

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Shoulder subluxation, one possible reason of hemiplegic shoulder pain (HSP), refers to a non-traumatic, partial or total change of relation between the scapula and the humerus in all directions and planes as compared to the non-affected shoulder [1]. Shoulder subluxation in hemiplegic patients after stroke varies commonly in 17% to 64% [2]. The development of shoulder subluxation occurs mostly during the first 3 weeks of hemiplegia [3].
HSP is a general term used to describe pain in the paralyzed shoulder in stroke patients. HSP impacts on upper limb functional recovery, activities of daily living performance, and quality of life and is associated with a higher incidence of depression both during and after rehabilitation [4]. In a hemiplegic shoulder, the humeral head is displaced inferiorly and anteriorly by a loss of normal shoulder muscle activity, particularly the supraspinatus and posterior deltoid muscles, and the weight of the upper limb stretches the joint capsule, muscles, tendons, and ligaments which in turn leads to painful ischemia in the peri-articular tissues of shoulder joint [5]. Latent shoulder pain after shoulder subluxation occurs due to fibrous changes or injury in these peri-articular tissues due to the improper alignment between the humerus and scapula. However, the relationship between the subluxation and HSP is controversial so far.
Various interventions for subluxation includes positioning, slings, strapping and electrical stimulation [16]. Among these treatments, strapping and slings have the shortcomings of holding the upper extremity in a bad position that seems to cause peri-articular tissue contracture and have a disadvantageous effect on body image, balance, and symmetry. One purpose of sling is to prevent HSP from shoulder subluxation, but sling can result in rather deteriorating HSP.
A recent and relatively large study reported that HSP was significantly more frequent in subjects with shoulder subluxation [7]. As in previous studies, simple radiography is not able to reveal a correlation between the subluxation and HSP. Compared with simple radiography, magnetic resonance (MR) arthrography may clarify the relationship between soft-tissue injuries and HSP. Therefore, we hypothesized that there were more abnormal findings on MR arthrography in patients with HSP than those without HSP. In the current study, we intended to group hemiplegic patients with shoulder subluxation according to the presence of HSP and to compare the difference in clinical and MR arthrography findings between groups in the effort to find factors possibly related to HSP, with the eventual aim of evaluating and managing HSP properly in hemiplegic patients with shoulder subluxation.
MATERIALS AND METHODS
Setting and participants
After approval from the Institutional Review Board (approval number: 4-2015-0327), we reviewed medical records of stroke survivors who admitted to a university rehabilitation institute for the rehabilitation of the sequelae of an ischemic or hemorrhagic stroke between March 2013 and February 2015 retrospectively to identify all eligible patients.
Inclusion criteria included 1) stroke occurring ≤ 3 months before MR arthrography evaluation; 2) hemiplegia; 3) shoulder subluxation; 4) MR arthrography and all clinical evaluation conducted within 7 days; and 5) > 24 on the Mini-Mental Status Examination scale for pain assessment [8]. Shoulder subluxation was diagnosed when there was a gap of more than one fingerbreadth between the acromion and the head of the humeral bone by palpation [9]. In addition, we confirmed all shoulder subluxation by anteroposterior radiographs centered on the glenohumeral joint. During the shoulder X-ray examination, patients were instructed to sit with an upright posture with the arm in a neutral position hanging down under gravity. Exclusion criteria included 1) prestroke shoulder pain; 2) previous stroke; 3) analgesics and muscle relaxants from 7 days before MR and clinical evaluation; 4) botulinum toxin at any time before MR and clinical evaluation; 5) hemineglect; 6) complex regional pain syndrome; 7) cervical originated pain; 8) central and/or other neuropathic pain; and 9) intensive trauma of the shoulder.
Data collection
Collected specific characteristics included age, gender, time from stroke onset to MR arthrography evaluation, duration of poststroke shoulder pain, stroke type (hemorrhagic versus ischemic), side of hemiplegia, and severity of HSP rated with a 10-cm horizontal visual analog scale (VAS). VAS score 0 was defined as no pain, 1 to 3 as mild pain, and 4 to 10 as moderate–severe pain [10]. Finding of physical examination also were collected. Motor status was documented based on the medical research council scale. Passive range of motions (ROM) of shoulder was measured using a goniometer with the patient sitting on a stool. Abduction, forward flexion and external rotation were measured. Muscle spasticity was measured by the modified Ashworth scale (MAS; range 0–5, with 0 representing no spasticity and 5 representing extreme spasticity) [11]. Subjects were divided into 2 groups according to presence of HSP. HSP was diagnosed in patients with a VAS value ≥ 4 [12].
