

 PDF
PDF ePub
ePub Citation
Citation Print
Print


Introduction
Enrofloxacin is undoubtedly one of the most prescribed antibacterial drugs in canine medicine. It possesses a broad antibacterial spectrum and an outstanding bactericidal activity. As fluoroquinolone, enrofloxacin targets selectively two important bacterial proteins: topoisomerase II or gyrase, and DNA topoisomerase IV. These interactions prevent modification of DNA topology, stabilizing its supercoiling, and, in this manner, stopping transcription. At low concentrations enrofloxacin exhibits a bacteriostatic effect, while at higher concentrations it becomes a bactericide and induces chromosome fragmentation, hindering bacterial resistance mechanisms [38]. Enrofloxacin has been recommended for the treatment of respiratory, dermatological, soft tissue, joint, and bone bacterial infections [28]. From a pharmacokinetic/pharmacodynamic (PK/PD) view point, optimal use of enrofloxacin is achieved if the dose regimen is designed to comply with concentration-dependent ratios [2028]. That is, the maximum serum concentration (CMAX) should peak at or above 10 to 12 times the value of the minimum inhibitory concentration (MIC) (CMAX ≥ 10–12 MIC), and/or the ratio of the area under the concentration vs. time curve (AUC0–24) divided by MIC should be equivalent or higher than 125 (AUC0–24/MIC ≥ 125) [1].
For many bacterial infections, the preferred PK/PD ratio appears to be obtainable with the common enrofloxacin dose recommendations for dogs, i.e., 5 to 20 mg/kg [21]. Yet, in some instances, absorption variability may impede attainment of the preferred ratios [3] e.g., when administering enrofloxacin orally with certain foods [33]. Additionally, lack of bioequivalence of pharmaceutical preparations may interfere with the appointed PK/PD target, as has been shown in some domestic species [343536]. In dogs, a 5% solution of enrofloxacin available for intramuscular (IM) injection (Baytril 5%; Bayer Animal Health, Mexico) has a pH of approximately 10.4. Such a pH is likely to cause an inflammatory reaction, influence absorption rate, and, consequently, the AUC and CMAX values. In such an event, PK/PD ratios may be below the desired levels for some diseases. Similarly, different qualities of tablet manufacturing and of the active principles utilized [9] may change oral bioavailability.
A new re-crystallized form of enrofloxacin, defined as hydrochloride-dihydrate (Enro-C) has been characterized [1523]. Enro-C shows considerably higher water solubility than the parent compound, and it has been shown to have superior bioavailability to that of the parent drug in broiler chickens [15], cows [19], and hamsters [5]. It has also been shown that Enro-C has greater tissue distribution than that of enrofloxacin [5]. Additionally, it produces a more neutral pH when dissolved (pH 6.2–6.8) [23].
The MIC reported for enrofloxacin vs. Leptospira spp. ranges from a low of 0.1–0.5 µg/mL [18] up to 1–4 µg/mL [22]. The CMAX concentration values reported for the reference enrofloxacin (Enro-R) from Baytril 5% solution fluctuate between 1.12 µg/mL [8] and 1.4 µg/mL [16], and its AUC0–24 has been reported to fluctuate between 4.46 µg/mL/h [3] and 8.74 µg/mL/h [16]. Considering the preferred ideal PK/PD ratio, it is understandable that enrofloxacin has not been recommended for the treatment of leptospirosis in dogs, explaining why only a few evaluations of Leptospira spp. in vitro sensitivity to enrofloxacin have been reported [1822].
Considering the above, the impetus of this study was to assess whether higher values of CMAX and AUC could be obtained with Enro-C in dogs and to carry out Monte Carlo simulations utilizing the available data on Leptospira spp. susceptibility in vitro to enrofloxacin. To this end, comparative PK studies in dogs were carried out between a hard gelatin capsule and a 5% injectable water suspension containing Enro-C against the reference tablet and a 5% solution of enrofloxacin.
