

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
Cognitive impairments are frequent symptoms of multiple sclerosis (MS). It is estimated that 40–70% of the patients have cognitive deficits,123 and information processing speed (IPS) is one of the most affected functions.3 IPS is a primary cognitive function, which is extremely important for the functionality of higher cognitive processes as it influences downward processes such as learning, memory, word retrieval, and executive function.4 Although no consensus on the definition of IPS as a neuropsychological construct has been reached, a prominent definition by Shanahan proposed a broad definition of processing speed as an underlying cognitive efficiency at understanding and acting upon external stimuli, which includes integrating low level perceptual, higher level cognitive, and output speed. Previous studies have analyzed the impact that processing speed has on emotional and clinical variables, and on different aspects of the MS patients' quality of life.45678
There are two tests widely used for evaluating IPS: the Symbol Digit Modalities Test (SDMT)910 and the Paced Auditory Serial Addition Test (PASAT).111213 In the SDMT an array of symbols that correspond to some numbers is presented to the evaluated. Later, the symbols are paired with empty spaces, and the evaluated must indicate the corresponding number as rapidly as possible. In the standard administration, the test has a written response task, followed by an oral response task, using the same stimuli.9 In the PASAT, according to the instructions, patients are asked to listen to successive numbers presented in a predetermined time interval and orally provide the sums of consecutive numbers as rapidly as possible.11 In MS research and clinical practice, the 3-s (PASAT-3) and 2-s (PASAT-2) versions of the interstimulus interval have been implemented. Both tests are part of two neuropsychological batteries used for assessing patients diagnosed with MS: the Brief Repeatable Battery of Neuropsychological Tests for Multiple Sclerosis214 and the Minimally Assessment of Cognitive Function in Multiple Sclerosis.15 The SDMT is also part of the Brief International Cognitive Assessment for Multiple Sclerosis.1617 A recent review describes that most of the studies on IPS of patients with MS are conducted through these two tests.4
Previous studies have analyzed the relationship between IPS and the clinical variables of patients with MS.1819202122232425 Regarding the relationship between processing speed and the patients' degree of motor disability, there are authors who claim that increasing motor disability is related to increased IPS slowing.212324 One of these studies23 has even found that of all the cognitive functions evaluated, processing speed was the most strongly associated with motor disability, measured by the Expanded Disability Status Scale (EDSS). However, there are other authors who did not find such relationship.26 With regard to disease evolution, there is a study that shows that the patients who had more years of disease evolution performed worse in IPS tasks,22 contrary to what was found by other authors.24 Regarding fatigue, some studies describe that in patients with MS fatigue is affected by IPS,20232527 whereas other studies dismiss such relationship.28 Another clinical aspect that has been widely reported in MS, is depression, the studies claim that there is a significant relationship between the patients' performance in processing speed tasks and the presence of depressive symptoms.1823272930
The symptoms of MS patients produce a negative impact on their psychosocial relationships, for this reason some authors have emphasized the role of social support in patient's life.303132 Regarding the specific relation between cognitive symptoms and social support, some authors claim that the IPS can affect their ability to face social situations,2133 but this is an area that has drawn little attention. Glanz et al.21 have analyzed the relationship between IPS and perceived social support, and found significant associations. Social support is usually described as a system of formal and informal relationships through which people receive material and psychological support to cope with their problems.29 The study of this variable has created interest due to the belief that people with better support have better health.
In recent years, there has been increasing interest in the study of IPS of patients with MS. However, the relationship between this cognitive function and the clinical variables of the patients is still under investigation. Also, the network of social support and its relationship with cognitive variables such as IPS is a field scarcely evaluated in this pathology. The aim of the present study is to analyze, in a group of patients with MS, the relationship between IPS and clinical variables such as disability, disease evolution, fatigue and depression, as well as its relationship with the social support perceived by the patients.
