

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
METHODS
RESULTS
Case report
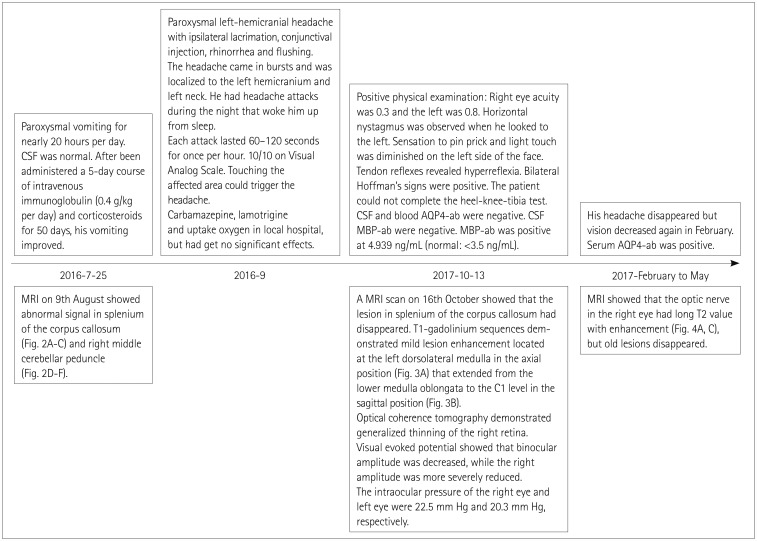 | Fig. 1Medical history. AQP4-ab: aquaporin-4 antibody, CSF: cerebrospinal fluid, MBP-ab: myelin basic protein antibody, MRI: magnetic resonance imaging.
|
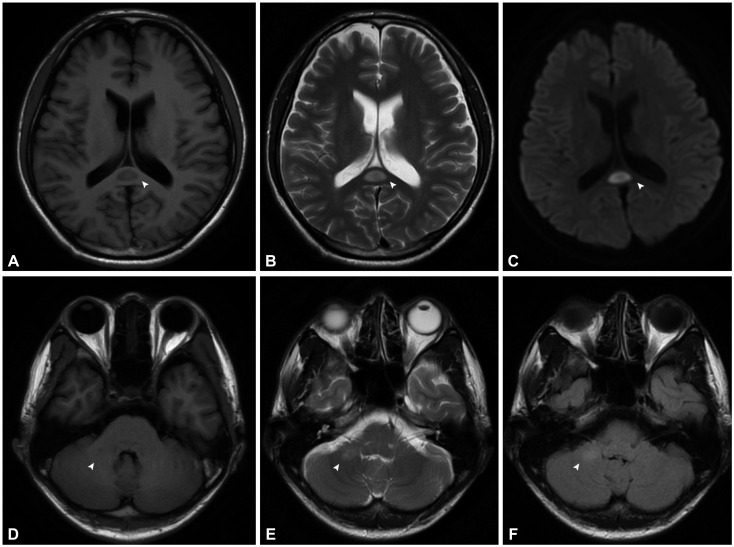 | Fig. 2MRI performed on August 9 showed slightly long T1-weighted (A), and T2-weighted (B) values for the splenium of the corpus callosum (arrowheads) with a high diffusion-weighted-imaging signal (C), and equal T1 signal (D), slightly high T2 (E), and T2 Flair values (F) for the right middle cerebellar peduncle (arrowheads).