Materials and Methods
Animals
All study procedures and animal care activities were conducted in accordance with the Institutional Committee of Research, Care and Use of Experimental Animals of the National Autonomous University of Mexico (UNAM), according to Mexican Official Regulation NOM-062-ZOO-1999 (1999). A group of 32 healthy dogs was made available from volunteer owners. All dogs were regarded as healthy, based on physical examination, complete blood count, and serum chemistry panel results prior to the study. The dogs were 3 to 5 years old, of both sexes, and included the following breeds (mean body weights): twelve mongrel dogs (15.3 ± 5.2 kg), three Golden Retrievers (32.3 ± 3.1 kg), two German Shepherds (34.0 and 32.4 kg), three Boxers (28.2 ± 2.5 kg), three Cocker Spaniels (15.2 ± 2.4 kg), two Schnauzers (14.8 and 16.4 kg), three Dobermans (38.0 ± 42.1 kg), one Border Terrier (5.5 kg), one Airedale Terrier (22.0 kg), one Collie (24.3 kg), and one Dalmatian (18.2 kg). Dogs were block-randomized by age and breed, assigning dogs as homogeneously as possible into four groups of 8 animals each; two for oral administration of the drug and two for IM injection of the antibacterial drug. The IM groups were formed as follows: Enro-RIM group received an IM injection of 10 mg/kg of the Enro-R (Baytril 5% solution), whereas the Enro-CIM received a single 10 mg/kg IM dose of Enro-C as a 5% suspension readily made with injectable water on the spot. The chosen injection site was either in the semitendinosus or the semimembranosus muscles, and half the dose-volume was injected into each leg. Total dose volumes ranged from 2.4 to 6.5 mL. The oral-dosing groups were: Enro-Roral group received a tablet of the reference preparation from Baytril 50 or 150 mg tablets (Bayer Animal Health), adjusting the dose to each animal's weight by scraping the tablet just before its administration to obtain a dose level of 10 mg/kg. The experimental group of Enro-Coral, received the same dose of Enro-C but the drug was weighed and then included in a gelatin capsule. Each capsule or tablet was manually administered, without food, by placing it at the back of the mouth and forcing dogs to swallow. Water was freely available and food was allowed 1 h after treatment.
Enro-C preparation
A batch of re-crystallized enrofloxacin was prepared as reported in the product patent (Mexico/Instituto Mexicano de Protección Industrial: IMPI MX/a/2013/014605 and PCT/Mx/2014/00192). That process yields enrofloxacin hydrochloride-dihydrate, identified as Enro-C. Enrofloxacin with 99.97% purity was purchased from Globe Chemicals (Mexico).
Pharmacokinetic set-up
In order to achieve a close timing interval between administration of the drug and blood sampling from the radial vein, a permanent, heparinized, 10 cm long, 20 gauge catheter (BD, Mexico) was placed in each dog's radial vein and an Elizabethan collar prevented the dogs from reaching the catheter. Blood samples (3 mL) were withdrawn and collected after discarding the first 2 mL of heparinized blood. Basal blood sampling before medication was performed in each dog with further sampling at fixed times: 0.25, 0.5, 1, 1.5, 2, 4, 8, 12, and 24 h after dosing of the drug preparation. Blood samples were immediately centrifuged at 3,000 × g for 10 min, after which the plasma was recovered, identified, and frozen in liquid nitrogen until analyzed.
