

 PDF
PDF ePub
ePub Citation
Citation Print
Print


INTRODUCTION
The immune system provides the immune surveillance that helps prevent the development of various cancers. Observational studies have noted that patients whose immune systems are compromised by human immunodeficiency virus infection or immunosuppressive medication after organ transplants have higher rates of malignancies [12]. In the context of carcinomas, tumor-infiltrating lymphocytes affect tumor growth, and these infiltrates have been associated with tumor prognosis and chemotherapeutic response [3]. Many tumor studies have shown that NK cell cytolytic activity and B- and T-cell interaction inhibit neoplastic cells [45].
The role of the immune system in hematologic malignancies is not entirely understood, although previous studies have suggested that T and/or NK cells play critical roles in the progression of malignant lymphoma and acute myeloid leukemia (AML) [678]. Most studies that evaluated immune cells in AML have addressed functional abnormalities, but only a few studies have shown that the relative or absolute number of T and/or NK cells differs between patients with AML and healthy controls. Moreover, lymphocyte subsets were found to differ among patients with various AML subtypes [891011].
Lymphocytes are excluded from malignant myeloid clones, and T and NK cells are known to be mainly involved in AML blast recognition [1213]. The functional link between B cells and AML blasts is unknown, although B cells may reflect the overall health of the bone marrow environment. The composition of lymphocyte subsets is altered by chemotherapy and stem cell transplantation, as immune reconstitution occurs [1415]. Thus, the baseline composition of lymphocyte subsets at diagnosis may be relevant in understanding host-tumor immunologic interactions.
Relatively little is known about the prognostic value of the baseline composition of lymphocyte subsets with regards to AML outcomes. High initial absolute lymphocyte count (>4.8×103/µL), which correlates with adverse outcomes, was found to be associated with a lower percentage of NK cells but not with differences in T and B cell percentages [16]. Another study showed that ≥5% NK cells and increased B cells were associated with improved prognoses [8].
In this study, we analyzed the distribution of lymphocyte subsets in patients with AML at diagnosis and determined their relationship with AML subtype. We also identified the prognostic impact of lymphocyte subset proportions.
MATERIALS AND METHODS
Population
This retrospective study evaluated patients aged <65 years who were newly diagnosed with AML between January 2013 and May 2016. Patients were excluded if they had any underlying autoimmune disease or evidence of concurrent bacterial or viral infections. Patients were classified using the 2016 WHO classification for hematopoietic and lymphoid neoplasms and categorized into cytogenetic risk groups according to the Medical Research Council criteria [1718].
Patients with acute promyelocytic leukemia (APL) were treated with all-trans retinoic acid and idarubicin, and the other patients with AML received induction chemotherapy with cytarabine at 100 mg/m2 per day for seven days plus daunorubicin at 45 mg/m2 per day, or idarubicin at 12 mg/m2, for three days. We applied consolidation chemotherapy, which consisted of a 3+5 regimen that consisted of daunorubicin (45 mg/m2) or idarubicin (12 mg/m2) for three days plus an intermediate dose of cytarabine (1.0 g/m2 every 12 hr) for five days. The conditioning regimen in allogeneic peripheral blood hematopoietic stem cell transplantation (allo-PBSCT) for AML was busulfan (6.4 mg/kg) and fludarabine (150 mg/m2).
Complete remission (CR) was defined as a <5% reduction in blasts in the bone marrow, with neutrophil counts >1×103/µL and platelet counts >100×103/µL [19]. Disease-free survival (DFS) was measured from the date of CR to the date of relapse, and overall survival (OS) was measured from the date of CR to the date of death or last follow-up. The medical records were reviewed, and this study was approved by the institutional review board.
Flow cytometric analysis of lymphocyte subsets
Two sets of four-color monoclonal antibody combinations (tetraCHROME; Beckman Coulter, Mervue Galway, Ireland) were used for the flow cytometric analysis of lymphocyte subsets. Panel 1 was composed of anti-CD45 fluorescein isothiocyanate (FITC)/anti-CD4 phycoerythrin (RD1)/anti-CD8 phycoerythrin-Texas Red-x (ECD)/anti-CD3 phycoerythrin-cyanine 5 (PC5), while Panel 2 was composed of anti-CD45 FITC/anti-CD56 RD1/anti-CD19 ECD/anti-CD3 PC5.