|
Literature review
Table 1
Clinical features of 17 patients with short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing attributed to neoplasm
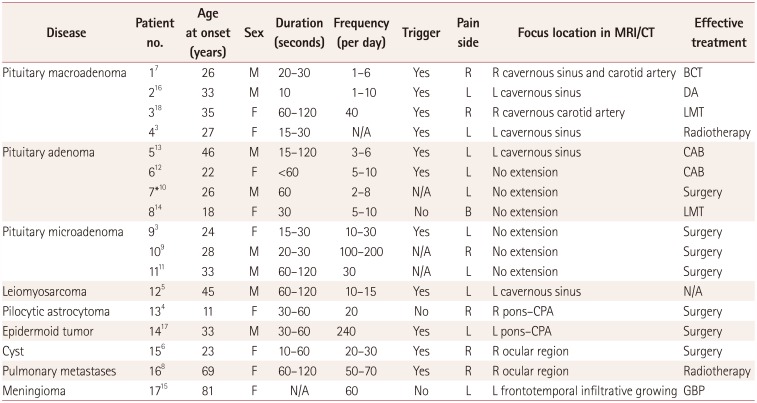
| Disease | Patient no. | Age at onset (years) | Sex | Duration (seconds) | Frequency (per day) | Trigger | Pain side | Focus location in MRI/CT | Effective treatment |
|---|---|---|---|---|---|---|---|---|---|
| Pituitary macroadenoma | 17 | 26 | M | 20–30 | 1–6 | Yes | R | R cavernous sinus and carotid artery | BCT |
| 216 | 33 | M | 10 | 1–10 | Yes | L | L cavernous sinus | DA | |
| 318 | 35 | F | 60–120 | 40 | Yes | R | R cavernous carotid artery | LMT | |
| 43 | 27 | F | 15–30 | N/A | Yes | L | L cavernous sinus | Radiotherapy | |
| Pituitary adenoma | 513 | 46 | M | 15–120 | 3–6 | Yes | L | L cavernous sinus | CAB |
| 612 | 22 | F | <60 | 5–10 | Yes | L | No extension | CAB | |
| 7*10 | 26 | M | 60 | 2–8 | N/A | L | No extension | Surgery | |
| 814 | 18 | F | 30 | 5–10 | No | B | No extension | LMT | |
| Pituitary microadenoma | 93 | 24 | F | 15–30 | 10–30 | Yes | L | No extension | Surgery |
| 109 | 28 | M | 20–30 | 100–200 | N/A | R | No extension | Surgery | |
| 1111 | 33 | M | 60–120 | 30 | N/A | L | No extension | Surgery | |
| Leiomyosarcoma | 125 | 45 | M | 60–120 | 10–15 | Yes | L | L cavernous sinus | N/A |
| Pilocytic astrocytoma | 134 | 11 | F | 30–60 | 20 | No | R | R pons–CPA | Surgery |
| Epidermoid tumor | 1417 | 33 | M | 30–60 | 240 | Yes | L | L pons–CPA | Surgery |
| Cyst | 156 | 23 | F | 10–60 | 20–30 | Yes | R | R ocular region | Surgery |
| Pulmonary metastases | 168 | 69 | F | 60–120 | 50–70 | Yes | R | R ocular region | Radiotherapy |
| Meningioma | 1715 | 81 | F | N/A | 60 | No | L | L frontotemporal infiltrative growing | GBP |
![]()
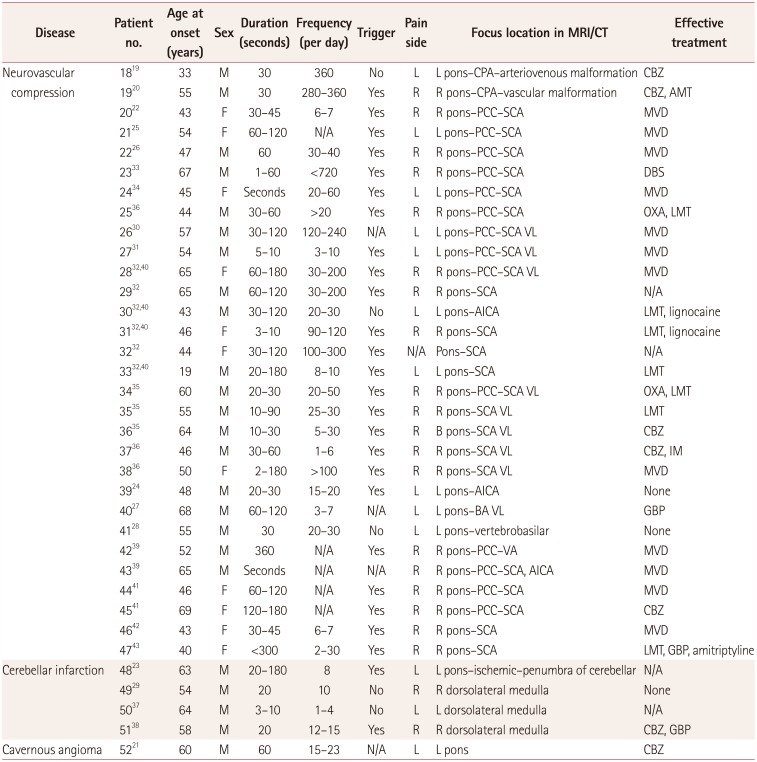
Table 2
Clinical features of 35 patients with short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing attributed to vascular disease
| Disease | Patient no. | Age at onset (years) | Sex | Duration (seconds) | Frequency (per day) | Trigger | Pain side | Focus location in MRI/CT | Effective treatment |
|---|---|---|---|---|---|---|---|---|---|
| Neurovascular compression | 1819 | 33 | M | 30 | 360 | No | L | L pons–CPA–arteriovenous malformation | CBZ |
| 1920 | 55 | M | 30 | 280–360 | Yes | R | R pons–CPA–vascular malformation | CBZ, AMT | |
| 2022 | 43 | F | 30–45 | 6–7 | Yes | R | R pons–PCC–SCA | MVD | |
| 2125 | 54 | F | 60–120 | N/A | Yes | L | L pons–PCC–SCA | MVD | |
| 2226 | 47 | M | 60 | 30–40 | Yes | R | R pons–PCC–SCA | MVD | |