Quantification of enrofloxacin
The method of enrofloxacin quantification in plasma samples was developed and validated in our laboratory and was based on the method described by Idowu and Peggins [17]. An aliquot (1 mL) of plasma was added to 1 mL of methylene chloride and, after shaking the mixture for no more than 10 sec on a vortex mixer, it was centrifuged for 5 min at 11,200 × g. The supernatant was discarded and the organic phase was evaporated in a nitrogen environment. Residues were reconstituted in acetonitrile:methanol:water (17:3:80), with phosphoric acid (4% v/v) and trimethylamine (4% v/v) as the mobile phase. This product was then analyzed by high-performance liquid chromatography (HPLC) with fluorometric detection at λ = 280 nm. A Jasco XLC HPLC system (LC-2000Plus; Jasco Benelux, the Netherlands) with a Symmetry-C18 column (4.6 mm × 100 mm, 3.5 µm; Waters, USA) was used. Injection volume was 50 µL and flow was 0.6 mL/min. Data were analyzed by using Empower 3 from Waters (Mexico). The chromatographic method was validated, and the analytical procedure was demonstrated as specific. The method produced a linear result from 0.01 to 20.48 µg/mL (r2 = 0.984; y = 500030x − 107046). Recovery of enrofloxacin was calculated by applying linear regression analysis. Samples had an r2 = 0.978 (y = 0.072322309x + 0.1233375). Precision was demonstrated by the inter-day coefficient of variance (< 3.1) and inter-assay error value (< 3.9). The quantification limit for enrofloxacin in plasma was 0.01 µg/mL with a detection limit of 0.008 µg/mL. For robustness and tolerance, an absolute difference of 1.8 and a coefficient of variance of 2.2% (< 3.0%) were obtained.
Determination of MICs (MIC50 and MIC90)
Seven MIC studies of equal numbers of bacterial isolates obtained from clinical cases from January 2012 to December 2016 at the Veterinary School of the UNAM were incorporated into a composite database. All organisms studied in this experiment were subcultured twice on 5% sheep blood Colombia agar (35℃ for 16–18 h) prior to MIC testing. Leptospira spp. microorganisms were maintained by continuous culture in Ellinghausen McCullough Johnson Harris (EMJH) medium (BD) and were evaluated by applying the broth microdilution and macrodilution susceptibility tests as described by Murray and Hospenthal [26]. Broth microdilution testing was performed with microtiter plates; each plate included positive controls (bacteria without an antimicrobial), negative controls (medium only), and serial two-fold dilutions of enrofloxacin ranging from 25.0 to 0.01 µg/mL and the Leptospira spp. inoculum in amount of 100 µL (2 × 106 microorganisms/mL). The plates were incubated at 30℃. After 3 days of incubation, 20 µL of AlamarBlue were added to all wells. On the fifth day of incubation, the MIC value was recorded. The macrodilution antimicrobial-containing tubes were prepared to contain serial two-fold dilutions of enrofloxacin in Leptospira Medium Base EMJH medium in final concentrations of 0.01 to 20 µg/mL. Leptospira spp. inoculum was added to each tube to a final concentration of 106 microorganisms/mL (final volume, 2 mL). Then, the tubes were incubated at 30℃ for 7 days. The drug concentration contained in the lowest concentration tube without visual growth was recorded as the MIC90 [10]. For both methods, the quality control strain was Leptospira interrogans ATCC 56601. Cumulative efficacy is derived from the MIC50 and MIC90, the concentrations at which 50% and 90% of the leptospiral isolates are inhibited. To obtain the total composite MIC50 and MIC90 values derived from our studies and the ones collected from formal literature, a retrospective review based on various databases (Web of Knowledge, Web of Science, MEDLINE, Biological Abstract, Biological Science, ProQuest, and others) was carried out using enrofloxacin and Leptospira spp. as literature search descriptors. Only data referring to Leptospira spp. from a canine origin were selected.
Pharmacokinetics and Monte Carlo simulations
Compartmental and non-compartmental PK modeling were performed with PKAnalyst (MicroMath Scientific Software, USA) and Phoenix WinNonlin (Certara, USA) softwares, respectively. Pharmacokinetic parameters obtained by either of these methods were almost identical for each chemical form of enrofloxacin and after either administration route. Considering that the primary requirement of this trial was to determine the degree of exposure to enrofloxacin following administration of both forms of the antibacterial drug, results from the non-compartmental analysis are presented.