METHODS
Participants
A group of 47 patients diagnosed with Relapsing-Remitting Multiple Sclerosis (RRMS) were evaluated—of which 31 were women and 16, men—, who had been treated at the Unit of Demyelinating Diseases of the General Hospital of Acute Diseases J. M. Ramos Mejía, Buenos Aires City. Participants were selected based on an incidental, non-probability sampling strategy. The patients who had attended neurological consultation and met inclusion and exclusion criteria were asked to participate in the study. They all signed an informed consent. Both the study and the informed consent were approved by the Ethics Committee of the institution (approval date: November 1, 2017).
As inclusion criteria, the following were established: being more than 18-years-old, having a diagnose of RRMS as per Poser et al.34 and Mcdonald criteria,35 having a minimum of seven years of schooling, and being able to understand and respond to the entire procedure. As exclusion criteria: having psychiatric disorders, severe visual or auditory deficits—or any other physical impairment that would not permit patients to appropriately carry out the test—, a medical history of events that affect cognition or personality, a history of alcoholism or drug abuse, systemic diseases that may produce cognitive impairment, or having had relapses or corticoids administration four weeks previous to the study.
Instruments of measure
Measures of IPS
In the PASAT, patients are asked to listen an audio in wich 61 successive numbers were presented at a fixed rate and they should orally provide the sums of consecutive numbers as rapidly as possible. Originally, the time interval between the stimuli was 2.4 s, 2.0 s, 1.6 s, 1.2 s, and 0.8 s.11 However, in MS research and clinical practice, the 3-s (PASAT-3) and 2-s (PASAT-2) versions of the interstimulus interval have been implemented.13 For this research we implemented the 3 seconds version which is internationally used in most MS studies. Higher scores on the PASAT represent better IPS.
In the SDMT, the subject is presented a form headed by a key that pairs single digits (1 to 9) to nine different symbols. The rows that are below contain only the symbols. The subject's task is to record both orally and in writing the correct number in the adjacent empty spaces. After completing the first ten items with guidance, the subject is then timed to observe how many responses they can fulfill in 90 seconds. In the standard administration of the SDMT, the written response task is conducted first, followed by an oral response task using the same stimuli. However, the majority of studies on MS skip the written response administration and only utilize the oral version.15 Thus, the examiner uses a form in which they record the subject's voiced responses in such a manner that the scoring can be made quickly, with minimal chance for error. In total, the test requires five minutes to complete. Since the subjects participating in this study were MS patients, the oral version of the SDMT was used. Higher scores on the SDMT represent better IPS.
Social support
In order to evaluate this aspect, the Medical Outcomes Study Social Support Survey (MOS) Social Support Survey was used,40 adapted to Argentina by Rodríguez and Enrique.41 It is a brief multidimensional survey that allows to evaluate aspects both quantitative (social network) and qualitative (dimensions of social support). It consists of 20 items: the first refers to the size of the social network (number of friends and family members on whom the patient can rely) and the other 19 to the dimensions of social support. These dimensions are: emotional/informational support—which represents the information that can be used by the patient to anticipate and react to problems, in the form of suggestions and advice—; affective support—real demonstrations of love, affection or empathy—; instrumental support—the access to material resources such as economic help, food and clothing—.29 The higher the score in the MOS, the better social support.
Statistical analysis
The data were analyzed through the SPSS statistical package version 21.0 (IBM Corp., Armonk, NY, USA). The degree of significance used was p<0.05. Descriptive statistics for the patients' demographic and clinical variables were obtained. Pearson correlation coefficient was implemented in order to study the relationship between IPS, clinical variables and the social support perceived by the patients. A simple linear regression analysis was conducted in order to assess the impact of processing speed (independent variable) on each one of the clinical variables (dependent variables). In order to identify to what extent processing speed can predict social support, a stepwise regression was conducted. Scores from EDSS, BDI-II, and FSS were added in each regression analysis (block 1) to control the influence that motor disability, depression and fatigue have in estimating the relationship between processing speed (block 2) and each score of social support (dependent variable).
