

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Although emphysematous infections are well-known disease entities, emphysematous osteomyelitis has rarely been reported since intraosseous gas was first described as a sign of osteomyelitis 1981 [1]. Hematogenous or contiguous spread has been proposed as a mechanism in the development of emphysematous osteomyelitis, and vertebral bone involvement has been observed in almost half of the reported cases, including two recent ones [234]. In addition, various causative organisms, such as Klebsiella pneumoniae and Fusobacterium necrophorum, were identified in patients with significant underlying comorbidities, particularly diabetes mellitus [2]. Although emphysematous osteomyelitis is a rare disease entity, aggressive antimicrobial and surgical intervention should be considered because of its serious morbidity and mortality [56].
There has been one report of emphysematous osteomyelitis that was complicated by K. pneumoniae liver abscess [5]. However, other systemic metastatic infections such as septic pneumonia and cerebral septic emboli were not observed in previous reports of emphysematous osteomyelitis caused by K. pneumoniae [35]. Here, we report a case of rapidly fatal emphysematous osteomyelitis complicated by multiple systemic septic emboli and liver abscesses caused by K. pneumoniae.
Go to : 
Case report
A 79-year-old woman who had a 2-year history of diabetes mellitus and hypertension controlled with oral hypoglycemic and antihypertensive agents presented to the hospital due to altered mental status on the day of admission. The patient did not have any medical history, nor did she have a history of alcohol consumption and smoking.
On physical examination, body temperature was 36.0°C, blood pressure was 68/40 mmHg, pulse rate was 100 beats/min, and respiration was 22 breaths/min. The initial mental status was assessed as semicomatose, and auscultation of her lungs revealed coarse crackles throughout bilaterally. A chest radiograph showed cardiomegaly and bilateral patchy consolidations. Arterial blood gas analysis revealed a pH of 7.23, carbon dioxide tension of 14 mmHg, partial pressure of oxygen of 76 mmHg, bicarbonate level of 9.9 mmol/L, base excess of 19.1 mmol/L, oxygen saturation level of 92%, and lactic acid level of 12.0 mmol/L. Increased levels of serum ketones (1.3 mmol/L) and blood sugar (691 mg/dL) with elevated hemoglobin A1c (8.2%) were also observed. Initial laboratory findings revealed a hemoglobin level of 12.4 g/dL, white blood cell count of 25,240 /mm3 (neutrophils, 92.3%), platelet count of 11,000/mm3, blood urea nitrogen level of 105.0 mg/dL, creatinine level of 2.32 mg/dL, and C-reactive protein level of 22.95 mg/L (normal range, 0.0-5.0 mg/L).
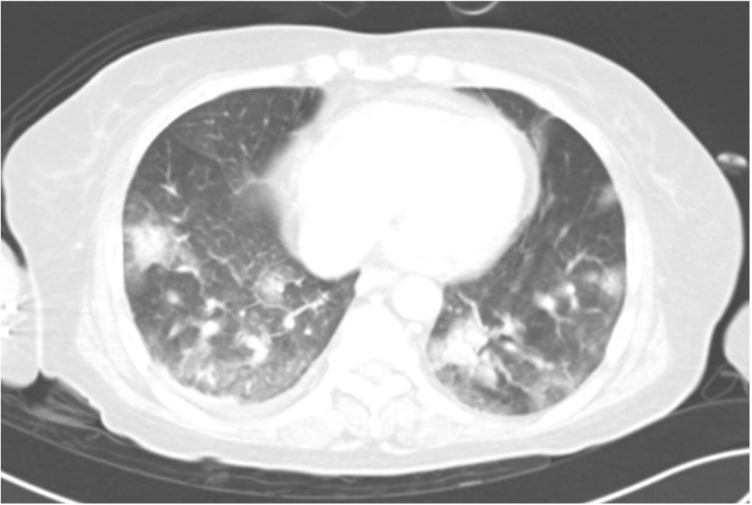
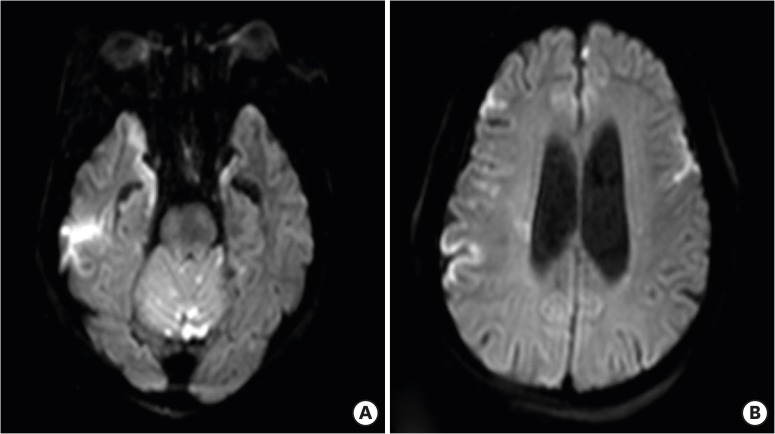
Abdominopelvic computed tomography (CT) with enhancement revealed extensive intraosseous gas, which extended from the fifth lumbar (L) spine to the sacrum (S), indicative of emphysematous osteomyelitis (Fig. 1). In addition, gas-containing abscesses were observed in the epidural space (L3-S5), soft tissue, and muscles in the adjacent sacrum and L5 vertebrae (Fig. 2). CT findings also confirmed two liver abscesses (sizes of 3 cm and 2.2 cm, respectively) (Fig. 3) Systemic septic emboli, such as multiple septic pulmonary emboli and multifocal cerebral embolic infarctions, were observed on CT and magnetic resonance imaging (Fig. 4 and Fig. 5).