Key PK data from the four groups in this trial (Enro-RIM, Enro-CIM, Enro-Roral, and Enro-Coral) were subjected to Monte Carlo simulations based on the target attainments of CMAX/MIC = 10 and AUC0–24/MIC ≥ 125, as functions of optimal serum bactericidal concentration obtained by means of Phoenix WinNonlin software, simulating 10,000 subjects for each pharmaceutical preparation. The estimated parameters obtained from the population PK analysis were used to obtain unbiased target attainment rates (TARs; CMAX/MIC and AUC0–24/MIC), which are expressed as the percentage of the population reaching or exceeding the specific target. The TARs were then compared with the MIC distributions of the pooled survey on Leptospira spp. susceptibility to enrofloxacin.
Results
Fig. 1 shows the serum profiles of enrofloxacin after IM and oral administrations of either chemical form of enrofloxacin; i.e., the reference tablet and solution preparations of Enro-R and the capsules or injectable suspension of Enro-C. The estimated PK parameter values for the four groups included in this trial are presented in Table 1. The data did not exhibit a normal distribution; hence, data are presented as mean ± SD of 8 observations for each parameter, and, for statistical comparisons of pharmacokinetics variables among groups, the Kruskal-Wallis and Dunn tests were used. Table 1 also indicates the statistically significant differences among the four groups.
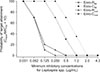
The key parameter values for the concentration-dependent antibacterial drugs were: CMAX after oral administration 1.47 ± 0.19 µg/mL and 5.3 ± 0.84 µg/mL for Enro-Roral and Enro-Coral, respectively (p < 0.05), and 1.63 ± 0.12 µg/mL and 7.6 ± 0.93 µg/mL after Enro-RIM and Enro-CIM administration, respectively (p < 0.05). Areas under the plasma vs. time concentration curve in 24 h (AUC0–24) were 8.02 µg/mL/h and 36.2 µg/mL/h for Enro-Roral and Enro-Coral, respectively (p < 0.05), and 8.55 µg/mL/h and 56.4 µg/mL/h after Enro-RIM and Enro-CIM administration, respectively (p < 0.05). Also, Table 1 shows the key PK/PD ratios, i.e., CMAX/MIC50, CMAX/MIC90 and AUC0–24/MIC50, AUC0–24/MIC90, considering the composite MIC50 and MIC90 values derived from the data summarized in Table 2, in which MIC values for enrofloxacin were obtained from a small survey of isolates obtained from infections in dogs with Leptospira spp. and from a review of formal reports. Monte Carlo simulation results are depicted in Fig. 2 where the probability of target attainment (CMAX/MIC50 = 10) for the two chemical forms of enrofloxacin and the two administration routes (all dosed at a rate of 10 mg/kg) are presented against the composite MIC values found for Leptospira spp. Other Monte Carlo simulation results, i.e., for AUC0–24/MIC50 are redundant and are not presented. After administration of an oral dose of 10 mg/kg of Enro-C, the TAR in plasma was high, with values of more than 70% TAR at MIC ≤ 0.25 µg/mL. Even better, for Enro-CIM TAR value was higher, with values of more than 70% TAR at MIC ≤ 0.5 µg/mL. Both these rates were significantly higher than the corresponding TAR values of Enro-RIM and Enro-Roral, which produced 70% TAR at MIC = 0.02 µg/mL, in both cases.