| 2333 | 67 | M | 1–60 | <720 | Yes | R | R pons–PCC–SCA | DBS | |
| 2434 | 45 | F | Seconds | 20–60 | Yes | L | L pons–PCC–SCA | MVD | |
| 2536 | 44 | M | 30–60 | >20 | Yes | R | R pons–PCC–SCA | OXA, LMT | |
| 2630 | 57 | M | 30–120 | 120–240 | N/A | L | L pons–PCC–SCA VL | MVD | |
| 2731 | 54 | M | 5–10 | 3–10 | Yes | L | L pons–PCC–SCA VL | MVD | |
| 2832,40 | 65 | F | 60–180 | 30–200 | Yes | R | R pons–PCC–SCA VL | MVD | |
| 2932 | 65 | M | 60–120 | 30–200 | Yes | R | R pons–SCA | N/A | |
| 3032,40 | 43 | M | 30–120 | 20–30 | No | L | L pons–AICA | LMT, lignocaine | |
| 3132,40 | 46 | F | 3–10 | 90–120 | Yes | R | R pons–SCA | LMT, lignocaine | |
| 3232 | 44 | F | 30–120 | 100–300 | Yes | N/A | Pons–SCA | N/A | |
| 3332,40 | 19 | M | 20–180 | 8–10 | Yes | L | L pons–SCA | LMT | |
| 3435 | 60 | M | 20–30 | 20–50 | Yes | R | R pons–PCC–SCA VL | OXA, LMT | |
| 3535 | 55 | M | 10–90 | 25–30 | Yes | R | R pons–SCA VL | LMT | |
| 3635 | 64 | M | 10–30 | 5–30 | Yes | R | B pons–SCA VL | CBZ | |
| 3736 | 46 | M | 30–60 | 1–6 | Yes | R | R pons–SCA VL | CBZ, IM | |
| 3836 | 50 | F | 2–180 | >100 | Yes | R | R pons–SCA VL | MVD | |
| 3924 | 48 | M | 20–30 | 15–20 | Yes | L | L pons–AICA | None | |
| 4027 | 68 | M | 60–120 | 3–7 | N/A | L | L pons–BA VL | GBP | |
| 4128 | 55 | M | 30 | 20–30 | No | L | L pons–vertebrobasilar | None | |
| 4239 | 52 | M | 360 | N/A | Yes | R | R pons–PCC–VA | MVD | |
| 4339 | 65 | M | Seconds | N/A | N/A | R | R pons–PCC–SCA, AICA | MVD | |
| 4441 | 46 | F | 60–120 | N/A | Yes | R | R pons–PCC–SCA | MVD | |
| 4541 | 69 | F | 120–180 | N/A | Yes | R | R pons–PCC–SCA | CBZ | |
| 4642 | 43 | F | 30–45 | 6–7 | Yes | R | R pons–SCA | MVD | |
| 4743 | 40 | F | <300 | 2–30 | Yes | R | R pons–SCA | LMT, GBP, amitriptyline | |
| Cerebellar infarction | 4823 | 63 | M | 20–180 | 8 | Yes | L | L pons–ischemic–penumbra of cerebellar | N/A |
| 4929 | 54 | M | 20 | 10 | No | R | R dorsolateral medulla | None | |
| 5037 | 64 | M | 3–10 | 1–4 | No | L | L dorsolateral medulla | N/A | |
| 5138 | 58 | M | 20 | 12–15 | Yes | R | R dorsolateral medulla | CBZ, GBP | |
| Cavernous angioma | 5221 | 60 | M | 60 | 15–23 | N/A | L | L pons | CBZ |
AICA: anterior inferior cerebellar artery, AMT: amitriptyline, BA: basilar artery, CBZ: carbamazepine, CPA: cerebellopontine angle, CT: computed tomography, DBS: deep brain stimulation, GBP: gabapentin, IM: indomethacin, LMT: lamotrigine, MRI: magnetic resonance imaging, MVD: microvascular decompression, N/A: not applicable, OXA: oxcarbazepine, PCC: pontocerebellar cistern, SCA: superior cerebellar artery, VA: vertebral artery, VL: vascular loop.