RESULTS
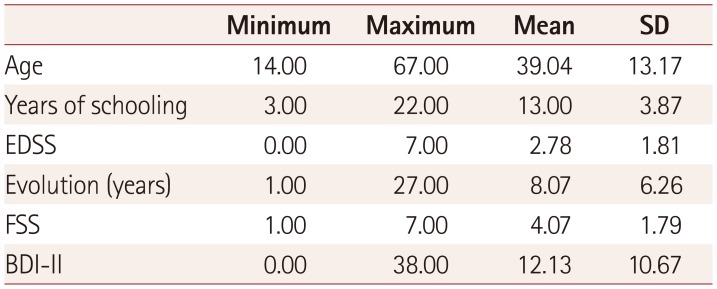
The group of patients was composed of 31 women (66% of the total) and 16 men (34%). The mean for age was 39.04± 13.17 years-old, and for years of schooling, 13.00±3.87. Patients had an EDSS mean of 2.78±1.81, and the mean for years of disease evolution was 8.07±6.26 years. BDI-II mean was 12.13±10.67, and FSS mean was 4.07±1.79, representing mild levels of depression and fatigue as reported by patients. Results are shown in Table 1.
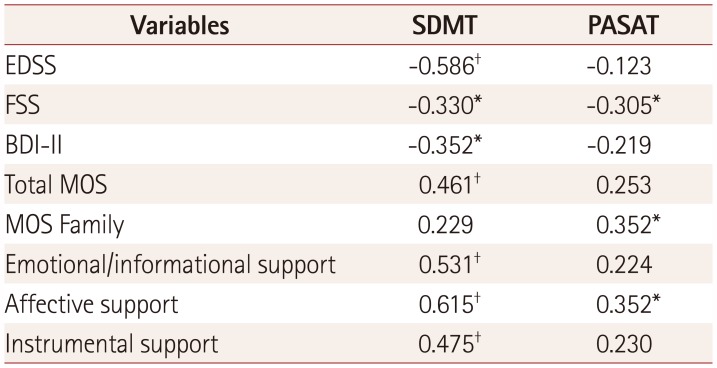
Significant associations were found between IPS and most of the clinical variables, as can be observed in Table 2. The scores that the patients obtained in the SDMT correlated significantly and negatively with measures of motor disability, fatigue and depression, whereas the scores obtained in the PASAT correlated significantly and negatively with measures of fatigue. No associations were found between IPS and the years of disease evolution.
Regarding social support, significant and positive associations were found between IPS and the scores obtained by the patients in the social support survey. The SDMT correlated with the total score of the survey, as well as with its three dimensions—emotional/informational, affective and instrumental—,while the PASAT correlated significantly with the dimension of emotional support and with the number of family members whom patients can rely on as their network of support.
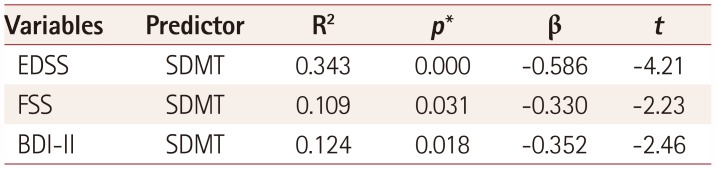
In order to analyze the influence of IPS on the clinical variables under evaluation, the scores obtained by the patients in the SDMT and PASAT were added as independent variables in a linear regression model, as performance predictors in EDSS, FSS, and BDI-II. The result was a model that explains to a large extent the variance in the clinical variables.
The regression model implemented with the SDMT explains 34.3% of the variance in EDSS (p=0.000), as well as 10.9% of the variance in FSS (p=0.031), and 12.4% in BDI-II (p=0.018). Processing speed, measured through the SDMT, appeared as the performance predictor of the mentioned variables, demonstrating a significant relationship between processing speed and EDSS, FSS, and BDI-II. The model implemented with the PASAT was not significant (Table 3).