Discussion
The physicochemical characteristics of Enro-C include higher water solubility than that of the parent molecule [1523]. Yet, this feature was insufficient for the preparation of a 5% injectable solution of Enro-C. Therefore, a 5% water suspension was made on the spot for IM administration. In addition, hard gelatin capsules containing Enro-C powder were tested in this study. It is likely that these two preparations require a longer dissolution time in body fluids, compared to that of the reference pharmaceutical preparations of Baytril, and, in turn, this may account for the slower absorption rate and consequently the longer time to reach CMAX (TMAX) value for the oral and IM administrations of Enro-C. However, CMAX was noticeably higher with either preparation of Enro-C when compared to the values obtained for the Enro-R preparations (Table 1). This could be linked to the improved water solubility of the solvate, considering that enrofloxacin is almost insoluble in water. The CMAX value of Enro-C was 3.6 times higher than the corresponding value of the Enro-R. There is no clear explanation for these differences in CMAX, and, as stated, a rapid absorption of Enro-C is ruled out. Nevertheless, the CMAX values together with the higher AUC values for Enro-C confirm better bioavailability of the solvate in other species. High CMAX values for Enro-C have been shown after oral administration in broiler chickens [15] and after IM administration in hamsters [5]. In addition, plasma CMAX values observed after intramammary administration of Enro-C in cows were notably high [19]. Mean residence time also indicates longer residence of enrofloxacin in the body of dogs, when administered as Enro-C, compared to that for the reference preparation. This may also be related to a slow absorption rate and longer elimination half-life value of Enro-C compared to that for the Enro-R (3.8 h vs. 2.4 h). In contrast, elimination half-life (T½β) values found for the Enro-R ranged from 2.2 to 2.4 h, and these values are in agreement with others reported previously [38]. Due to the physiochemical characteristics of Enro-C, the intravenous administration of this solvate was not attempted, and therefore, an appropriate value for the apparent volume of distribution was not calculated. However, it is interesting to note that the area under the curve (AUC0–∞) was considerably higher in the Enro-C group than in the Enro-R one after oral administration (8.4 µg/h2/mL vs. 42 µg/h2/mL). Values of AUC0–∞ can be utilized to assess the extent of the distribution of a drug at a steady state. Hence, values found for Enro-C suggest a comparatively better distribution of this drug outside the central compartment. This feature is of particular importance in the treatment of leptospirosis when the leptospiremia phase has faded.
As reported previously, it is accepted, in general, that optimal PK/PD ratios for enrofloxacin are CMAX/MIC ≥ 10–12 and/or AUC0–24/MIC ≥ 125 [2028]. Based on the ratios obtained in this study for Enro-C (Table 1), it is possible to expect a certain degree of clinical efficacy in patients suffering leptospirosis caused by a relatively sensitive microorganism (MIC50 = 0.5 µg/mL). That is, CMAX/MIC50 values of 10.6 and 15.2 for oral and IM administration of Enro-C, respectively. However, if the patient's disease is caused by a less sensitive microorganism (MIC90 = 1.0 µg/mL), efficacy would be slightly less satisfactory, and daily IM administration of Enro-C would appear necessary (CMAX/MIC90 = 7.6). In any event, this is the first report showing that enrofloxacin, based on its PK/PD ratios and in an Enro-C solvate form, can be of use when treating leptospirosis. Kim et al. [18] found susceptibility patterns for Leptospira canicola, Leptospira grippotyphosa, Leptospira icterohemorrhagiae, and Leptospira pomona ranged from 0.05 to 0.39 µg/mL. In such infections, efficacy of Enro-C to treat this disease is more likely to be successful. Susceptibility values obtained in this study are in agreement with the MIC reported by Miraglia et al. [22]. Nevertheless, a clear-cut consensus on Leptospira spp. in vitro susceptibility to enrofloxacin is still lacking.
To the best of our knowledge, there are no previous reports describing the utilization of enrofloxacin or other fluoroquinolones to treat leptospirosis in dogs. Apparently, enrofloxacin from Enro-R has an insufficient CMAX and, consequently, has insufficient tissue distribution to reach the necessary concentrations for a favorable bactericidal action against Leptospira sp. Other fluoroquinolone derivatives produce similar results in clinical trials. For example, ciprofloxacin therapy in a hamster model of leptospirosis, resulted in survival rates of 90% when given at 50 mg/kg/day and 60% when given at 25 mg/kg/day, whereas all animals treated with 5 mg/kg/day of ciprofloxacin died prior to the end of the study. However, daily doses of 25 and 50 mg/kg of ciprofloxacin, were accompanied by severe/lethal drug reactions [14]. Gatifloxacin, another potent fluoroquinolone molecule, achieved a 60% survival rate in hamsters at a dose of 50 mg/kg/day. Again, severe antibiotic-associated diarrhea was observed in all treated animals [24]. In contrast, Enro-C administered IM at 10 mg/kg, also in a hamster model of leptospirosis, resulted in almost complete protection without adverse side effects [6]. Enro-C is a solvate of enrofloxacin [23] and, therefore, a close derivative. Nevertheless, the remarkable efficacy of Enro-C compared to the null efficacy of enrofloxacin, as in the reference preparation, is noteworthy.