MR arthrography assessment
All patients underwent shoulder MR arthrography. All MR examinations were performed on 3.0-T scanners (Horizon, GE Healthcare, Milwaukee, WI, USA; or Gyroscan Intera, Philips Healthcare, Bothell, WA, USA; or Magnetom Trio, Siemens, Elrangen, Germany) with an 8-channel shoulder coil (Invivo, Gainesville, FL, USA). Patients received an intra-articular injection of 15–18 mL of diluted dimeglumine gadopentetate solution with a concentration of 0.08 mL of Magnevist (Schering, Berlin, Germany) per 18 mL of normal saline and 2 mL of iodine contrast into the glenohumeral joint performed under fluoroscopic guidance before MR arthroscopy. The following scanning sequences were performed: axial, sagittal, and coronal fat-suppressed T1-weighted spin-echo sequences. All MR arthroscopy images were interpreted or confirmed by one radiologist with more than 8 years of experience in musculoskeletal MR. The following requirements were requested when prescribing MR arthrography such as frozen shoulder including inferior recess thickening; rotator cuff interval measurements; rotator cuff injury (including biceps longhead tendon); and presence/absence of subdeltoid-subacromial bursitis.
Statistical analyses
SPSS version 21.0 (SPSS Inc., Chicago, IL, USA) was used for all statistical analyses. Patients whose VAS scores with a clinically meaningful amount (≥ 4 points) were classified as HSP group, whereas patients who did not were classified as no-HSP group. Independent t-test and χ2 test were used to compare differences between the 2 groups. In addition, logistic regression analyses were used to identify the relating factors for HSP. HSP group was coded as 1, and the no-HSP group was coded as 0. The significant relating factors with a significance level of p < 0.20, identified by univariate logistic analyses, were entered into the forward multivariate logistic regression models. A p value < 0.05 was considered to be statistically significant.
Additional analysis was done to evaluate whether ROM and spasticity of the shoulder were correlated irrespective of findings of adhesive capsulitis in MR arthrography. Since ROM and spasticity of the shoulder did not show normal distribution respectively, Spearman correlation coefficients were calculated to investigate the association between them.
RESULTS
A total of 726 stroke patients were admitted to the university rehabilitation institute and assessed for study eligibility between March 2013 and February 2015. Of these, 59 patients (mean age 65.0 ± 11.0 years); mean body weight 65.4 ± 14.1 kg; mean body height 162.6 ± 8.4 cm; 56% male; 74% ischemic stroke) were eligible for the criteria. The flowchart of the study is presented in Fig. 1.

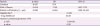
Twenty-one (35.6%) and 38 (64.4%) patients were classified as the HSP and no-HSP groups, respectively (Table 1). Table 2 reports the results of univariate logistic regression on the HSP group.
Table 1
Comparison of the pain and the no-pain groups

HSP, hemiplegic shoulder pain; MR, magnetic resonance; VAS, visual analog scale; ROM, range of motion; MRC, medical research council scale.
*Compared with HSP group.
![]()
Table 2
Univariate logistic regression analysis to identify relating factors associated with the hemiplegic shoulder pain

OR, odds ratio; CI, confidence interval; ROM, range of motion; MRC, medical research council scale; MAS, modified Ashworth scale; MR, magnetic resonance.
![]()
The results from multivariate logistic regression analysis are summarized in Table 3. Of particular note, ROM of flexion and rotator cuff atrophy were significantly related to HSP in stroke patients (Nagelkerke R2 = 0.449, p < 0.05).
Table 3
Multivariate logistic regression analysis to identify relating factors associated with the hemiplegic shoulder pain
![]()
The final logistic regression equation showed that ROM of flexion was 1.1 times more likely associated with HSP in patients with stroke. Similarly, HSP in the stroke patients with the rotator cuff atrophy apparent in MR arthrography was 6.4 times more likely than in those without the rotator cuff atrophy in MR arthrography. However, the ROM of abduction, external rotation, and total ROM of shoulder were not significantly related with HSP. Muscle power and spasticity were also not related with HSP. Of MR arthrography findings, those compatible with adhesive capsulitis were not significantly related with HSP. Findings compatible with adhesive capsulitis included axillary recess thickening, rotator cuff interval obliteration, and coracohumeral ligament thickening. Rotator cuff tear, biceps lesion, acromioclavicle joint arthrosis, and humerus chondromalacia were also not significantly correlated with HSP.
From additional analysis, MAS of flexion correlated with ROM in flexion (coefficient = 0.257, p = 0.049), external rotation (coefficient = 0.276, p = 0.034), and total ROM (coefficient=0.278, p = 0.033).
DISCUSSION
The purpose of this study was to group hemiplegic patients with shoulder subluxation according to the presence of HSP and to compare the difference in clinical and MR arthrography findings between 2 groups in the effort to find factors possibly related to HSP. To our knowledge, this is the first study to evaluate MR arthrography findings in hemiplegic shoulders with subluxation. A significant correlation between HSP and restricted ROM of the shoulder was evident. An unexpected finding was that HSP did not relate with MR arthrography findings, except for rotator cuff muscle atrophy.