![]()
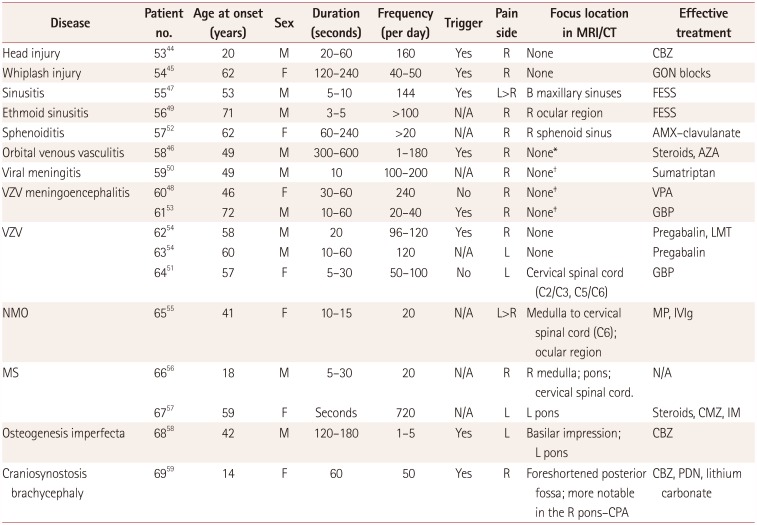
Table 3
Clinical features of 17 patients with short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing attributed to other etiologies
| Disease | Patient no. | Age at onset (years) | Sex | Duration (seconds) | Frequency (per day) | Trigger | Pain side | Focus location in MRI/CT | Effective treatment |
|---|---|---|---|---|---|---|---|---|---|
| Head injury | 5344 | 20 | M | 20–60 | 160 | Yes | R | None | CBZ |
| Whiplash injury | 5445 | 62 | F | 120–240 | 40–50 | Yes | R | None | GON blocks |
| Sinusitis | 5547 | 53 | M | 5–10 | 144 | Yes | L>R | B maxillary sinuses | FESS |
| Ethmoid sinusitis | 5649 | 71 | M | 3–5 | >100 | N/A | R | R ocular region | FESS |
| Sphenoiditis | 5752 | 62 | F | 60–240 | >20 | N/A | R | R sphenoid sinus | AMX–clavulanate |
| Orbital venous vasculitis | 5846 | 49 | M | 300–600 | 1–180 | Yes | R | None* | Steroids, AZA |
| Viral meningitis | 5950 | 49 | M | 10 | 100–200 | N/A | R | None† | Sumatriptan |
| VZV meningoencephalitis | 6048 | 46 | F | 30–60 | 240 | No | R | None‡ | VPA |
| 6153 | 72 | M | 10–60 | 20–40 | Yes | R | None‡ | GBP | |
| VZV | 6254 | 58 | M | 20 | 96–120 | Yes | R | None | Pregabalin, LMT |
| 6354 | 60 | M | 10–60 | 120 | N/A | L | None | Pregabalin | |
| 6451 | 57 | F | 5–30 | 50–100 | No | L | Cervical spinal cord (C2/C3, C5/C6) | GBP | |
| NMO | 6555 | 41 | F | 10–15 | 20 | N/A | L>R | Medulla to cervical spinal cord (C6); ocular region | MP, IVIg |
| MS | 6656 | 18 | M | 5–30 | 20 | N/A | R | R medulla; pons; cervical spinal cord. | N/A |
| 6757 | 59 | F | Seconds | 720 | N/A | L | L pons | Steroids, CMZ, IM | |
| Osteogenesis imperfecta | 6858 | 42 | M | 120–180 | 1–5 | Yes | L | Basilar impression; L pons | CBZ |
| Craniosynostosis brachycephaly | 6959 | 14 | F | 60 | 50 | Yes | R | Foreshortened posterior fossa; more notable in the R pons–CPA | CBZ, PDN, lithium carbonate |
*Narrowing of superior ophthalmic vein, †Thermogram showed that the skin temperature was higher around the orbital region than around the left side, suggesting decreased right sympathetic nerve function, ‡CT scans were normal when headache started. The author considered them to be a peripheral mechanism.