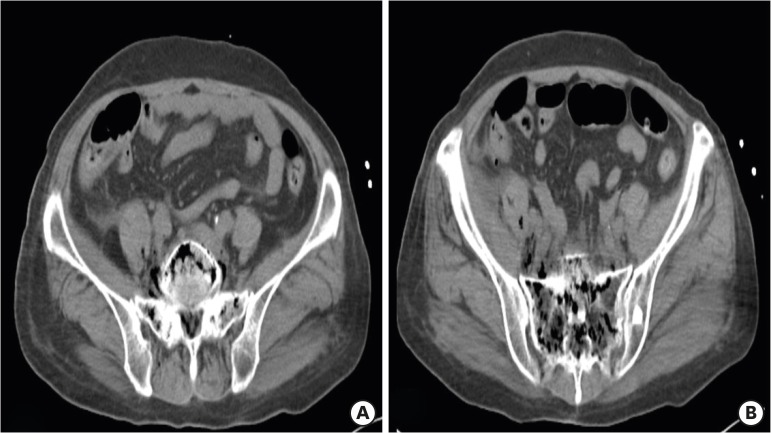 | Figure 1Non-enhanced abdominopelvic computed tomography demonstrates emphysematous osteomyelitis of L5 and the sacrum (A, B).
|
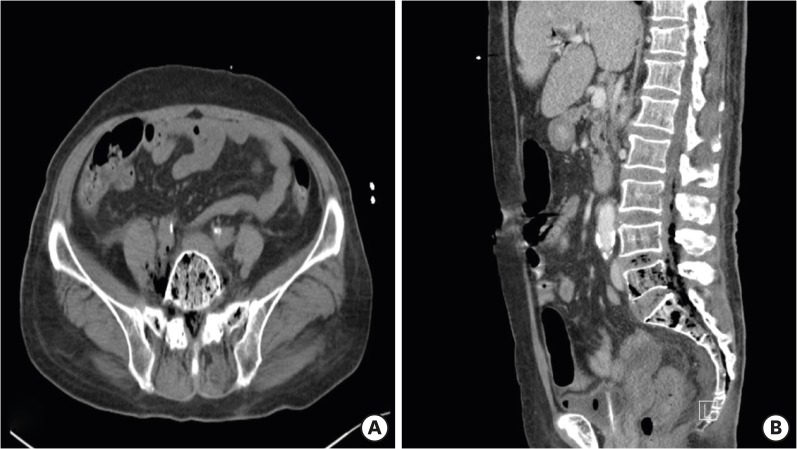 | Figure 2Axial (A) and sagittal (B) abdominopelvic computed tomography images show multiple air bubbles within the epidural space (L3-S5), retroperitoneum, paravertebral muscles, and right psoas muscle.
|
 | Figure 3Contrast-enhanced abdominopelvic computed tomography shows Klebsiella pneumoniae abscesses (arrows) in the right hepatic dome.
|
The patient was treated for presumed septic shock with diabetic ketoacidosis with intravenous ceftriaxone 2 g every 12 hours and metronidazole 500 mg every 8 hours. Although we initially planned urgent surgical decompression to release pus from the epidural and pelvic abscesses, aggressive surgical intervention could not be performed, because refractory shock and severe acidosis (serum lactic acid level, 15.0 mmol/L) developed rapidly. Despite the urgent addition of clindamycin and intravenous inotropic agents to meropenem without delay, the patient died of multiorgan failure from septic shock, 19 hours after admission.
