

 PDF
PDF ePub
ePub Citation
Citation Print
Print



INTRODUCTION
Mitral regurgitation (MR) is a frequent complication and a powerful predictor of long-term cardiovascular mortality after acute myocardial infarction (AMI) (1, 2, 3, 4, 5). Although left ventricular (LV) ejection fraction (EF) is a determinant of poor prognosis and an accurate marker of LV systolic dysfunction, the prognostic value of LVEF after MI has been questioned (6). In patients with chronic MR, LVEF underestimates the degree of LV systolic dysfunction because of volume overload. LVEF is also highly influenced not only by LV contractility but also by LV geometry, loading condition, and MR severity (7, 8). In patients with AMI, low LVEF can be the result of reduced contractile function due to extensive myocardial damage, LV dilatation, or myocardial stunning (9).
The role of LVEF as a prognostic factor in AMI patients with significant MR has been poorly addressed (10, 11). Furthermore, the prognostic value of LVEF in AMI patients with severe MR has not been previously reported. This study aimed to examine the prognostic significance of LVEF in the long-term outcome of AMI patients with or without severe MR in the clinical setting.
MATERIALS AND METHODS
Study population
The Korean Acute Myocardial Infarction Registry (KAMIR) is a Korean, prospective, open, observational, multicenter, on-line registry of AMI data with support from the Korean Society of Cardiology that was initiated in November 2005. The 50 participating hospitals are capable of performing primary percutaneous coronary intervention (PCI). Details of the KAMIR have been published previously (2, 12, 13). A total of 15,097 patients with AMI who received echocardiography were registered in the KAMIR between January 2005 and July 2011. Patients with low-grade MR (grade 0-2) were divided into two groups according to LVEF, namely, LVEF≤40% (n=2,426) or EF>40% (n=12,252). Patients with high-grade MR (grade 3-4) were similarly divided into two groups (EF≤40% [n=197] or EF>40% [n=226]).
The endpoints of the study were major adverse cardiac events (MACE), cardiac death, and all-cause death during the year following registration. MACEs were defined as the composite of all-cause death, MI, and repeated PCI or coronary artery bypass grafting (CABG) during 12 months of clinical follow-up.
The follow-ups in the outpatient clinic occurred immediately after hospital discharge, one month post-discharge, and at intervals of less than 6 months thereafter. Information on events and mortality was obtained from hospital records and phone calls.
Coronary angiogram
Coronary angiograms were performed using standard techniques. Significant coronary artery disease (CAD) was defined as ≥70% stenosis of an epicardial coronary artery. The extent of CAD was characterized by one-, two-, or three-vessel disease or left main disease (14, 15). Percutaneous coronary intervention (PCI) was performed according to the physician's discretion. Coronary blood flow in the infarct-related artery before and after stent implantation was graded according to the classification used in the Thrombolysis in Myocardial Infarction trials.
Echocardiography
All index transthoracic echocardiographs were recorded during routine clinical practice according to the current guidelines (16). Two-dimensional M-mode echocardiography and Doppler ultrasound examinations were performed within 3 days of the PCI.
In each patient, LVEF was measured using bidimensional echocardiography from two- and four-chamber apical views by the modified Simpson's method (17). The wall motion score index was derived according to a 17 segment model (18). For each segment, wall motion was scored from 1 (normal) to 4 (dyskinesia). The presence and degree of MR were measured using the proximal isovelocity surface area (PISA) method and a validated nomogram for semi-quantitative estimation (19). MR was classified into four degrees of severity (I: mild, II: mild to moderate, III: moderate, IV: severe).
Statistical analysis
Data are expressed as the means±SD for continuous variables and absolute numbers (proportions) for categorical variables. All comparisons between baseline variables were performed by the Pearson chi-square test for categorical variables and the t-test for continuous variables.
Cox proportional hazards regression was used to estimate the relative mortality risk at 1 yr. We controlled for all available variables considered potentially relevant in all regression analysis of low-grade MR (grade 0-2) and high-grade MR (grade 3-4): age, gender, Killip class, Q wave on electrocardiography (ECG), Ischemic heart disease history (IHD), diabetes mellitus (DM), N-terminal pro-B type natriuretic peptide (NT-proBNP), glucose level, high-sensitivity C-reactive protein (Hs-CRP), LVEF, estimated glomerular filtration rate (eGFR), and PCI. Best cut-off values of continuous variables were assessed by the receiver operating curve. All statistical tests were 2-sided, and a P value <0.05 was considered statistically significant. Statistical analysis was performed using SPSS 18.0 for Windows (SPSS, Inc., Chicago, IL, USA). Survival analysis was performed using the Kaplan-Meier method with log-rank tests to compare survival between groups.
RESULTS
Baseline clinical characteristics and laboratory findings
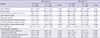
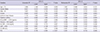
The baseline clinical characteristics are presented in Table 1. Among the patients with low-grade MR (grade 0-2), the patients in the LVEF≤40% group were older, were more likely to be women, had decreased body mass indexes (BMIs) and blood pressures, had higher heart rates and Killip classes and were more likely to have histories of hypertension, DM, and IHD compared with the patients in the LVEF>40% group. Patients with reduced LVEF were more likely to present STEMI, Q waves, and atrial fibrillation/flutter on electrocardiography. However, among the patients with high-grade MR (grade 3-4), the patients in the LVEF≤40% group were more likely to be men, have higher heart rates, have histories of DM and IHD, and present Q waves on ECG compared with the patients in the LVEF>40% group. Regardless of MR grade, the LVEF≤40% group had higher glucose, Hs-CRP, and NT-proBNP levels compared with the LVEF >40% group (Table 2).
Coronary angiogram
