

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Dear Editor,
Sjogren's syndrome is characterized by the involvement of exocrine glands, predominantly the salivary and lacrimal glands. The commonly reported central nervous system (CNS) presentations include a multiple sclerosis-like presentation with focal or multifocal white matter lesions, cranial nerve palsies, and myelitis.1 Small-vessel vasculitis has often been postulated as a pathogenic mechanism of the CNS involvement in Sjogren's syndrome,23 but the involvement of major cerebral vessels in Sjogren's syndrome has only rarely been reported.456
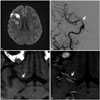
A 50-year-old female without vascular risk factors presented with recurrent episodes of right-hemispheric transient ischemic attacks involving left upper limb paresthesia and weakness, with complete recovery of symptoms after several minutes, and two episodes of righthemispheric minor stroke with recovery after 2 days. The patient also reported dryness of the eyes with no joint or cutaneous symptoms. An examination revealed no focal neurological deficits. The routine blood parameters, ESR, and findings of a CSF study were normal. The antinuclear antibody profile revealed strong positivity for anti-Sjogren's-syndrome-related antigen A(SSA/Ro), anti-Sjogren's-syndrome-related antigen B (SSB/La), and PM-Scl. Schirmer's test was positive for dry-eye syndrome. Head CT revealed infarcts in the right middle cerebral artery (MCA) and anterior cerebral artery (ACA) deep watershed territory, and in the MCA and posterior cerebral artery cortical watershed territory. CT angiography revealed stenosis of the right supraclinoid and communicating segments of the intracranial internal carotid artery (ICA). Digital-subtraction angiography showed 80% stenosis of the right supraclinoid ICA with normal distal smaller vessels. High-resolution MR vessel wall imaging (HRVWI) revealed smooth homogeneous concentric wall thickening with enhancement involving the communicating segment of the right ICA, the proximal M1 segment of the MCA, and the A1 segment of the ACA, without any significant positive or negative remodeling, suggestive of vasculitis of the terminal right ICA and its branches. Large-vessel vasculitis secondary to Sjogren's syndrome was diagnosed. The patient was treated for 5 days with intravenous methylprednisolone followed by oral prednisolone, along with mycophenolate mofetil and hydroxychloroquine. The patient had not experienced any further cerebral ischemic events at a 3-month follow-up.
This case demonstrates vasculitis of cerebral large-vessels in a patient with primary Sjogren's syndrome and provides further insight into the pathogenesis of the CNS involvement in Sjogren's syndrome. Our patient had dry-eye syndrome, based on a positive Schirmer's test, and strong positivity for SSA/Ro and SSB/La, suggestive of Sjogren's syndrome. The presence of right supraclinoid ICA stenosis in a setting of primary Sjogren's syndrome suggested a vasculitic etiology. The alternative possibilities considered were intracranial atherosclerotic disease and moyamoya disease. The homogenous concentric thickening and enhancement involving the communicating segment of the right ICA and a few millimeters of the proximal M1 segment of the MCA and the A1 segment of the ACA, without any significant positive or negative remodeling, is characteristic of vasculitis. Eccentric wall thickening and the juxtaluminal T2-weighted hyperintensity that is evident in intracranial atherosclerotic disease was not seen in our patient. The absence of collateral vessels on angiography as well as the absence of negative remodeling in HRVWI excluded the possibility of moyamoya disease.
Vasculitis is one of the mechanisms underlying CNS involvement in primary Sjogren's syndrome. Vasculitis involving small and medium-size vessels has been demonstrated in histopathological examinations of brain and spinal cord specimens, and in angiography of patients with Sjogren's syndrome.37 Large-artery involvement in Sjogren's syndrome is rare, with only three cases reported in the literature456 We did not perform a histopathological confirmation of vasculitis and follow-up HRVWI after treatment to look for resolution of the vessel-wall enhancement. Our case highlights the presence of vasculitic involvement of the large cerebral vessels in primary Sjogren's syndrome, which can be confirmed by HRVWI.
 XML Download
XML Download