

 PDF
PDF Citation
Citation Print
Print



INTRODUCTION
Accepted treatment of acute ischemic stroke until now are reperfusion therapy with tissue plasminogen activator or intra-arterial thrombolysis or mechanical thrombectomy. But due to limited time window, still majority of patient cannot benefit from these treatments and even after all the successful standard therapy, neurological deficit still remains. Therefore, strategies for protecting neurons must continue from the beginning to the end of the treatment. From this point of view, pleiotropic functioning material can be expected to be more effective [1]. Insulin-like growth factor-1 (IGF-1) is appropriate candidate because it has pleiotropic effects such as neurogenesis [2], increasing muscle mass [3] and involved in ocular growth by influencing the synthesis of the extracellular matrix of the sclera [4]. The recombinant human growth hormone (rhGH) can increase serum IGF-1 level and can enhance injured brain plasticity, cell regeneration and may lead to functional recovery. Song et al. [5] reported administration of rhGH resulted in the improvement of motor function recovery in completed stroke patients. The purpose of this study was to evaluate effectiveness of rhGH on functional recovery of acute stroke patients.
MATERIALS AND METHODS
Patient selection
Patients for the trial were selected on the basis of inclusion and exclusion criteria from acute stroke patients visited our emergency room between September 2013 and March 2016 (Table 1). To be eligible for the study, the patient must have symptoms consistent with ischemic stroke National Institute of Health Stroke Scale (NIHSS) between 8 and 15 points. Clear onset time should be over 6 hours. For patients not clear with onset time such as patients who awoke with their symptoms, it was determined that their onset time would start at the observed last normal time. Intravenous tissue plasminogen activator (maximum 4.5 hours) or intra-arterial thrombolysis (maximum 6 hours) were withheld due to time window limitation. All patients underwent a routine brain computed tomography (CT) and magnetic resonance imaging (MRI). Cerebral infarction should be restricted to middle cerebral artery (MCA) (Fig. 1). Patients were excluded when NIHSS was below 8 or over 15 and when cerebral infarction area was not MCA territory. Among the initial 238 patients, 84 had hemorrhagic stroke (intracranial hemorrhage 25, subarachnoid hemorrhage 28, and subdural hemorrhage 31), 26 had onset time below 6 hours, 21 had NIHSS below 8 and over 15 and 52 had ischemic infarction territory other than MCA (anterior cerebral artery 13, posterior cerebral artery 26, basilar artery 10, and vertebral artery 3) and 22 patients disagreed on trial. Final thirty patients were enrolled (male = 19, female = 11). Patients were randomly divided into 3 groups. Ten patients were assigned in treatment with rhGH 6 months plus citicoline 6 weeks (GH6) group (male = 5, female = 5) and 10 patients in the treatment with rhGH 3 months plus citicoline 6 weeks (GH3) group (male = 6, female = 4), and final 10 patients in control group (male = 8, female = 2). GH6 group was treated with rhGH for 6months with citicoline (cytidine-59-diphosphocholine; CDP-choline) co-treatment for 6 weeks, GH3 group for 3 months of rhGH with citicoline for 6 weeks as well, and control group used citicoline only for 6 weeks. All participants or their families provided written informed consent before participation.
Table 1
Inclusion and exclusion criteria

CT, computed tomography; NIHSS, National Institute of Health Stroke Scale; CrCl, creatinine clearance; HbA1c, hemoglobin A1c.
![]()
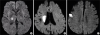 | Fig. 1MRI diffusion weighted image of cerebral infarction areas in MCA territory. MRI diffusion weighted images of enrolled patients had acute ischemic stroke in (A) basal ganglia, (B) corona radiata, and (C) motor cortex, which can influence motor function.
MRI, magnetic resonance imaging; MCA, middle cerebral artery.
|
rhGH treatment
GH6 group received rhGH (Eutropin®; LG Life Sciences Ltd., Iksan, Korea; 4 unit = 1.32 mg) subcutaneous injection once a week for 6 months plus citicoline (Somazina®; Bukwang pharm Ltd., Ansan, Korea) 1,000 mg bid per oral daily for 6 weeks. GH3 group received 3 months of rhGH and 6 weeks of citicoline treatment and control group received only citicoline treatment for 6 weeks. All patients started medication treatment and discharged at any time with oral and injection treatment, continued through the remainder of the treatment period.
