDD. Conversely, LEDD was not a predictor of the consolidation index when controlling for caudate (p=0.25) or striatal (p=0.45) uptake. Since most of the included patients had left-predominant parkinsonism and thus a slightly lower right caudate nucleus uptake (1.95±0.70 vs. 2.11±0.66 on the left side, p=0.62), we added VOI AI as an independent variable to the linear regression and still found a significant correlation between right caudate uptake and the TPT consolidation index (p=0.026, 95% CI=0.16–1.59), whereas caudate AI (p=0.29) and LEDD (p=0.52) were not predictors of the performance. After adjusting for LEDD and striatal AI, right striatal uptake was not a significant predictor of the TPT index (p= 0.058, 95% CI=−0.05–2.13).
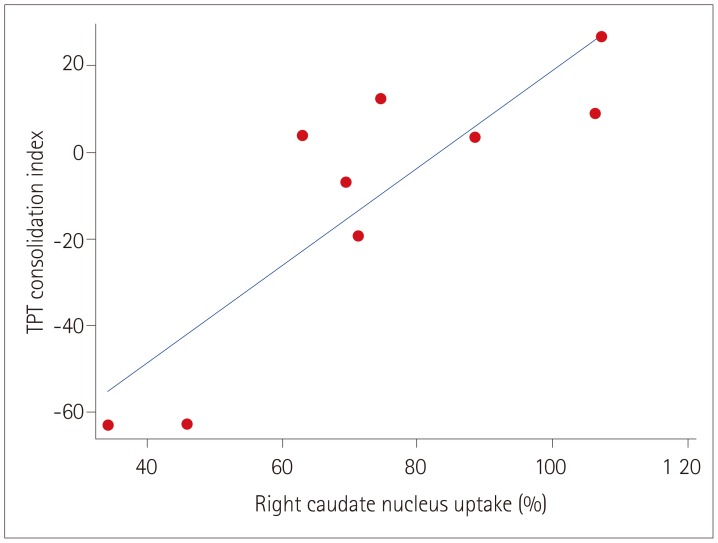 | Fig. 3Unadjusted correlation between the right caudate nucleus semiquantitative 123I-ioflupane uptake (compared to age-dependent reference limits) and TPT consolidation index for the nine Parkinson's disease patients included in the study (R2=0.7492). Positive values of the TPT index indicate improved performance from early on day 2 to late on day 1. TPT: time per trial.
|
Table 2
Volume of interest semiquantitative 123I-ioflupane uptake values for Parkinson's disease patients
![]()
The right caudate nucleus uptake was significantly higher in PD patients with improved TPT consolidation performance (87.8±19.4%) than in those without this improvement (55.0±18.0%, p=0.036, t-test).
We did not observe any significant correlations between VOI uptake and the other parameters (ER or combined consolidation indices, or ER, TPT, or combined learning indices) in multiple linear regressions correcting for LEDD (all p> 0.106).
Go to :
DISCUSSION
The present study indicates that consolidation for visuomotor skill learning is impaired in early PD. This finding is consistent with previous studies demonstrating that early basal ganglia dysfunction is not restricted to the motor domain, instead also involving procedural memory processes.112829
Dopaminergic 123I-ioflupane uptake has been found to be correlated with executive dysfunction,303132 but its association with procedural motor learning—which is directly implicated in the basal ganglia network—has not been reported previously. We observed that right caudate nucleus uptake was strongly correlated with the TPT consolidation index. This confirms the findings of previous fMRI and PET studies333435 showing activation or enhanced metabolism in the caudate nucleus (especially on the right side) for control subjects compared to PD patients. To a lesser extent, improvement of task performance with regards to the TPT consolidation index is also weakly correlated with the whole striatum uptake (Spearman's rho=−0.67, p=0.049). In our opinion, this result is mainly attributable to the contribution of its caudate nucleus portion.