Tubes were labeled as Panel 1 and Panel 2, and 100 µL of EDTA-treated whole blood and 10 µL of the monoclonal antibody combinations were added to each labeled tube. The mixture was incubated for 15 minutes at room temperature in the dark. Red blood cells were lysed with the ImmunoPrep reagent system and the TQ-Prep workstation (Beckman Coulter). Flow cytometry analysis was performed on a Cytomics FC 500 flow cytometer (Beckman Coulter).
Statistical analysis
All statistical analyses were performed using MedCalc statistical software 14.12.0 (MedCalc Software, Mariakerke, Belgium). Continuous variables are presented as the median (range). The Mann-Whitney test or Kruskal-Wallis test was used to compare continuous variables, and the Chi-square test was used to compare categorical variables. The relationships between continuous variables was assessed using the Pearson's correlation coefficient. DFS and OS were estimated using a Kaplan-Meier analysis, and a log-rank test was used for univariate analyses to evaluate survival differences between groups. Variables with P<0.2 were included in the multivariate analysis, which was performed based on the Cox proportional regression model. A P-value <0.05 was considered statistically significant.
RESULTS
Patient characteristics
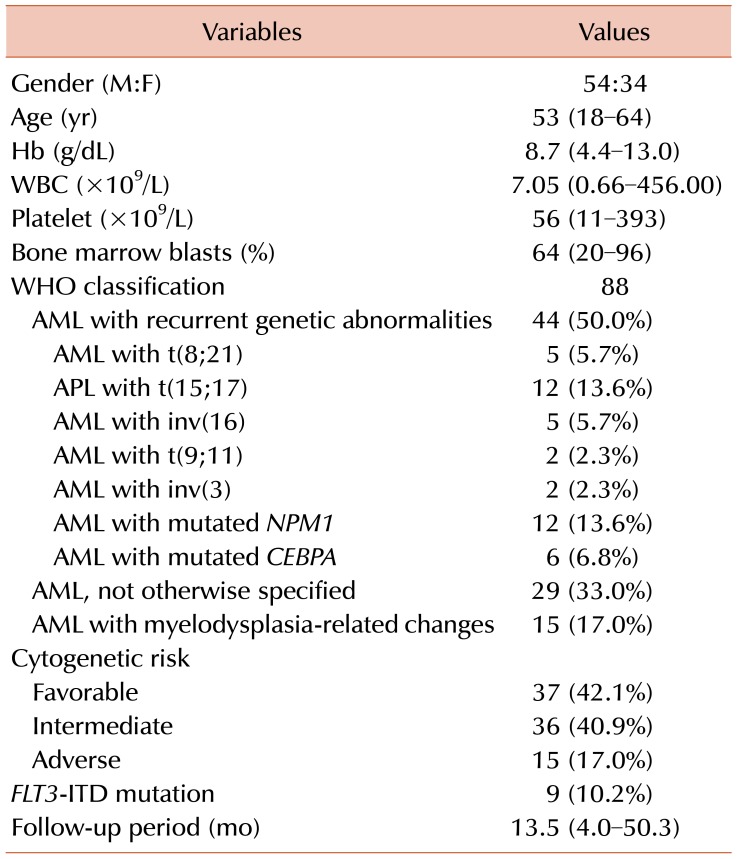
This study included 88 patients (54 men and 34 women) with a median age of 53.0 years (range, 18–64 yr), 79 of whom had de novo AML, and nine had secondary AML (antecedent hematologic disorder related). Based on the WHO classification, 44 patients had AML with recurrent genetic abnormalities, 29 had AML not otherwise specified (AML-NOS), and 15 had AML with myelodysplasia-related changes (AML-MRC). NPM1 and CEBPA mutations were detected in 13.6% (12/88) and 6.8% (6/88) of the patients, respectively. The FLT3-ITD mutation was detected in 10.2% (9/88) of the patients. Genetic risks were favorable in 37 (42.1%), intermediate in 36 (40.9%), and adverse in 15 (17.0%) patients. Patient characteristics at diagnosis are shown in Table 1.
Of the 76 patients in the non-APL cohort, five were transferred to other hospitals, 67 achieved CR, and four died before achieving CR. Of the 67 patients in remission, 35 underwent stem cell transplantation during the follow-up period.