Outcome measurement
The primary outcome measure of this study was functional outcome as determined by Korean modified Barthel Index (K-MBI) and modified Rankin Scale (mRS) at baseline and 6 months after treatment by a same single doctor. K-MBI is Korean version of Barthel scale modified in 2007 used to measure performance in activities of daily living. It has 10 categories which has score running from 0–5 (personal hygiene, bathing self), 0–10 (feeding, getting on/off toilet, stair climbing, dressing, bowl control, bladder control), and 0–15 (chair/bed transfer, ambulation). Cut off score below 60 means, independency. The mRS scale runs from 0–6, running from perfect health without symptoms (0) to death (6). Stroke sufferers with mRS 0 to 2 means independent in managing their normal daily activity.
Statistical analysis
Wilcoxon signed-rank test was performed for comparing the changes of K-MBI and mRS in each group at baseline and after treatment. Kruskal-Wallis test was performed for the changes of K-MBI and mRS between 3 groups. Differences were considered significant at p < 0.05 (2-tailed). Statistical analyses were performed by using SPSS 18.0 Statistical Package Program for Windows (SPSS Inc., Chicago, IL, USA).
RESULT
Patient and baseline characteristics
Characteristics of the initial enrolled patients on stroke lesion, onset time, imaging modality were described in Table 2. Before completion of study period, 7 patients dropped out from GH6 group, and 4 patients from GH3 group. Finally, 3 patients in GH6 group (male = 1, female = 2), 6 patients in GH3 group (male = 3, female = 3), and 10 patients in control group (male = 8, female = 2) were analyzed. The baseline demographic characteristics of final analyzed patients were demonstrated in Table 3. All the characteristics showed no statistically different except in sex ratio, smoking, and alcohol consumption. The control group showed more male preponderance (M:F ratio of 1:2, 3:3, and 8:2 in GH6, GH3, and control groups, p = 0.013), smoking tendency (10.50 ± 3.72, 10.62 ± 5.91, and 18.35 ± 9.98 pack-year in GH6, GH3, and control groups, respectively, p = 0.031) and alcohol consumption (weekly alcohol drinking of 0.21 ± 0.11, 0.38 ± 0.22, and 0.96 ± 0.54 bottle in GH6, GH3, and control groups, respectively, p = 0.037) than other 2 groups.
Table 2
Patient characteristics regarding lesion, onset time, and imaging modality

GH6, treatment with recombinant human growth hormone 6 months plus citicoline 6 weeks; BG, basal ganglia; MRI, magnetic resonance imaging; D, drop-out; CR, corona radiata; CT, computed tomography; GH3, treatment with recombinant human growth hormone 3 months plus citicoline 6 weeks; IC, inferior colliculus; PCA, posterior cerebral artery.
![]()
Table 3
Baseline characteristics of final analyzed patients

GH6, treatment with recombinant human growth hormone 6 months plus citicoline 6 weeks; GH3, treatment with recombinant human growth hormone 3 months plus citicoline 6 weeks; ER, emergency room; NIHSS, National Institute of Health Stroke Scale; BP, blood pressure; Hba1c, hemoglobin A1c; LDL, low density lipoprotein.
![]()
Changes in functional outcomes within and between groups
The mean scores of K-MBI and mRS were demonstrated in Table 4. K-MBI score increased in all 3 groups by intra-group analysis during the study (37.5% [p = 0.018], 38.1% [p = 0.027], and 70.9% [p = 0.011] in control, GH3, and GH6 group, respectively). In inter-group analysis, GH6 group showed statistically significant increment than control group (p = 0.042). Meanwhile, GH3 failed to show statistically significant increment than control group (p = 0.054) (Fig. 2). The mRS score decreased in all 3 groups by intra-group analysis during the study (22.1% [p = 0.013], 22.0% [p = 0.033], and 40% [p < 0.001] in control, GH3, and GH6 group, respectively). In inter-group analysis, however, the GH6 group only showed statistically significant decrement of mRS score (p = 0.026) compared to GH3 group (p = 0.394) (Fig. 3).