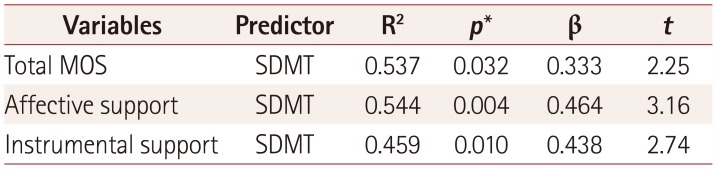
Regarding social support, when the variables of EDSS, FSS, and BDI-II were controlled, SDMT produced a model that explains 53.7% of the variance of the MOS total score (p=0.032), 54.4% of affective support (p=0.004), and 45.9% of instrumental support (p=0.010). The PASAT was not a significant predictor after the clinical variables were controlled (Table 4).
DISCUSSION
Changes in IPS are frequent symptoms of MS that can interfere in different aspects of the patients' life. The study of these variables is relevant for the treatment MS patients. The aim of this study is to describe the relationship between IPS and clinical variables such as motor disability, disease evolution, fatigue and depression, as well as its relationship with the social support perceived by patients with MS.
The results obtained confirm that IPS is a cognitive function that highly predicts clinical aspects and the social support of patients with MS. Patients with a greater degree of motor disability, depression, fatigue, and with a weaker network of social support, also had slow processing speed. On the other hand, in this study no associations were found between processing speed and the years of disease evolution. These findings are consistent with the previously reported by Sundgren et al.,23 who found that IPS was the cognitive function most strongly associated with motor disability. Other authors do not report such association.26 Regarding disease evolution, previous studies coincide with our results in that there is no correlation between processing speed and the years of disease evolution.2442 However, Dusankova et al.22 found that patients who had more years of disease evolution performed worse in IPS tasks; but in that case, patients had different disease' subtypes, which might explain those results. Meanwhile, the results obtained concerning fatigue severity are consistent with previous studies that show that there is a relationship between IPS and fatigue in patients with MS.20232527 Jougleux-Vie et al.28 dismiss that relationship, but they measured fatigue with a different instrument than ours. In this study, we also found a strong influence of IPS on the patients' degree of depression, a relationship that has been previously described.18192327
An interesting finding is the relationship between processing speed and the network of social support, both in the quantitative and qualitative aspects. When the influence of speed on social support was analyzed, it was found that patients with slow IPS had weaker social relations in terms of quality. Patients who were experiencing a slowdown receive fewer demonstrations of affection and have less help of material resources, than those who are not in that stage. There are previous studies that report variations in the social support perceived by patients with MS,2143 but its relationship with cognition—and specifically, with IPS—has not been studied. Our findings are consistent with those of Glanz et al.,21 who found that there is a strong correlation between the SDMT and one dimension of social support, although they used a different method of measure than ours. Barker-Collo33 describes that there is a strong relationship between IPS and the social relations of patients with MS, and although in that case the network of social support was not specifically evaluated, the patients who had a slow IPS ranked lower in the items related to social relations of a quality of life scale.
The reported findings reaffirm the importance of considering the processing speed in the different aspects of MS patients, and specifically consider the variable of social support, which has not been especially highlighted in previous studies about quality of life in MS patients. This last finding is highly relevant because an adequate social support is really necessary in patients suffering from this kind of diseases, and it would be especially affected in patients with slow processing. Even though there are treatments of cognitive stimulation44 and physical activity45 that collaborate with the rehabilitation of different cognitive functions, including the speed of processing, studying in more detail the processing speed could help the development of specific training programs that are really necessary.
It is essential to aim towards the need of taking into consideration IPS when treating patients with MS, since it has an important influence on the clinical aspects and the social network of the patients. As it mentioned above, the last point has special importance, given the prominence of social relations in the therapeutic treatment and rehabilitation process of chronic diseases, as well as in the patients' quality of life.
 XML Download
XML Download