

 PDF
PDF ePub
ePub Citation
Citation Print
Print



Introduction
Diabetic patients have a higher incidence of bacterial infections with increased morbidity and mortality [1234]. Urinary tract infection (UTI) is one of the most frequent infections among hospitalized as well as community-based patients with diabetes mellitus (DM). UTI in diabetic patients might present with more severe clinical course [567], tend to recur [8], and stay longer in hospital [9]. Despite certain predisposition to bacterial infection in diabetic patients, there are conflicting reports regarding the risk of UTI associated with hemoglobin A1c (HbA1c), blood glucose, and diabetic conditions [101112131415161718].
Till date, very little information exist regarding the impact of diabetes, glycemic control, and other clinical features on the clinical course of patients hospitalized for UTI. If there are some differences in this regard, identifying variables predictive of clinical outcomes will be feasible to better understand the clinical presentation and improve the current management of this patient population. Therefore, in the present study, we aimed to evaluate the clinical outcomes in association with clinical variables including the presence of DM, blood glucose, and HbA1c in hospitalized patients with febrile community-acquired UTI.
Materials and Methods
1. Study setting
A single-center, prospective observational study was conducted at Utsunomiya Memorial Hospital. Patients consecutively hospitalized for f-UTI between February 2016 and January 2018 were used for this study. The following laboratory tests were obtained on admission: complete blood count, blood chemistry including blood glucose, HbA1c, albumin, creatinine, blood urea nitrogen (BUN), estimated glomerular filtration ratio (eGFR), aspartate aminotransferase, alanine aminotransferase, alkali phosphatase, lactate dehydrogenase, total bilirubin and C-reactive protein, urinalysis and urine culture. Urine samples were collected using the clean-catch midstream method or urethral catheterization. Urine samples were placed on the blood agar and the deoxycholate-hydrogen sulfide-lactose agar and incubated under aerobically at 37°C. Urine samples showing a colony count more than 104 colony forming unit (cfu)/ml were considered as positive for UTI and microorganisms were identified using automated system VITEC2 (bioMèrieux inc, Durham, NC, USA). All patients received empiric treatment using parenteral antibiotics following the discretion of the attending doctor until susceptibility testing was available. The clinical course such as duration of fever (DOF) and length of hospital stay (LOS) were compared among groups classified by the clinical variables to know the underlying differences among them and how diabetic status affects the clinical course of patients hospitalized for f-UTI.
This study was conducted in accordance with the Helsinki Declaration and was approved by the ethical review board of Ustunomiya Memorial Hospital. Each patient signed a consent form that was approved by our institutional review board.
2. Definitions
Febrile UTI was defined as body temperature ≥38°C with pyuria (≥10 leukocytes/ high power field) in the absence of other infectious focus. Acute pyelonephritis was defined as f-UTI with lumbar tenderness or dirty fat sign around the kidney on computed tomography. Acute prostatitis was defined as f-UTI with lower urinary tract symptoms and tenderness by the digital rectal examination. Urine culture was considered positive for UTI when organisms were growing at a concentration of ≥105 cfu/ml. Patients were considered afebrile when body temperature remained below 37°C for more than 24 hours. Admission blood glucose (ABG) level was defined as the blood glucose level closest to the arrival time within 24 hours of the admission date. Patients were dichotomized by the median value of each clinical variable except for the cut-off of 140 mg/dl for ABG and 6.5% for HbA1c. Patients were also divided into three groups by diabetic status: those with known DM before hospitalization (DM group), those without known DM but with ABG ≥140 mg/dl (H group), and those without DM and with ABG <140 mg/dl (nDM group). Concurrent hydronephrosis caused by urolithiasis, urosepsis, and disseminated intravascular coagulopathy (DIC) were considered as risk factors for severe complicated infection.
3. Statistics
As collected data were not normally distributed, continuous variables compared two groups using the Mann-Whitney U test or the Kruskal-Wallis test for three groups. Intergroup comparison among three groups was performed by bonferroni correction. The case distribution for categorical variables were analyzed by the chi-square test or Fisher's exact test. The Kaplan-Meier curves were generated to estimate the probability of febrile condition and hospitalization as well as differences between the curves were assessed by the log rank test. Patients were regarded as having events at afebrile condition or hospital discharge and censored at death for this analysis. The Cox proportional hazard analysis was used to evaluate the impact of multiple variables on DOF and LOS. Data were expressed as median [interquartile range (IQR)]. P-value <0.05 was considered to be significant.