Table 4
K-MBI and mRS at baseline and 6 months after treatment

K-MBI, Korean version of modified Barthel Index; mRS, modified Rankin Scale; GH3, treatment with recombinant human growth hormone 3 months plus citicoline 6 weeks; GH6, treatment with recombinant human growth hormone 6 months plus citicoline 6 weeks.
![]()
 | Fig. 2The K-MBI score change in 3 groups. K-MBI score increased in all 3 groups by intra-group analysis during the study (p < 0.05). In inter-group analysis, GH6 group showed significant increment than control (p = 0.042). GH3 group however, failed to show significant increment than control group (p = 0.054).
K-MBI, Korean version of modified Barthel Index; GH6, treatment with recombinant human growth hormone 6 months plus citicoline 6 weeks; GH3, treatment with recombinant human growth hormone 3 months plus citicoline 6 weeks; NS, not significant.
|
 | Fig. 3The mRS score change in 3 groups. The mRS score decreased in all 3 groups by intra-group analysis during the study (p < 0.05). In inter-group analysis GH6 group showed significant decrement than control group (p = 0.026). GH3 group however, failed to show significant decrement than control group (p = 0.394).
mRS, modified Rankin Scale; GH6, treatment with recombinant human growth hormone 6 months plus citicoline 6 weeks; GH3, treatment with recombinant human growth hormone 3 months plus citicoline 6 weeks; NS, not significant.
|
DISCUSSION
The objective of this study was to investigate whether the use of rhGH would be helpful for functional recovery in acute stroke patients in proportional to treatment duration. The reason why this study excluded other cerebral artery infarction other than MCA is because K-MBI and mRS scale mostly reflects motor functional deficit. We aimed to concentrate primarily on rhGH and motor dysfunction recovery other than sensory, balance, cognition, or mood problems.
To compare rhGH effect among 3 groups, all the populations in this study had received nearly same management such as dual (sometimes triple) antiplatelet, warfarin or non-vitamin K antagonist oral anticoagulation, statin, antidiabetic and antihypertensive medication therapy along with citicoline until reaching 1 year after the stroke. This could be achieved easily because most of drugs are used to control stroke risk factors that could not be quitted halfway.
Citicoline is well known neuroprotective adjuvant treatment in ischemic stroke and Korean health insurance review and assessment service admit and permit citicoline use of 2,000 mg/day/6-week if initial NIHSS scale is 8 or over starting within 24 hours of stroke onset [67]. Citicoline has therapeutic effects at several stages of the ischemic cascade in acute ischemic stroke and has demonstrated efficiency in a multiplicity of animal models of acute stroke. Long-term treatment with citicoline is safe and effective, improving post-stroke cognitive decline and enhancing patients' functional recovery [8].
All the study populations involved in our study scored more than 8 points. So basically, all the 3 groups (citicoline plus rhGH 6 months, citicoline plus rhGH 3 months, citicoline alone) used citicoline. In this study, GH6 group showed improvement in the K-MBI and mRS score compared to control group after the treatment. GH3 group, however, showed no statistically significant improvement from control. The result from this study highlight prolonged and continuous treatment with rhGH have additive therapeutic potency in functional recovery of stroke patients.
The rhGH increases IGF-I and IGF-1 is a pleiotropic pivotal peptide that exerts prosurvival signals on neurons, oligodendrocytes, and other glial cells. IGF-1 also inhibits glutamate, nitric oxide, and hydrogen peroxide-induced apoptosis and able to modulate brain plasticity by influencing neurite outgrowth, synaptogenesis, neuronal excitability, and neurotransmitter release [91011]. The rhGH, in addition, promote improvement of body components such as muscle fiber, bone mineralization to improve muscle strength and exercise performance, ocular tissues such as extracellular matrix of the sclera for emmetropization. Previous animal model studies proposed that rhGH increased serum IGF-1 level and it is essential for recovery of the nervous system. Other studies reported cognitive function such as mini mental status evaluation score did not changed even though motor function increased compared to control. These findings seem to suggest that rhGH not only increases neuronal regeneration but also related to gain of muscle function [12]. These could be one of the reason for explanation of prolonged rhGH efficacy on motor function recovery even after insulted nerve stabilized.