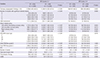
In AMI patients with low-grade MR (grade 0-2), the LVEF≤40% group had more severe coronary angiogram findings than the LVEF>40% group (Table 3). However, in patients with high-grade MR (grade 3-4), the LVEF≤40% group had no significantly different coronary angiographic findings, except for left anterior coronary artery disease, compared with the LVEF>40% group. PCI was performed in a significantly lower number of patients in the high grade MR group as compared to the low grade MR group. However, based on LVEF, there was no significant difference between the number of PCI performed on patients in the high grade MR group (Table 3).
Independent predictors of mortality
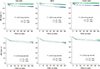
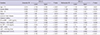
The independent predictors of cardiac death in the multivariate analysis in AMI patients with low-grade MR were age≥75 yr, Killip class≥III, IHD history, NT-proBNP>4,000 pg/mL, Hs-CRP ≥2.59 mg/L, eGFR, PCI, and LVEF≤40% (Table 4). However, PCI was an independent predictor in patients with AMI with high-grade MR (Table 5). Primary endpoints in the MR grade 0-2 group based on Kaplan-Meier analysis were significantly different according to EF (EF≤40% vs. EF>40%, total death, 330/2,422 vs. 373/12,252, P<0.001; MACEs, 489/2,422 vs. 1,091/12,252, P<0.001; cardiac death, 281/2,422 vs. 254/12,252, P<0.001 by the log-rank test). However, primary endpoints among AMI patients with MR grade 3-4 was not different according to EF (EF≤40% vs. EF>40%, total death, 42/197 vs. 37/226, P=0.216; MACEs, 55/197 vs. 49/226, P=0.357; cardiac death, 37/197 vs. 31/226, P=0.216 by the log-rank test) (Fig. 1). Fig. 1 reveals that patients with grades 3-4 MR and preserved EF exhibit a poor prognosis given the advanced age of this patient population compared with groups with low-grade MR (Table 1).
DISCUSSION
The present study showed that in the presence of high-grade MR, LVEF is not an independent predictor of mortality. LVEF is the most widely used variable to represent LV systolic function in patients with AMI. Furthermore, low LVEF was associated with high one-year mortality after AMI in patients without high-grade MR in the present study. Because the majority (97%) of the patients with AMI did not have high-grade MR. However, the prognostic value of LVEF after AMI has been questioned in several studies that could not confirm LVEF as a prognostic factor in AMI patients. Left ventricular end-diastolic volume (LVEDV) and left ventricular end-systolic volume (LVESV) were described as more meaningful prognostic factors than LVEF because a low EF might be attributed to extensive myocardial damage, LV dilatation, or a hibernating or stunned myocardium (6, 9). The present study suggests that ischemic high grade MR could be one reason for this result because LVEDV and LVESV could be increased by volume overload disease, such as ischemic MR. A previous study reported that the presence of MR was associated with an increased likelihood of adverse outcomes but not LV EF in patients with AMI with MR (11).
Ischemic MR could be caused by global LV remodeling with spherical LV enlargement or local inferior wall remodeling with predominantly posterior leaflet restriction. In case of non-ischemic MR, an increase in preload and/or a decrease in afterload will result in a falsely higher EF because the EF is load-sensitive (20). However, some have argued that the 'low impedance leak' effect might exclusively apply to acute severe MR and that the afterload is likely increased when the LV is dilated. Furthermore, the decline in EF following MVR could result from chordal transection. Whitlow et al. (21) have shown that the EF is essentially unchanged at 12 months among patients experiencing significant reductions in MR and 'reverse' remodeling using edge-to-edge clip devices without the confounding effects of CABG, sternotomy, or chordal transection.
Alternatively, a portion of the LV dysfunction in AMI patient results from afterload excess; this finding could explain why reduced LVEF has no impact on survival in patients with severe MR. Accordingly, contractile function might be better than the EF suggests because the LV is managing afterload excess.
The LVEF is derived from the LV volume. Although heart rate and fiber shortening both affect LVEF, it is influenced to a far greater extent by LVEDV given that changes in stroke volume tend to be considerably smaller than changes in LVEDV (22). In the AMI setting, LVEDV is not yet fully dilated by acute severe MR. In addition, ischemic MR might have a transiently severe grade.
LVEF is a determinant of the degree of functional ischemic mitral regurgitation in patients with systolic left ventricular dysfunction (4). However, there is only a weak correlation between LVEF and MR severity (7, 8). Recently, several small population studies have examined the role of assessing LV systolic function in addition to LVEF in ischemic MR (23, 24).
PCI was performed in a significantly lower number of patients in the group of LVEF<40% with low grade MR as compared to the group of LVEF>40% with low grade MR. That could contribute the difference of survival in low grade MR not high grade MR. Furthermore, PCI was an independent predictor of lower cardiac death in high grade MR (Table 4). Reperfusion therapy for patients in AMI with severe MR could be beneficial for survival.
This study was a retrospective study. There are no detailed descriptions of MR volume or effective regurgitant orifice area (ERO) due to a lack of central readings of the echocardiograms in the core laboratory. Furthermore, the etiologies of MR and the presence of non-ischemic MR were not distinguished. Long-term follow-up echocardiography data were limited. The number of patients with severe MR was considerably lower than that in the other group. Nevertheless, this study demonstrated the prognostic impact of LVEF according to the presence of severe MR in a large, real-world population.
In conclusion, MR is a predictor of poor outcome regardless of ejection infarction. LVEF is an inadequate method to evaluate contractile function of the ischemic heart in the face of high grade MR. Other new parameters for assessing LV systolic function beyond LVEF are needed in patients with significant ischemic MR.

 XML Download
XML Download