Results
1. Patients characteristics
A total of 101 patients (30 men and 71 women) with mean age of 77.7 ± 15.7 years were enrolled, of whom majority (69.3%) were not hyperglycemic on admission. Fifteen (14.9%) patients were presented with known diabetes (DM group), 18 (17.8%) with hyperglycemia (H group), and 68 (67.3%) without diabetes and hyperglycemia (nDM group). Thirty seven (36.6%) patients had any of the comorbidities of cardiovascular disease, cerebrovascular disease, chronic obstructive pulmonary disease, chronic renal failure, malignancies, and so forth other than DM and urolithiasis. Febrile UTI mostly consisted of pyelonephritis (n = 94, 93.1%) with a few exception of prostatitis (n = 4, 3.9%), epididymitis (n = 1, 1%), renal abscess (n = 1), and emphysematous cystitis (n = 1). Fourteen (13.8%) patients had obstructive urolithiasis, 5 of whom needed ureteral stenting during hospitalization. Eight (7.9%) patients showed signs of sepsis, DIC, or both, and were treated with concomitant recombinant human soluble thrombomodulin, immunoglobulin, or both. Overall, 18 (17.8%) patients had either of the risk factors which led to severe complicated infection.
2. Comparison of the patients' characteristics, laboratory parameters, and clinical course among the groups according to the diabetic status
Patients profile represented by age and the presence of comorbidity and risk factors for severe complicated infection were not different among the three groups according to the diabetic status. Of the tested laboratory parameters, ABG, HbA1c, BUN, and eGFR levels were significantly different by the diabetic status. HbA1c levels in diabetic patients were significantly higher than those in H group and nDM group (P < 0.0001). Patients in DM group showed significantly worse renal function indicated by BUN (P = 0.0066) and eGFR (P = 0.0440), but not by creatinine level (P = 0.0767) compared with the other two groups. Median DOF and LOS in all patients were 3.5 (IQR; 2-6) days and 8 (IQR: 7-12) days, respectively. Patients in DM group experienced significantly longer febrile periods (P = 0.0289) and hospitalization (P = 0.0330) compared with those in the other two groups (Table 1).
Table 1
Comparison of age, laboratory reults, duration of fever, and length of hospital stay according to the diabetic status
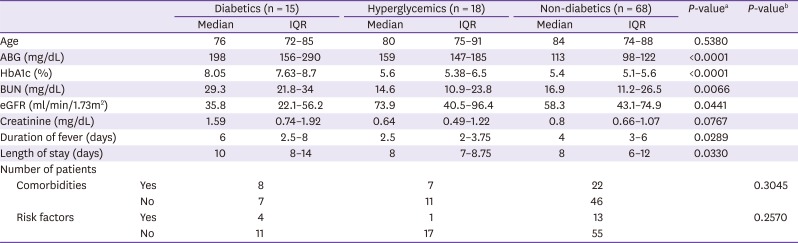
IQR, interquartile range; ABG, admission blood glucose; BUN, blood urea nitrogen; eGFR, estimated glomerular filtration rate.
Risk factors include hydronephrosis caused by urolithiasis, urosepsis, or disseminated intravascular coagulopathy.
aP-values were determined by the Kruskal-Wallis test.
bP-values were determined by the chi-square test or Fisher's exact test.
3. Comparison of the clinical course between the dichotomized groups according to the clinical variables
During the study period, two patients died of sepsis and one patient who had pneumonia subsequently were censored.
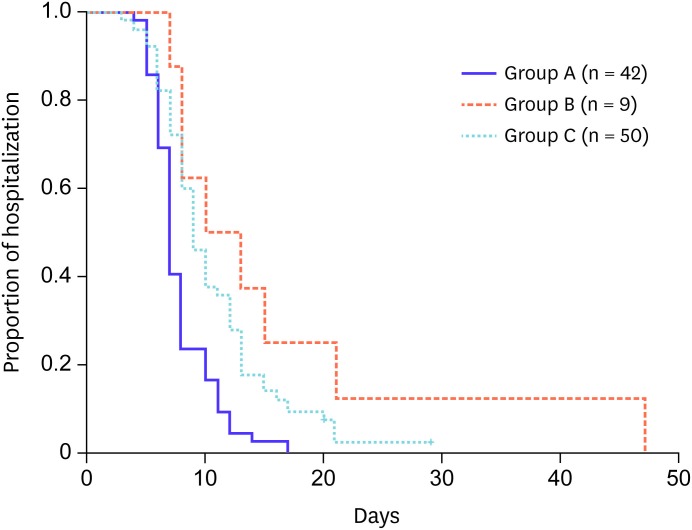
Of the laboratory parameters tested on admission and clinical factors including age, sex, presence of comorbidity or diabetes, and risk factors for severe complicated infection, the last two factors as well as HbA1c and albumin were identified as predictors for LOS by the univariate analysis, whereas none of the variables failed to predict DOF. In subsequent multivariate analysis, HbA1c and albumin were associated with LOS (Table 2). Figure 1 depicts Kaplan-Meier survival curves comparing the two groups dichotomized by the defined cut-off values for HbA1c or albumin. Patients with lower HbA1c (≤6.5%) or higher albumin level (>3.2 g/dl) had a shorter hospitalization period than their counterparts (P = 0.0185 and 0.0008, respectively). Since HbA1c and albumin were isolated as independent predictors of LOS, patients were classified into three groups according to the combined status of HbA1c and albumin; lower HbA1c and higher albumin (group A, n = 42), higher HbA1c and lower albumin (group B, n = 9), and both higher or lower (group C, n = 50). These categorized groups were significantly associated with LOS (P = 0.0002). The intergroup comparison revealed that patients in group A had a significantly shorter period of hospitalization compared with those in group B or C [median LOS of A, B, and C were 7, 11.5, and 9 days, and the pair-wise P-values were 0.0015 (A vs. B) and 0.0090 (A vs. C), respectively] (Fig 2).