No standard method for assessing the in vitro activity against Leptospira spp. is currently accepted, and laboratories do not routinely culture leptospires because of their very slow growth rate and the need for an expert in the field [2729]. Hence, a meta-analysis of susceptibility patterns or breakpoint data for enrofloxacin vs. Leptospira sp. cannot be performed. Thus, to accomplish the Monte Carlo simulations with enrofloxacin and Enro-C in this study, a small-scale survey of MIC values of Leptospira spp., pooled with values reported in the few studies available, is presented as a composite of MIC50 and MIC90 data. Hence, If MIC values for both chemical forms of enrofloxacin are assumed identical, a difference in clinical efficacy can be predicted based on PK/PD ratios (451% and 660% for the oral and IM administrations of Enro-C). This prediction merits a controlled clinical trial. Also, Monte Carlo simulations clearly depict differences when comparing the probability of target attainment for Enro-R vs. Enro-C (CMAX/MIC50 = 10) and considering the composite MIC values for Leptospira sp. set for this study. In general, these simulations suggest the potential for good clinical efficacy of Enro-C in the treatment of leptospirosis when in vitro sensitivity of the bacteria is ≤ 1.0 µg/mL. In this context, it is important to note that it is not uncommon to obtain better pharmacokinetics with a re-crystallized polymorph derivative of an active principle [73039]; for example, rifaximin-α, a crystal polymorph, is much more bioavailable than the parent molecule [4]. In spite of the above, the PK/PD and Monte Carlo simulations obtained herein advocate for a fully controlled trial to characterize the efficacy of Enro-C to treat leptospirosis. Also, considering that leptospirosis is probably the world's most widespread zoonosis [29], clinical efficacy against leptospirosis should also be assessed in other species, e.g., cattle. Clinical trials are mandatory, given that the clinical scenarios of this disease in dogs are bound to be diverse. For example, pharmacological interventions during the first stages of leptospiremia are rare, due to the inherent difficulties of an early diagnosis [229].
The clinical value of these results may be weighed against a broader perspective if the few chemotherapeutic options for treating leptospirosis in dogs are considered. Administrations of penicillin and other beta-lactam antibiotics, such as cefotaxime, require close compliance with very precise dosing schemes [25]. For example, administration of cefotaxime is preferred at the beginning of the disease, and high doses of the drug are mandatory, as well as short dose-intervals for longer periods. All such features can compromise compliance [1213]. A study in humans revealed that if antibiotics are delayed by 7 days after presentation of this disease, there is no longer an advantage in their administration [11]. The use of oral doxycycline for 21 days has been described as the most effective dosing scheme [37]; however, it is often related to severe adverse gastrointestinal effects such as irritant gastritis, vomiting, esophagitis, diarrhea, and depression. Eventually, these adverse reactions lead to rejection of this medication [13].
In conclusion, given that leptospirosis is a zoonotic disease with a worldwide distribution and can affect most mammalian species, research on new and more effective treatments is imperative, not only from an animal health viewpoint but also from a public health perspective [3132]. Our PK/PD and Monte Carlo simulation results for Enro-C in dogs indicate that its administration at a dose of 10 mg/kg, mainly through the IM route and in some cases orally, can be an important option for the treatment of this disease [56].



 XML Download
XML Download