Relationship of AML subtypes and lymphocyte subsets
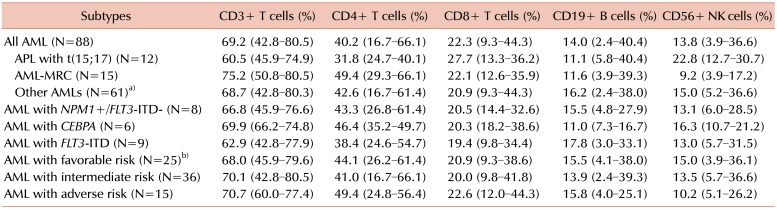
In the 12 patients with APL with a t(15;17)(q22;q12) chromosomal translocation, the median percentages of CD3+ pan T cells (60.5% vs. 69.9%, P=0.0209) and CD4+ helper T cells (31.8% vs. 43.5%, P=0.0015) were significantly lower, and the median percentage of CD56+ NK cells (22.8% vs. 13.2%, P=0.0011) was significantly higher than those in the 76 patients of the non-APL cohort. However, the percentages of CD8+ cytotoxic T cells and CD19+ B cells did not differ between these two groups. Regardless of the relative percentages of lymphocyte subsets, the absolute counts of all lymphocyte subsets were lower in the APL group than in the non-APL group, due to the lower median lymphocyte counts in the former (715/µL vs. 1,785/µL, P<0.0001).
The median percentages of CD3+ T cells (75.2% vs. 68.7%, P=0.0166) and CD4+ T cells (49.4% vs. 42.6%, P=0.0405) were significantly higher in the 15 patients with AML-MRC than in the 61 other patients with AML, excluding those with APL. However, the percentages of CD8+ T cells, CD19+ B cells, and other T and B cell subsets did not differ between these two groups. The median percentage (9.2% vs. 15.0%, P=0.0027) and absolute counts (115/µL vs. 278/µL, P=0.0160) of CD56+ NK cells were lower in the AML-MRC cohort.
The percentages of lymphocyte subsets did not differ between the groups of patients with and without NPM, CEBPA, and FLT-ITD mutations. The percentage of NK cell cells was lower in the 15 patients with adverse genetic risks than in the 25 patients with favorable genetic risk, but this difference was not significant (P=0.0673). The percentages of other lymphocyte subsets showed no differences according to cytogenetic risks (Table 2).
NK cell subsets and their relationships to patient outcomes
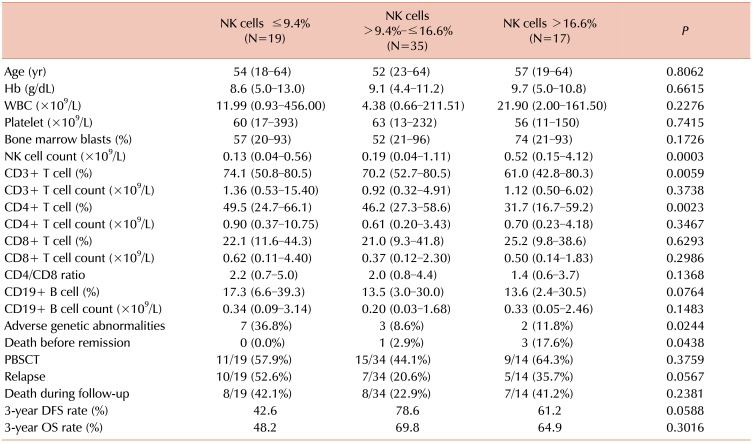
Since patients with APL with a higher percentage of NK cells have a more favorable prognosis than patients with any other AML subtype, we evaluated the clinical significance of NK cells in the 71 patients of the non-transferred non-APL group. The median percentage of NK cells was 13.0% (range, 3.9–36.6%), with 70 (98.6%) patients having ≥5.11% NK cells, which is the lower limit of the reference range for Korean patients [20]. Based on the 25th and 75th NK cell percentiles, these patients were divided into three groups: low (≤25th percentile, ≤9.4%), medium (>25th and ≤75th percentile), and high (>75th percentile, ≥16.6%) NK cell percentages (Table 3).
The group with high NK cell percentage had significantly lower percentages of CD3+ T cells (P=0.0059) and CD4+ helper T cells (P=0.0023) than the other two groups. In contrast, the CD3+ T cells and CD4+ helper T cell counts, and the counts and percentages of CD8+ cytotoxic T cells and CD19+ B cells, did not differ among the three groups. The NK cell count (P=0.0003) was significantly higher in the group with high NK cell percentage than in the other groups.