Table 2
Significat variables predictive of length of hospital stay by univariate and multivariate analyses

Figure 1
Probability of hospital stay indicated by Kaplan-Meier curves according to HbA1c (A) or albumin (B) levels. Patients with higher HbA1c or lower albumin required longer hospitalization. Note that the lower curves represent better outcomes of shorter hospital stay as discharge from the hospital is counted as an event.
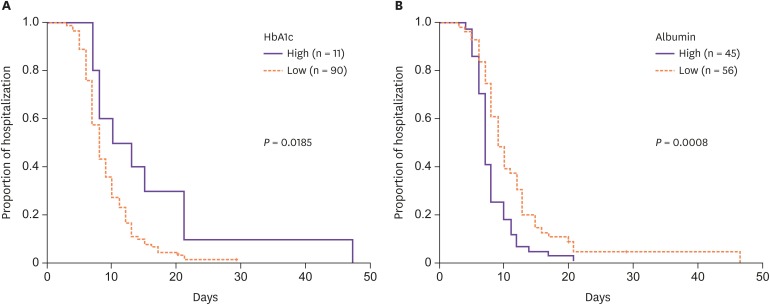
Figure 2
Probability of hospital stay indicated by Kaplan-Meier curves according to the combination of HbA1c and albumin levels.
group A: patients with lower HbA1c and higher albumin, group B: patients with higher HbA1c and lower albumin, group C: patients with both higher or lower albumin.
Patients in group A experienced the shortest hospital stay.
4. Difference in isolated microorganisms according to the glycemic status
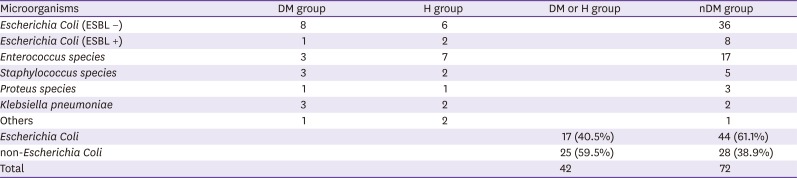
We thereafter investigated how glycemic conditions affected the etiology of isolated microorganisms. Detailed case distribution of isolated microorganisms according to the diabetic status was displayed in Table 3 (upper). To characterize the etiology of isolates by the glycemic status, patients were dichotomized into hyperglycemic group (DM and H groups) and normoglycemic group (nDM group), and microorganisms were dichotomized into Escherichia coli and non-E. coli. Patients with DM or hyperglycemia were more likely to have non-E. coli uropathogens compared with those without both. (P = 0.0328) (Table 3, lower).
Table 3
Distribution of isolarted microorganisms according to the diabetic status
Discussion
In the present study, we explored the impact of diabetes, glycemic control, and other clinical features on the clinical course of patients with community-acquired f-UTI. It was found that HbA1c and albumin levels at admission were identified as independent predictors for length of hospitalization. When patients were classified by their diabetic status based on known history of diabetes and admission blood glucose level, diabetic patients experienced significantly longer febrile period and hospitalization than those with hyperglycemia but without DM or those without both. The latter had less incidence of non-E. coli uropathogens compared with diabetic or hyperglycemic patients.