AMX: amoxicillin, AZA: azathioprine, CBZ: carbamazepine, CMZ: carbimazole, CPA: cerebellopontine angle, CT: computed tomography, FESS: functional endoscopic sinus surgery, GBP: gabapentin, GON: greater occipital nerve, IM: indomethacin, IVIg: intravenous immunoglobulin, MP: methylprednisolone, MRI: magnetic resonance, MS: multiple sclerosis, N/A: not applicable, NMO: neuromyelitis optica, PDN: prednisone, VPA: valproic acid, VZV: varicella-zoster virus.
![]()
SUNCT secondary to neoplasm
SUNCT secondary to neurovascular disease
SUNCT secondary to other etiologies
Focus location
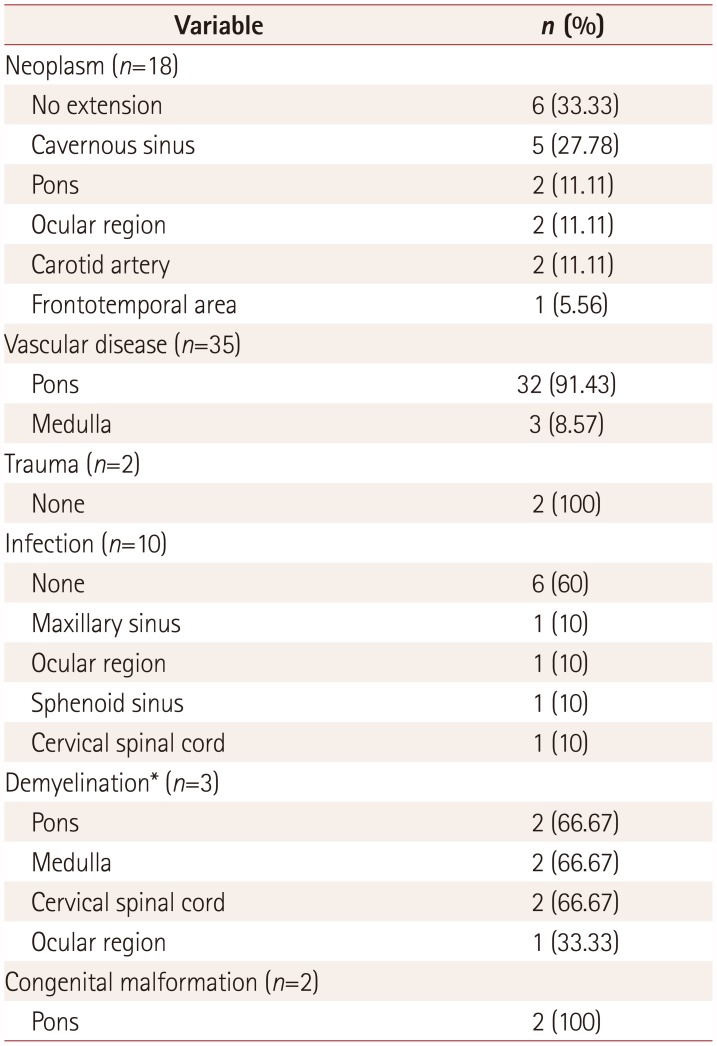
Table 4
Distribution of lesion locations according to the etiology classification
![]()