Hemoglobin, white blood cell (WBC) count, and platelet count showed no differences among the groups. Also, the blast percentage in bone marrow did not differ significantly among the three groups of patients, who differed by NK cell percentage. However, the percentage of NK cells weakly correlated with the percentage of bone marrow blasts (r=0.2714, P=0.0220) (Fig. 1).
The incidence of adverse cytogenetic abnormalities was higher in the group with low NK cell percentage (P=0.0244), and death before CR was more frequent in the group with high NK cell percentage (P=0.0438) than in the other two groups. The relapse rate was higher in the group with low NK cell percentage than in the groups with medium or high NK cell percentages, but these differences were not statistically significant (P=0.0567). The incidence of PBSCT and death rate during follow-up showed no significant differences between the groups.
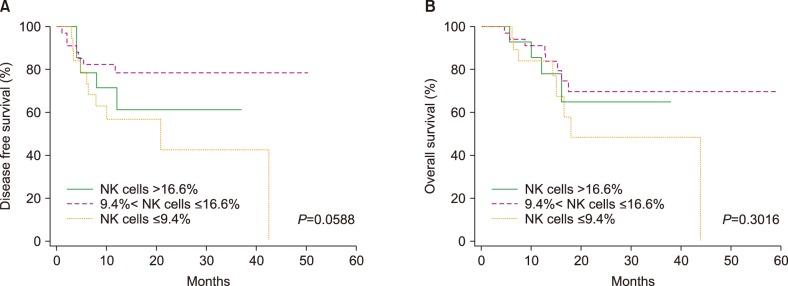
The 3-year DFS rates in the groups with low, medium, and high NK cell percentages were 42.6% (95% CI, 41.1–44.1%), 78.6% (95% CI, 71.4–85.8%), and 61.2% (95% CI, 47.2–75.2%), respectively. DFS was shorter in the group with low NK cell percentage than in the other groups, but this difference was not statistically significant (P=0.0588). The 3-year OS rates in patients with low, medium, and high NK cell percentages were 20.6% (95% CI, 4.3–36.9%), 69.8% (95% CI, 60.5–79.1%), 64.9% (95% CI, 49.8–80.0%), respectively, and none of these differences were statistically significant (P=0.3016) (Fig. 2).
Multivariate analysis for DFS and OS
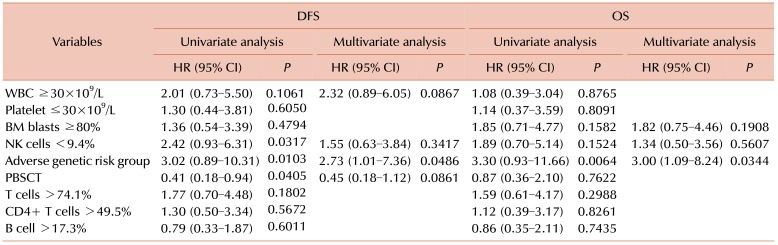
Multivariate logistic regression analyses were performed to assess the relationships between NK cell subsets and clinical outcomes. The factors that were analyzed included high WBC count, low platelet count, high marrow blast percentage, poor genetic risk, and low NK percentage. Because the group with low NK percentage tended to show higher median percentages of pan T, CD4+ T, and B cells, the significance these cell percentages that exceeding their medians was also evaluated.
The multivariate analysis showed that adverse genetic risk was the only factor that was independently predictive of poorer OS and DFS (Table 4). A higher WBC count at diagnosis (≥30.0×109/L; P=0.0867) and PBSCT (P=0.0861) were associated with the risk of relapse, but the relationships were not statistically significant. Platelet count, bone marrow blast percentage, low NK cell percentage, and high T and B cell percentages were not associated with DFS. None of the variables that were evaluated, except for adverse genetic risk, was associated with OS.