Previous studies of MR findings suggestive of adhesive capsulitis between stoke survivors with and without HSP reported that synovial capsule thickening, synovial capsule enhancement, and enhancement in the rotator cuff interval were more prominent in those with HSP [1314]. Unlike these studies, our study conducting on shoulder subluxation found no more MR arthrography findings suggesting adhesive capsulitis in the HSP group. Although many stroke survivors suffer from restricted ROM, it is not fully established whether the pathologic biomechanics are same with adhesive capsulitis. Another potential reason of restricted ROM in hemiplegic shoulder, besides the adhesive capsulitis-like process, might be spasticity around the shoulder joint. It was reported that hemiplegic shoulder had less stiff glenohumeral joint capsules than those with adhesive capsulitis, who had similar ROM limitations [15]. In this context, restricted ROM of the hemiplegic shoulder could result from the combination of adhesive capsulitis and spasticity rather than a pure adhesive capsulitis since spasticity were correlated with restricted ROM of the shoulder in the current study. Therefore, prevention and aggressive management of spasticity and contracture in hemiplegic patients with shoulder subluxation are needed to reduce HSP.
Arm slings have been used for shoulder subluxation. Slings might be theoretically useful while patients ambulate to support the dependent extremity against the effects of gravity and prevent further subluxation and/or decrease pain. A 2009 Cochrane review, however, found insufficient evidence to determine whether slings prevent subluxation, decrease pain, or increase function after stroke [16]. Furthermore, in case of hemislings, positioning of the arm in adduction and internal rotation can predispose these patients to adhesive capsulitis and can promote contractures as the arm is kept in a flexor synergy pattern [17]. If the arm is incorrectly positioned, or if use of a sling is not alternated with therapeutic exercise, soft-tissue contractures can occur. Such contractures can contribute to the very pain the sling is intended to prevent. Since HSP in patients with shoulder subluxation are directly affected by restricted ROM of the shoulder, more active ROM exercise of the shoulder is required regardless of applying slings. Also, the present findings suggest that pathologic lesions like rotator cuff tear may not be related with HSP in patients with shoulder subluxation. Further studies are needed.
Previous studies demonstrated increased prevalence of the rotator cuff tear in hemiplegia [181920], contrary to other reports that suggested no association between them [212223]. Occurrence of rotator cuff tear in hemiplegia depends on the severity of motor weakness [24]. A subluxed shoulder can have altered biomechanics and may predispose the patients to rotator cuff injury. Although this study was not designed to assess the prevalence of rotator cuff tear in patients of HSP with shoulder subluxation, this study results showed that there was no difference in the incidence of rotator cuff lesion including the long head of biceps brachii between the HSP and non-HSP groups. The results correspond with a previous study reporting that the association of rotator cuff tears in hemiplegia with premorbid shoulder pain and not with HSP [24]. It may not be necessary to diagnose rotator cuff tear in hemiplegic shoulder if rotator cuff tear does not cause any symptom such as HSP.
The current study showed that HSP did not relate with MR arthrography findings, except for rotator cuff muscle atrophy. We do not know that rotator cuff muscle atrophy was the cause or result of HSP. However, atrophic rotator cuff muscle can result in pain with a pulling sensation with movement, which contributes to posture and muscle imbalance [25]. Considering that muscle imbalance, postural disturbance, and immobilization-common findings in poststroke patients are predisposing factors for the appearance of myofascial trigger points [26], myofascial pain can be a potential contributing cause of HSP. Further studies are needed.
There are some limitations in our study. The retrospective, cross-sectional design study cannot reveal a causal relationship between HSP and other factors. Second, we may have missed potential confounders. Specifically, we excluded the patients who have central pain, central sensitization, and complex regional pain syndrome since they can also play an important role in HSP development. Third, there was a selection bias in the study sample since not all subluxed shoulders were examined by MR arthrography. Because the included subjects did not represent a random sampling of all stroke survivors with subluxed shoulder, the study results may not be generalizable to the broader stroke population. Finally, when the patients were divided into 2 groups, it can be the limitation of this study to set the diagnostic criteria for HSP to “VAS 4 above or below.”
In conclusion, there is a significant correlation between HSP and restricted ROM of shoulder subluxation in this study. Therefore, active treatment of restricted ROM in subluxed shoulder should be emphasized since restricted ROM of shoulder itself is associated with HSP in these patients.
Also, HSP did not relate with MR arthrography findings, except rotator cuff muscle atrophy in hemiplegic patients with shoulder subluxation. In this study, it is difficult to know why the presence or absence of restricted ROM or rotator cuff atrophy affects HSP, and we will try to clarify this through prospective studies on a large number of patients.
 XML Download
XML Download