Previous studies indicated mixed results regarding the risk of symptomatic UTI associated with HbA1c, blood glucose, and diabetic conditions including its presence, duration, and complications. Some studies demonstrated significant associations between predisposition to UTI and HbA1c level or duration of diabetes [1011121314], while the others did not find meaningful associations between the incidence of UTI and HbA1c, blood glucose, or diabetic conditions [151617]. Collectively, the evidence for a causal relationship between UTI and glycemic status seems to be lacking. On the other hand, although it is widely held that diabetic patients are more likely to have a complicated course of infections, the information on how diabetic status affects the clinical course of patients hospitalized for established UTI is quite scarce. Horcajada et al. demonstrated that the duration of hospitalization was significantly longer in diabetics than in non-diabetic patients, although the duration of fever after therapy was similar in both groups [9]. Kim et. al also showed a longer period of hospitalization in diabetic than in non-diabetic women with acute pyelonephritis [19]. In contrast, van der Starre et. al reported that diabetes was not associated with a longer duration of fever or prolonged hospitalization [20]. In the present study, diabetic status was further classified into 3 groups according to known history of diabetes and ABG level, and their clinical course was compared. Diabetic patients experienced significantly longer febrile period and hospitalization compared with non-diabetics with or without hyperglycemia, suggesting that diabetic patients may need a longer time to recover from acute infection and regain the strength needed to leave the hospital. Inconsistent results regarding the relationship between diabetic status and clinical course may partly come from the difference in uropathogens between diabetics and non-diabetics. That is, previous studies including ours, in which a longer hospitalization in diabetics was indicated, demonstrated that non- E. coli and extended spectrum β-lactamase (ESBL) positive or fluoroquinolone resistant E. coli were more frequently isolated than in non-diabetics [919]. However, the only report by van der Starre, in which duration of fever and hospitalization were similar, did not mention the difference in uropathogens but showed that E. coli was the most common in both diabetics and non-diabetics [20]. Taken together, diabetics are more susceptible to complicated uropathogens and thus need a longer time for cure compared with non-diabetics. This is biologically plausible, given that diabetics have immunologic deficits such as impaired leukocyte function [21] and a lower pro-inflammatory cytokine production [22], and neuropathic complications that lead to incomplete emptying of the bladder [23].
Furthermore, it has been reported that elevated ABG level is associated with poor outcomes in patients with various acute conditions including stroke, myocardial infarction, heart failure, surgery, trauma, pneumonia, and pulmonary embolism [24252627282930]. Likewise, the recent study demonstrated that there was a significant association between ABG and short and long-term mortality in patients without DM, but not in patients with DM, hospitalized for UTI [18]. Elevated blood glucose in non-diabetics may be induced by acute infection in which several cytokines stimulate gluconeogenesis and increase insulin resistance as well as cortisol release [31]. Thus, it is assumed that ABG may have predictive value to short-term clinical course in patients hospitalized for UTI. However, ABG was not associated with DOF or LOS in patients without DM (data not shown) as well as in the whole patients.
The present study identified not only HbA1c, but also albumin as independent predictors for the clinical course of patients hospitalized for f-UTI. Combined use of these two predictors discriminate patients' clinical course more precisely. That is, patients with lower HbA1c and higher albumin experienced significantly shorter hospital stay than the others. In contrast, those with higher HbA1c and lower albumin needed the longest period of hospitalization. Low albumin level reflects not only malnutrition, but also underlying conditions such as nephrotic syndrome, enteropathies, and hepatic insufficiency, and also may occur in the setting of acute injury and illness [32]. Systemic inflammation decreases albumin synthesis but increases its degradation. Despite such various factors that affect albumin levels, some studies found that hypoalbuminemia was a risk factor related to the onset, complications, length of hospitalization and mortality caused by various infections [3334], as hypoalbuminemia causes deficient immunity in elderly patients, making them prone to infectious diseases [35].
The present study is limited by the relatively small number of patients from a single institution. Given the small subsets of patients for the proposed stratification on which the results are based, the statistical power may be insufficient to draw firm conclusion, and further confirmatory studies will be necessary to confirm the findings.
In conclusion, the present study suggests that poor nutrition and poor glycemic control may contribute to the vulnerability of patients to UTI and expose them to prolonged hospitalization. Thus, evaluation of HbA1c and albumin on first contact may provide accurate guidance to the physicians on which patients may run a complicated course and who may be safely treated. If attention is paid to the nutritional care of patients during hospital stay, hypo-nutrition on admission can be ameliorated, which may facilitate recovery from infections. Also, patients with diabetes or hyperglycemia were liable to have non-E. coli uropathogens, suggesting that they may develop more complicated infections and need early intensive treatments. Such approach will contribute to our understanding of the clinical and laboratory characteristics of infections and help to better treat patients suffering from f-UTI.
 XML Download
XML Download