DISCUSSION
Immune system cells are essential for targeting and recognizing malignant cells, and the robust immune responses that are mediated by T and NK cells are responsible for the graft-versus-leukemia effect. Although the prognostic significance of morphologic, immunophenotypic, and genetic characteristics has been extensively evaluated in AML, less is known about anti-leukemic immune responses [891011]. In chronic lymphocytic leukemia, higher percentages of T and NK cells, relative to malignant monoclonal B-cells, reflect greater host immunity and relate to a more indolent disease course [21]. Few studies have evaluated the relationship between the percentages of NK cells and clinical outcomes in AML; however, the impact of T and B cell subsets has not been identified [821].
Since lymphocyte subset reference ranges are thought to differ among races, we selected the reference ranges for Korean subjects for comparisons [20]. The distributions of lymphocyte subsets have been reported to differ in patients with AML and healthy controls [91122]. One study found that the number of blood NK cells was higher in patients with AML than in healthy controls, whereas the number of T cells was similar in the two groups [11]. In contrast, other studies have reported that the absolute number of T cells was significantly higher, and the percentage of marrow NK cells significantly lower, in patients with AML [922]. Although our study analyzed lymphocyte subsets in the peripheral blood, the numbers of peripheral blood T, B, and NK cells at the time of diagnosis varied among patients with AML, and the median numbers and percentages of T and NK cells in patients with newly diagnosed AML were similar to those in healthy controls. However, we observed distinct patterns of lymphocyte subset proportions in a few specific AML subtypes, which is consistent with previous findings [8].
Compared with other AML subtypes, APL with the t(15;17) chromosomal translocation was associated with a higher percentage of NK cells and lower percentages of pan T cells and CD4+ helper T cells. In contrast, the NK cell percentage was higher, and pan T cell and CD4+ helper T cell percentages were lower, in patients with AML-MRC. Genetic risk category and molecular features, such as CEBPA, NPM1, and FLT3-ITD mutations, were not associated with differences in the percentages of lymphocyte subsets, although the NK cell percentage tended to be lower in the adverse genetic risk group than in the favorable genetic risk group (P=0.0673). These results suggest that a particular leukemic clone can influence the proportions of blood NK and CD4+ T cells.
A previous study reported that ≥5% NK cells in the blood was associated with improved survival. In the present study, 70 of the 71 patients of the patients in the non-APL cohort had ≥5% NK cells, limiting the usefulness of this cutoff. A recent study reported that a lower proportion of bone marrow NK cells (≤15%) at diagnosis correlated with better survival in patients with AML. We therefore compared patients with low (≤25th percentile) and high (>75th percentile) NK cell percentages. We found that the frequency of adverse genetic abnormalities was higher in the group with low NK cell percentage and that death prior to remission was more frequent in patients with high NK cell percentages.
Although the group with high NK cell percentage did not show a significantly higher marrow blast percentage, NK cell percentage weakly correlated with the percentage of bone marrow blasts (r=0.2714) and was higher in patients with APL who had a high percentage of leukemic promyelocytes. The higher rate of death prior to remission in the group with high NK cell percentage may be related to cytopenia, which is caused by the overproduction of leukemic cells, because the causes of death were cerebral hemorrhage and infection.
The patients with low NK cell percentage also tended to have a higher relapse rates and shorter DFS than patients with higher NK cell percentage. However, death rate during the follow-up period and OS did not differ. The multivariate analysis showed that low NK cell percentage was not an independent risk factor for DFS. Rather, adverse genetic risk was the most important predictor of DFS and OS.
The percentages of T and B cells were higher in the group with low NK cell percentage than in the groups with medium or high NK cell percentages. However, survival time was not affected by T and B cell percentages. Circulating T cells are composed of various subsets. Several of these specific T cell subsets, including regulatory T cells, CD3+CD56+ cells, and CD3+CD5+ cells, have been found to differ among subsets of patients with AML [89102324]. In this study, the percentages and counts of pan T cells and traditional T cell subsets (CD4+ cells and CD8+ cells) at diagnosis were similar to those in a healthy population and were not associated with clinical outcomes [1125]. However, our study had a limitation in assessing the role of T cells because we did not numerically analyze the different T cell subsets or assay T cell function.
In conclusion, measurable characteristics of lymphocyte subsets at the time of AML diagnosis appear to be helpful in the differentiation of specific subtypes. In non-APL, the low proportion of NK cells is associated with high frequencies of concurrent adverse genetic abnormalities, and the high proportion of NK cells are possibility associated with death before remission. The proportions of lymphocyte subsets, including the NK cell subset, do not show independent correlations with clinical survival.

 XML Download
XML Download