After the patient died, on the second day after admission, two sets of blood cultures taken upon admission tested positive for gram-negative bacilli. On the third day, blood cultures showed non-resistant K. pneumoniae, susceptible to cefazolin, ceftriaxone, and ciprofloxacin on the standard disk diffusion method.
Go to :
Discussion
In this case report, we describe a case of extensive emphysematous osteomyelitis, which extended from the lumbar spine to the sacrum with involvement of the adjacent soft tissue and epidural infection, and complicated by systemic septic emboli and liver abscesses. The causative organism was K. pneumoniae. To the best of our knowledge, this is the first case report of emphysematous osteomyelitis accompanied by systemic metastatic infections via hematogenous spread from K. pneumoniae liver abscess.
Although emphysematous osteomyelitis is a rare disease, it is a life-threatening infection with high rate of mortality (32%), as one recent report suggested [2]. Emphysematous osteomyelitis is commonly located in vertebral bones, however, unusual locations such as tarsal bones are also reported [257]. Moreover, emphysematous infections of soft tissue and epidural space adjacent to bones have been described in previous reports [89]. Among several comorbidities that may predispose patients to the development of emphysematous osteomyelitis, diabetes mellitus is one of the most commonly associated diseases [2]. In our patient, immunosuppression related to diabetes mellitus may have influenced the development of emphysematous osteomyelitis along with adjacent infected tissues and poor treatment outcome.
K. pneumoniae has been reported as a causative organism of emphysematous osteomyelitis via hematogenous spread [35]. Invasive liver abscess syndrome, such as K. pneumoniae liver abscess with extrahepatic complications, may result in emphysematous osteomyelitis as a consequence of bacteremic dissemination [10]. It is noteworthy that diabetic patients with poor glycemic control, such as our patient, are well established to be a risk factor for gas formation as well as invasive syndrome and metastatic infections of K. pneumoniae [11121314]. In addition, patients with diabetes who show altered mental status accompanied by K. pneumoniae bacteremia should be evaluated promptly and treated with aggressive antibiotic therapy or surgical intervention, because of potentially poor outcomes even within 1 or 2 days of hospitalization [15].
Previous studies suggest that some K. pneumoniae strains possess pathogenic factors associated with invasive K. pneumoniae infections, such as the hypermucoviscous phenotype, K1 serotype, and the presence of the mucoviscosity-associated gene A (mag A) or regulator of mucoid phenotype A gene (rmp A) [161718]. K1 serotype K. pneumoniae, which has catastrophic complications and potentially poor prognosis, has already been reported to be prevalent in Korea [19]. Notably, diabetes mellitus is a significant risk factor for the K1 serotype K. pneumoniae liver abscess in Korean patients [20]. From our point of view, emphysematous osteomyelitis may be one of serious extrahepatic complications of invasive K. pneumoniae syndrome caused by the K1serotype, particularly if patients have diabetes mellitus. Our present report implies that clinicians should suspect K. pneumoniae, as a causative pathogen, when liver abscess and emphysematous osteomyelitis are observed in patients with diabetes. This may lead to an appropriate treatment approach and initial antibiotic therapy. Although we could not assess the presence of these pathogenic factors in our isolate of K. pneumoniae, we may presume that the patient in our case was infected by K. pneumoniae with hypermucoviscous phenotype associated with serotype K1. However, further studies to identify the molecular characteristics of the K. pneumoniae isolates in patients with emphysematous osteomyelitis would help clinicians have a lower threshold to suspect K. pneumoniae, as a causative organism for emphysematous osteomyelitis from liver abscess.
In conclusion, we present, to our knowledge, the first report of a patient with rapidly fatal emphysematous osteomyelitis caused by K. pneumoniae in Korea, which was complicated by extensive gas-containing abscesses in adjacent tissues and systemic septic emboli. Clinicians should suspect invasive K. pneumoniae syndrome, when confronted with liver abscess and concomitant intraosseous gas, particularly in patients with diabetes. Rapid diagnosis followed by aggressive antibiotic therapy and thorough surgical intervention may lead to successful management of this extremely challenging infectious disease.
Go to :
 XML Download
XML Download