Acute stroke patients have lower IGF-1 level and furthermore, rhGH-induced elevation of level of IGF-1 does not sustain after quitting exogenous rhGH probably due to growth hormone — IGF-1 axis negative feedback adaptation [5]. Therefore, it appears that early start and repeated supply of rhGH could be beneficial. Present study compared 3-month and 6-month rhGH treatment outcome. As a consequence, functional outcome from longer treatment of rhGH was better. So, we should expect more effective results by continuous rhGH even after 6 months and dose elevation.
This study had several limitations. First, the number of initial enrolled subject was small and it was open-labeled study. Second, we could not collect data on serial serum IGF-1 level and rehabilitation treatment methods because patients transferred to other rehabilitation centers immediately after the acute stroke manage. Therefore, whether the rhGH therapy can exactly increase serum level of IGF-1, which could not be determined in our study. The correlation of IGF-1 in the rhGH treatment and functional outcome should be enlightened through further studies. Third, many patients dropped out during the study due to prolonged use of rhGH. Since the number of each group decreased, statistical confidence could be declined. The reasons of high drop-out rates during the study were due to cost and distance. The drop out patients or their family could not afford the cost of rhGH for that long period (54,750 Korean won or 49 US dollar/week). Next, after finishing acute treatment for one week, the patients were transferred to rehabilitation hospital or nursing home. Even though patients and their family accepted initial rhGH treatment, they soon retracted their will due to inconvenience. Fourth, we excluded mild and severe stroke patients (NIHSS < 8 or > 15) which could have affected the outcome of the study. However, we presumed that patients with very mild stroke symptoms (NIHSS < 8) could expect good recovery with pre-existing standard treatment and because of the ceiling effect, we thought it would be hard to compare between treatment groups. On the other hand, patients with severe symptoms (NIHSS > 15) were unable to properly determine the function recovery due to frequent infections or other complications. Fifth, because the patients transferred to different rehabilitation centers after acute stroke manage, we could not control various factors affecting post stroke functional outcome, such as rehabilitation program, depression control and previous cognitive function. Socioeconomic status could affect functional outcome as well. In addition, functional recovery measures other than K-MBI and mRS such as manual muscle strength test, Fugl-Meyer assessment, fatigue scale, and Korean version of the mini-mental status examination could not be performed. Finally, we could not conduct brain MRI follow up after the study. In general, it is not recommended to repeat brain MRI within 2 years after stroke if there is no indicative symptom change. Therefore, to explore whether rhGH treatment facilitated functional outcome and IGF-1 level increased in proportion to rhGH dose, studies with double blind, large sample size, long-term IGF-1 level collection, controlling many factors affecting functional outcome, many functional recovery measurement scale and less drop out study plan are needed. Also, serial brain MRI follow up study and higher doses of rhGH treatment trial should be needed to find out whether it has further beneficial effect on functional and imaging outcome.
However, in spite of above-mentioned many limitations such as no direct data on method, duration, intensity of physical/psychiatric rehabilitation program which could give a big impact on functional recovery, we could collect from families or caregivers of patients about rehabilitation time, frequency, how well the patient performs and cognition, mood changes. Of the patients enrolled in this study, no special drug adjustment was made until the end of the study. In addition, it is estimated that patients obtained similar rehabilitation therapy in average because, due to insurance related issues in Korea, patients need to move hospital to hospital in every 3 months and treatment protocol, equipment and services of every rehabilitation hospital are basically similar. And finally, although there were small numbers in each group, mRS and K-MBI score showed statistically significant improvement in intra-group analysis and based on these findings, inter-group analysis showed GH6 group improved more than GH3 and control group. For the above reasons, we could conclude that the effects of rhGH are significant.
In conclusion, prolonged administration of rhGH treatment at least 6 months could give effect on functional outcome in acute stroke patients.
 XML Download
XML Download