The functional organization of the basal ganglia is usually subdivided into three distinct loops: motor, associative, and limbic.363738 The dorsolateral prefrontal cortex (DLPFC) and caudate nucleus are particularly involved in the associative circuit and play a crucial role in goal-directed learning,439 whereas the habitual system (automatic execution of learned motor plans) is thought to be mediated by the motor loop, which primarily involves the putamen.40 A dynamic fMRI study of visuomotor tasks found the differential involvement of corticostriatal subsystems at different stages of learning: during the initial phase of learning, which requires greater attention to the task, a more-pronounced activity was observed in the prefrontal cortex and caudate nucleus, whereas the dentate-thalamo-striate circuit showed increased activity in the later phases, when greater task automaticity prevails.41
As observed previously,34 caudate nucleus metabolism on 18F-FDG-PET is increased in control subjects compared to PD patients during the early phase of procedural learning, especially on the right side. Another study involving 18F-fluoropropyl-beta-CIT PET showed a correlation between sequence learning and caudate nucleus binding in PD, with a nonsignificant trend toward the right side.42 In addition to the presupplementary motor area, the right caudate nucleus has been described as the region mainly activated in an fMRI task involving spatial attention and motor preparation.43
Moreover, reactive inhibition—a mechanism that might be crucial in a reversed right-left movement task with a visual cue such as the one we applied to our subjects—showed strong right-lateralized fMRI activation of the DLPFC and inferior parietal lobule, as well as the ventrolateral prefrontal cortex and presupplementary motor area.44 Our study provides further evidence for a major right caudate nucleus involvement in procedural memory consolidation.
Some limitations of the present study must be recognized. First, SPECT was performed a few months before (3.7±1.6 months, range 1–5 months) rather than at the same time as the procedural motor task. Our observations on patients with degenerative parkinsonism and repeated SPECT identified an annual uptake loss of 5–10% (unpublished data), which is consistent with previous reports.45 It can therefore be estimated that a loss of <5% can be extrapolated between SPECT acquisition and visuomotor skill learning task in our patients, which we judged to be negligible. We therefore considered that striatal uptake values obtained in our PD patients represent a valid assessment of their dopaminergic status during the task.
Second, the study included only a small number of subjects. Since we established semiquantitative reference limits for VOI uptake specifically for our medical center, it was necessary to enroll PD patients for whom SPECT image acquisition and processing were performed in the same center. The required sample size was calculated before the study commenced, which revealed that seven subjects per group would be sufficient to observe the hypothesized effect. We indeed found a strong correlation between visuomotor consolidation and caudate nucleus uptake, but it is not excluded that other correlations (e.g., with learning) could have been observed in a larger cohort. It is unclear whether the lower right caudate uptake values found in our group with left-predominant parkinsonism may have played a role in the results. The linear regressions adjusting for VOI asymmetry still showed that the caudate nucleus (p=0.026) was a predictor of the TPT consolidation index, whereas the VOI AI was not. Moreover, the highly asymmetric nature of parkinsonism in PD is an inherent issue when determining lateralized brain functions, and it is possible that a larger and more-balanced group of patients with left- and right-predominant parkinsonism could have helped to resolve this issue.
Third, SPECT was not performed on the included controls, since we considered that cognitive testing was not a sufficient reason to expose them to ionizing radiation. Moreover, we mainly wanted to assess whether damage to the striatum is correlated with visuomotor performance, and therefore scanning subjects with supposedly intact dopaminergic pathways was futile.
Fourth, we decided to enroll PD patients with and without dopaminergic medication since this was an exploratory study and we were reluctant to modify their treatment and disrupt their hard-earned motor equilibrium. However, dopaminergic medication could not be considered a confounding factor since we were mainly interested in the patient-specific relative improvement (using indices) rather than the absolute improvement. In addition, multiple linear regression still showed a significant correlation between consolidation indices and striatal uptake when controlling for LEDD and, conversely, LEDD was not correlated with the performance when adjusting for VOI uptake.
Fifth, in contrast to other studies,8101328 we enrolled PD patients with a short disease duration (mean of 1.0 year) and mild motor impairment (mean Hoehn & Yahr stage of 1.6 and MDS-UDPRS III score of 15.0). Nevertheless, we showed that even in the early stage of the disease, consolidation is impaired in comparison to age-matched healthy subjects. A particularly interestingly finding was the similarity of early-phase learning (between the first and second parts of the performance on day 1) in the two study groups, which contrasts with other reports on PD subjects.8 This discrepancy might also be explained by the shorter disease duration: 1.0±0.3 years in the present study vs. 7.0±4.5 years in the previous one.8
It is unclear whether similar results would have been obtained if the subjects had performed the second session on the same day (but still >6 h after the first session) rather than on the next day. In other words, the specific role of sleep on visuomotor consolidation for PD4647 was not demonstrated in the present study.
In summary, we report that early-PD patients exhibit weaker consolidation in a visuomotor procedural task compared to age-matched healthy subjects and that their speed when performing a task is strongly correlated with the semiquantitative right caudate nucleus 123I-ioflupane uptake. These promising results open new perspectives for studying in vivo dopaminergic pathways and their association with impaired procedural memory in degenerative parkinsonism.
Go to :
 XML Download
XML Download