Table 5
Distribution of etiology according to the classification of lesion location
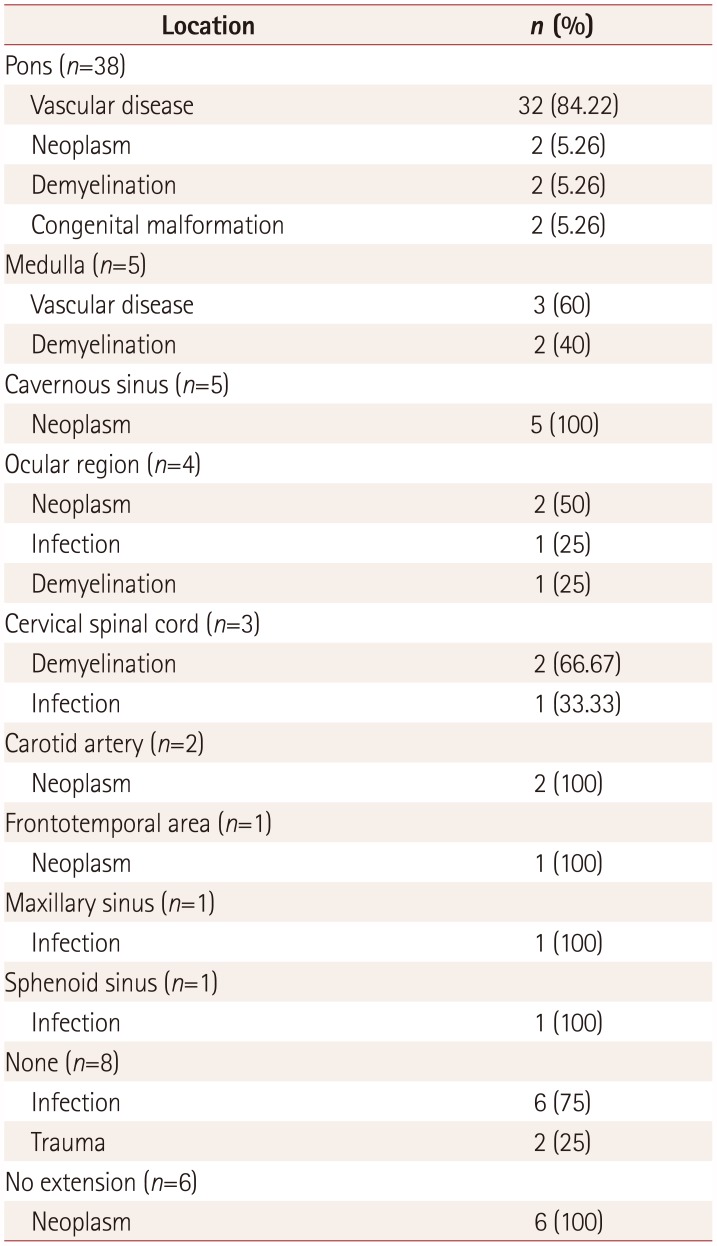
![]()
DISCUSSION
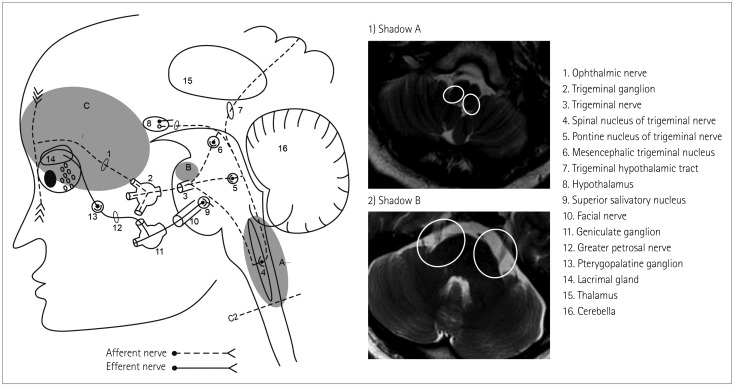 | Fig. 5Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing-related pathways and structures. Shadow A represents the dorsolateral medulla and upper cervical spinal cord where the spinal nucleus of the trigeminal nerve was located, which was often affected by cerebral infarction and demyelination. Vascular compression was likely to occur in the area of Shadow B. The neoplasm and infection had a widespread focus, and were mostly located at the preganglionic fibers of the trigeminal nerve (Shadow C).
|
 XML Download
XML Download